
Abstract

Keywords
Introduction
Superficial vein thrombosis (SVT), sometimes called superficial vein thrombophlebitis, refers to a blood clot that forms in one of the surface veins of the body. It is different from deep vein thrombosis (DVT), which occurs in veins deeper inside the body and which can have serious health consequences if not treated promptly with an anticoagulant medication, or ‘blood thinner’ (see Vascular Disease Patient Information Page: Venous thromboembolism 1 ). The term ‘phlebitis’ means inflammation of the vein, which may occur when there is no clot present, often in cases when a vein becomes irritated by physical trauma or after an intravenous line (IV). On physical examination, phlebitis may be indistinguishable from SVT. Although SVT typically is not life- or health-threatening, it is important for patients with the symptoms of SVT to be examined by a health care provider.
What is superficial vein thrombosis (SVT)?
SVT occurs when a blood clot, or thrombus, forms in one of the surface veins on the body, typically in the legs or arms, but occasionally on the chest or abdomen. The veins are the tubes that carry blood from the body back to the heart, and these veins are divided into ‘superficial’ and ‘deep’ veins. The superficial veins are closer to the skin surface, and they drain into the deep veins. In the legs, the superficial veins drain into the deep veins behind the knee and at the groin (Figure 1), and in the arms, the superficial veins drain into the deep veins at the upper arm and shoulder. The veins have a series of valves, which are small flaps of tissue that, when closed, prevent blood from flowing backward. When the muscles contract, they squeeze the veins and help the blood flow against gravity up toward the heart. SVT usually starts around these vein valves.
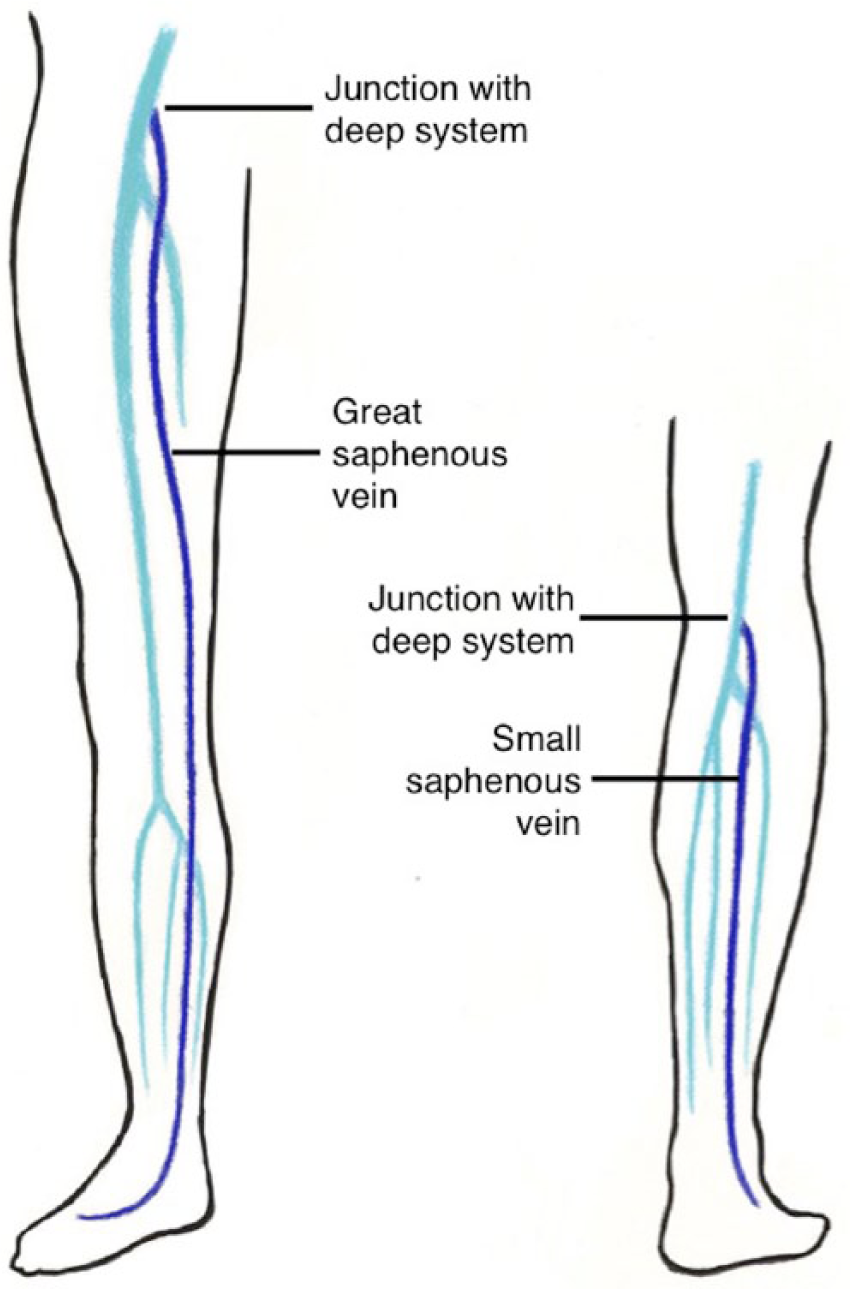
The main superficial veins of the leg are the great saphenous vein (also known as the GSV), which courses along the inside of the leg to meet the deep system in the groin, and the small saphenous vein (also known as the SSV), which runs along the back of the calf to meet the deep system behind the knee. There are many superficial veins throughout the legs and arms, which are not illustrated here.
Who is at risk for SVT?
The risk factors for SVT are similar to those for DVT. Patients who have had recent surgery within the past 1–3 months, medical illness with hospitalization or bed rest for longer than 3 days, or trauma to the arms or legs are at risk for thrombosis (blood clots). Pregnancy, recent childbirth, and hormones (including birth control pills and hormone replacement) all increase the risk. Patients with underlying tendencies to form blood clots, called hypercoagulable states or thrombophilias, are at risk for thrombosis. Cancer is a hypercoagulable state that can increase clotting risk. A common reason for developing SVT of the arm veins is a recent vein puncture to draw blood or insertion of an IV or catheter. Finally, patients with varicose veins – enlarged, ropy veins on the legs – are at risk for SVT.
What are the signs and symptoms of SVT?
Patients with SVT commonly have pain at the affected vein, which also may be warm, red, and tender to touch (Figure 2). The vein may feel hard or like a cord or knot. In some cases, the affected leg or arm may be swollen, especially if the SVT is extensive. In patients with varicose veins, leg pain or swelling should prompt suspicion for SVT.

The calf of this patient with superficial vein thrombosis is red, warm, and tender to the touch. A hard knot is felt under the skin.
How is SVT diagnosed?
In the past, SVT was most commonly diagnosed clinically – that is, with a physician’s physical examination in combination with suspicion for the condition. Now, it is usually diagnosed with ultrasound, which is a non-invasive test that uses sound waves to look at the blood vessels (see Vascular Disease Patient Information Page: The vascular laboratory 2 ). Sometimes called duplex or Doppler, this test creates pictures of the affected veins using a hand-held ultrasound probe (Figure 3). The probe, which is coated with gel that helps obtain better pictures, is run along the length of the veins. The ultrasound technologist who performs the test pushes on the veins to see whether they collapse normally. Veins do not collapse when they are filled with a blood clot. Having an ultrasound is important when a blood clot is suspected because sometimes blood clots form in the deep veins and in the superficial veins at the same time. It can be difficult to determine if a clot is superficial or deep on physical examination alone.
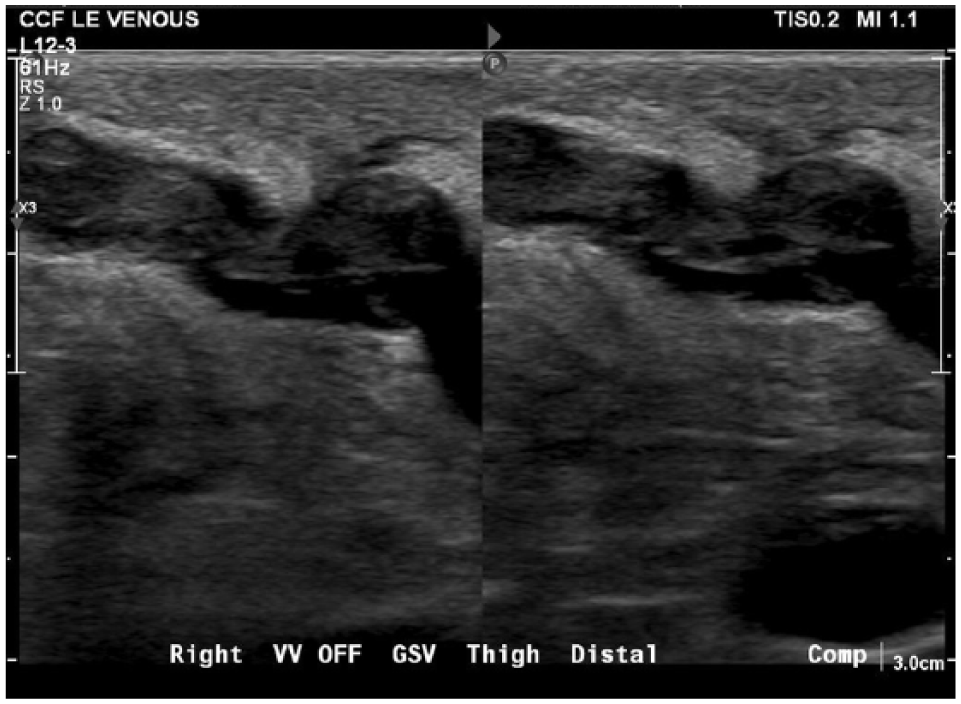
The left panel shows an enlarged varicose vein filled with clot (superficial vein thrombosis). The right panel shows that the thrombus-filled vein does not collapse with compression on the vein by the ultrasound probe.
Ultrasound uses no radiation and is typically painless, although pushing on the affected veins can sometimes be slightly uncomfortable. Occasionally, SVT may be found on tests like computed tomography (CT) scans or magnetic resonance imaging (MRIs) done to look for other problems. When a blood clot is diagnosed, age-appropriate cancer screening is often recommended (such as a mammogram or colonoscopy if it is overdue) and in some cases testing for other hypercoagulable states may be suggested.
How is SVT treated?
In most cases, SVT goes away on its own, and the focus of the treatment centers on relieving symptoms. The treating health care provider may recommend warm compresses and anti-inflammatory medications such as ibuprofen or diclofenac, either taken by mouth or as a gel put directly on the skin. For patients with SVT and swelling, raising the affected body part above the level of the heart can be helpful, as well as use of compression bandaging or elastic compression stockings.
When symptoms are severe or the clot is extensive, the health care provider may recommend an anticoagulant for several weeks to stop the clotting process and help the body resolve it faster. The anticoagulant may be a pill or a medication that is injected under the skin of the abdomen once a day.
When the SVT is within a few inches of joining with the deep vein system, an anticoagulant is also used to prevent the clot from extending into the deep veins, where it can break off and travel to the lungs, causing a serious condition called pulmonary embolism (PE). A study of patients with a SVT longer than 5 cm, or about 2 inches, showed that patients who got a low dose of an injected anticoagulant called fondaparinux once a day were less likely to develop PE. 3 Occasionally, when anticoagulants cannot be used, the health care provider will monitor the SVT with repeated ultrasounds over a few weeks to be sure the clot is not growing. In very rare cases, the clot may be removed surgically if the symptoms are not controlled.
What are the long-term effects of SVT?
Patients with SVT typically recover over several weeks with no serious consequences, although sometimes there may be dark discoloration of the skin over the vein that was affected. This discoloration usually resolves over time. Rarely, when the SVT travels into the deep system or to the lungs, the health care provider prescribes blood thinners for several months or more, depending on the patient’s underlying risk factors for getting future clots. Some patients with varicose veins and repeated episodes of SVT may develop long-term changes in the skin on the legs such as darkening, thinning, or, in the most severe cases, open sores, which can be very slow to heal. These skin changes are typically at the ankle and lower part of the leg. Patients with varicose veins are often advised to wear compression stockings, which are prescription-strength elastic socks that help control swelling and prevent these skin changes from occurring.
How is SVT prevented?
Patients who are hospitalized or undergo surgery often are at higher risk for blood clots, so while hospitalized and occasionally at home they are given a short course of anticoagulants, which helps to prevent SVT as well as DVT. Patients with varicose veins should avoid injury to the legs, which can provoke SVT. In patients with varicose veins, daily use of compression stockings may be helpful in preventing SVT. For patients with a tendency to form blood clots and who have had a clot in the deep system, anticoagulation helps prevent SVT in addition to DVT.
Summary
Superficial vein thrombosis is a clot in a superficial vein, which can lead to pain, redness, and swelling in the affected body part. Superficial vein thrombosis may be diagnosed on physical examination, but more often is diagnosed using ultrasound. Treatment is often aimed at improving symptoms, though some patients may be prescribed anticoagulant medications for weeks to months. Long-term complications are uncommon.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.