
Abstract
Internal jugular vein (IJV) thrombosis is mainly related to central venous catheter, malignancy, and ovarian hyperstimulation syndrome. We report a case of IJV thrombosis possibly related to IJV compression between the styloid process and the first cervical vertebra (C1) transverse process. To support this hypothesis, we perform radiological assessment of the IJV and examine its relationship with the styloid process and C1 transverse process in 34 controls. Our results showed a strong correlation between IJV diameter and styloid process–C1 transverse process distance. Compared to control subjects, our patient had a short styloid process–C1 transverse process distance, which suggests its involvement in IJV thrombosis.
Introduction
Internal jugular vein (IJV) thrombosis is an uncommon entity accounting for 1.5% of deep vein thrombosis and 45.3% of upper extremity deep-vein thrombosis (UE-DVT). 1 Its main risk factors are central venous catheters, malignancy, and ovarian hyperstimulation syndrome. 1 The relevance of thrombophilia testing is unclear in IJV thrombosis 2 and no entrapment syndrome has been described to our knowledge. We report the first case of IJV thrombosis potentially related to venous compression between the styloid process and the C1 transverse process. We furthermore analyzed these anatomical relationships in 34 control subjects.
Clinical presentation
A 19-year-old man was evaluated because of acute facial edema secondary to acute IJV thrombosis. The patient had no medical history. He had been painting the ceiling for several hours 2 days earlier. Computed tomography (CT) angiography of the neck showed evidence of thrombosis of the left IJV extending 3 cm from the jugular foramen. This segment of the IJV was not accessible on venous duplex and could not be evaluated by this technique.
The laboratory workup revealed a normal full blood count, normal blood chemistry and C-reactive protein, and elevated D-dimer levels at 2900 ng/mL (N < 500 ng/mL). Additional laboratory findings showed absence of antithrombin, protein C and S deficiencies, absence of factor V Leiden and prothrombin gene mutations, absence of antiphospholipid antibodies, and a normal plasma homocysteine level. CT of the chest, abdomen, and pelvis showed no additional thrombosis, no tumor and no lymphadenopathy. Anticoagulation with rivaroxaban was started for this unprovoked IJV thrombosis.
CT angiography of the neck (Figure 1) repeated 8 months later, because of recurrence of facial edema, showed partial thrombus resolution and suggested compression of the left IJV between the left styloid process measuring 35 mm and C1 transverse process. The distance between the left styloid process and C1 transverse process was 3.9 mm (Figure 1C: M2). Retrospective review of the initial CT angiography confirmed this finding. After multidisciplinary discussion, a first line conservative approach with long-term anticoagulation was chosen, without surgical decompression.
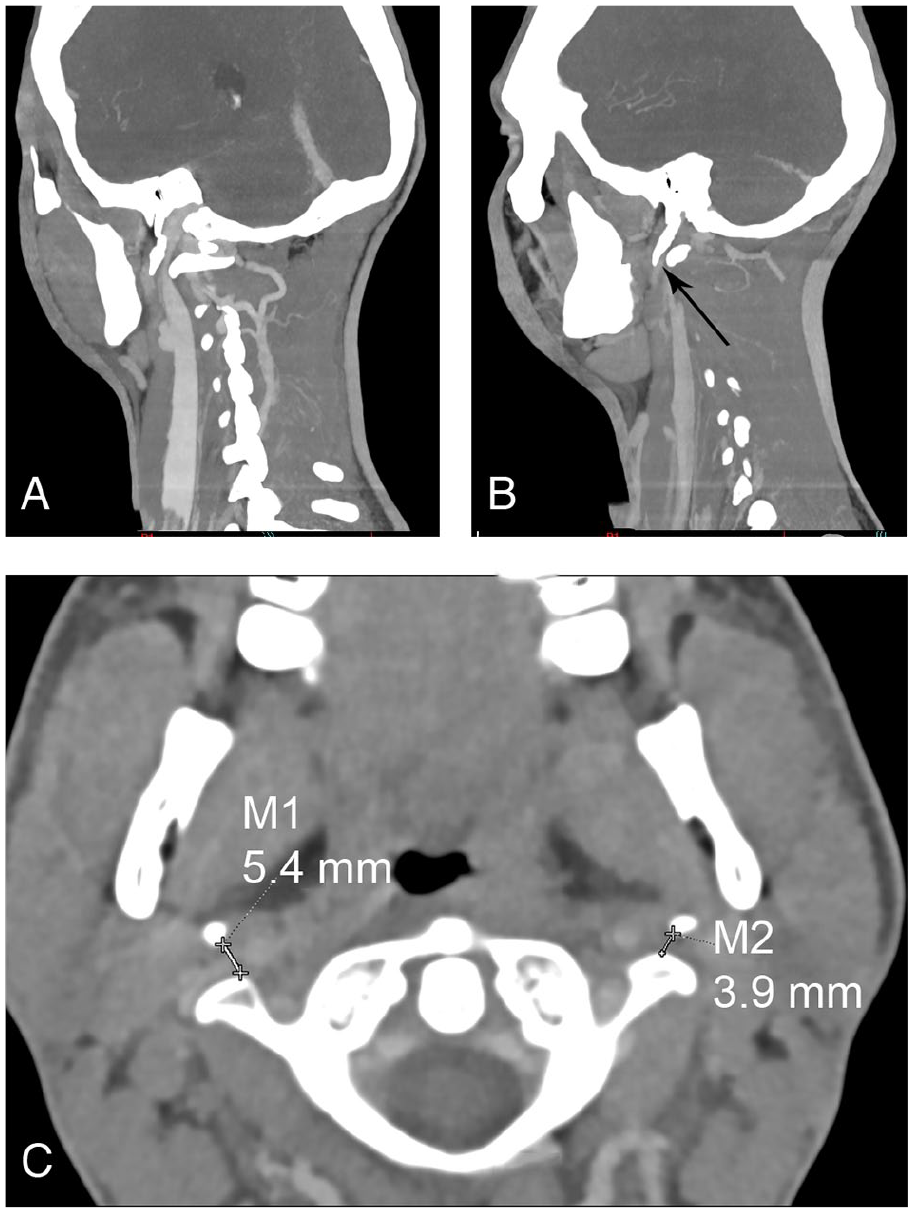
Cervical CT angiography in a male patient.
Comparison with control subjects
CT angiographies of 34 consecutive controls, consisting of 15 males with a mean age of 46.9 ± 17.7 years, who underwent a CT angiography of the head and neck for the evaluation of cellulitis or ENT cancer, were reviewed independently by a neuroradiologist (CD) and a vascular medicine physician (MRP). The following parameters were scored bilaterally: (i) the length of the styloid process defined as the distance from its tip to the flat surface on the side of the stylomastoid foramen; (ii) the minimum distance between the styloid process and the C1 transverse process; and (iii) the minimum diameter of the IJV (Figure 2). These parameters were described using median (interquartile range) and 10th and 90th percentiles. Correlation was assessed using Spearman’s test, in the absence of normality. All analyses were performed using R software (R Foundation for Statistical Computing, Vienna, Austria). French legislation on noninterventional studies requires collecting the non-opposition of patients but does not require written consent. As such, non-opposition was obtained from each patient included in the study for the use of their de-identified medical record data.
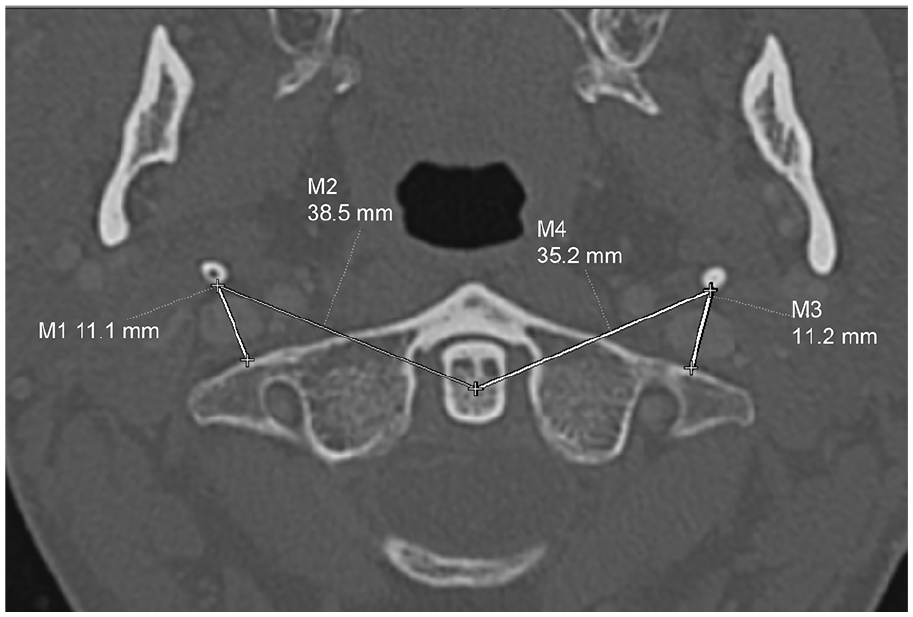
Axial CT angiography of a male control subject showing measured right (M1) and left (M3) styloid process–C1 transverse process distances.
None of the controls had past or acute IJV thrombosis. The median styloid length was 31 mm (IQR 24.4–36.3); 10th percentile was 20.9 mm and 90th percentile was 40.7 mm. The median styloid process–C1 transverse process distance was 9.0 mm (IQR 6.3–11.3); 10th percentile was 4.0 mm and 90th percentile was 12.6 mm. The median IJV diameter was 5.1 mm (IQR 3.5–6.7); 10th percentile was 2.4 mm and 90th percentile was 7.4 mm.
There was a strong positive correlation between IJV diameter and styloid process–C1 transverse process distance (ρ = 0.63, p < 0.001) and no correlation between IJV diameter and styloid process length (ρ = 0.08, p = 0.573).
Discussion
An elongated styloid process, as firstly reported by Eagle in 1937, can be involved in impingement of cranial nerves V, VII, IX, and X causing otalgia, pharyngeal pain, and foreign body sensation 3 and compression of the carotid arteries or sympathetic nerve fibers causing headache, facial, and neck pain. 4 More recently, the styloid process and the posterior belly of the digastric muscle have been reported to be the most common causes of asymptomatic jugular vein compression in 108 patients. 5 However, no venous thrombosis has been described in these patients and the relationship between the styloid process and C1 transverse process has not been evaluated.
Even in the setting of normal length styloid process, it has been reported that a narrowed distance between the styloid process and C1 transverse process may lead to IJV compression. 6 Hence, in our work, we decided to measure styloid process length and the distance between the styloid process and C1 transverse process. These parameters were also recently evaluated by Zhao et al. 7 , who described a novel clinical entity called styloidogenic jugular venous compression syndrome (SJVCS) whereby IJV compression between the transverse process of C1 and the styloid process causes intracranial hypertension and venous outflow reduction. Compared to patients with idiopathic intracranial hypertension, SJVCS patients had a significantly longer styloid process and a shorter distance between the styloid process and transverse process of C1.
In line with the findings of Zhao et al., 7 our analysis of 34 control subjects suggests the fact that a narrowed styloid process–C1 transverse process distance may cause IJV compression leading to impedance of venous outflow, which is a contributing factor in DVT, as in May–Thurner syndrome. 8 Indeed, there was a strong correlation between IJV diameter and styloid process–C1 transverse process distance. Compared to control subjects, our case patient had a short styloid process–C1 transverse process distance of 3.9 mm, which is below the 10th percentile, while the diameter of the IJV could not be measured because of thrombosis. In our patient, prolonged hyperextension of the neck during ceiling painting could have probably resulted in exacerbation of the left IJV compression and led to thrombus formation.
Although styloidectomy is the preferred treatment in most cases of Eagle syndrome with classic presentation or with carotid arteries compression, data are more limited in the case of symptomatic IJV compression.6,9,10 The recent work by Zhao et al. 7 suggests that decompression with a C1 tuberculectomy and styloidectomy in case of SJVCS could improve venous outflow. Further studies are needed to determine the optimal treatment strategy.
Conclusion
In the presence of unexplained IJV thrombosis, it might be of interest to search for IJV compression by evaluating the distance between the styloid process and C1 transverse process. Further studies are needed to confirm the relationship between IJV entrapment syndrome and venous thrombosis and to determine the optimal treatment strategy, especially the role of surgical decompression.
Footnotes
Acknowledgements
The authors wish to thank the patient for his consent and kind collaboration.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.