
Abstract
Evaluation for underlying hypercoagulable states in patients with thrombosis is a frequent clinical conundrum. Testing for thrombophilias is often reflexively performed without strategic approach nor clear appreciation of the clinical implications of such results. Guidelines vary in the appropriate utilization of thrombophilia testing. In this review, we discuss the more commonly encountered inherited and acquired thrombophilias, their association with initial and recurrent venous thromboembolism, arterial thromboembolism, and role in women’s health. We suggest an approach to thrombophilia testing guided by the clinical presentation, suspected pathophysiology, and an understanding of how such results may affect patient care.
The University of Virginia School of Medicine designates this journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit™ per article. Participants should claim only the credit commensurate with the extent of their participation in the activity. Learners are expected to read this article, along with any references and supporting material as appropriate, and complete the online post-test questions with an 80% pass rate to receive credit. CME credit may be claimed immediately after completing the quiz. This activity expires 2 years after the publication date, on
The faculty, staff and planning committee of the University of Virginia Office of Continuing Medical Education have no financial affiliations to disclose.
The CME planning committee disclosed the following: Heather Gornik has disclosed research support from AstraZeneca and CVR Global, intellectual property rights from Summit Doppler Systems, Inc., and intellectual property rights and stock/ownership from FlexLife Health (proceeds donated). Aditya Sharma has disclosed research support from National Institute of Health Sciences, AstraZeneca, Biomet Biologics, and Portola Pharmaceuticals. Valerie Clark has no financial affiliations to disclose.
The authors disclosed the following: Gregory Piazza receives research grant support from EKOS, a BTG International Group company, Bristol-Myers Squibb, Daiichi-Sankyo, and Janssen, and consulting fees from Portola and Bayer. Brett Carroll has disclosed no financial relationship or interest with any proprietary entity producing healthcare goods or services.
Cases
Introduction
The evaluation of an underlying tendency for venous and arterial thromboembolism (called thrombophilia or hypercoagulable testing) is a frequently encountered clinical challenge faced by primary care physicians, hospitalists, and thrombosis specialists alike. Though testing for inherited and acquired thrombophilia is often reflexively performed, the correct timing, appropriate utilization, and implications of such testing is poorly understood. The data are inconsistent and limited regarding the appropriate use of thrombophilia evaluation. Accordingly, guidelines vary and offer limited recommendations.1 –3
Thrombophilias represent inherited and acquired hypercoagulable states that increase the risk of venous and, in some cases, arterial thromboembolism. The incidence of thrombophilias varies based on the specific population evaluated. In the general population, thrombophilias are relatively rare in comparison to more traditional risk factors for venous VTE including cancer, immobility, post-surgery, and obesity. The prevalence increases when evaluating patients with an initial VTE or in those with a family history of VTE. In the RIETE registry of 21,367 patients, 21% were tested for inherited thrombophilia, of which 32% (7% of the total cohort) were positive. 4 The rate of thrombophilia was similar between those with an unprovoked and provoked VTE. Factor V Leiden was the most common thrombophilia (26%) followed by antiphospholipid antibodies (20%) and prothrombin gene mutation (18%). In a United States registry of patients with DVT, 5% were found to have a thrombophilia. 5
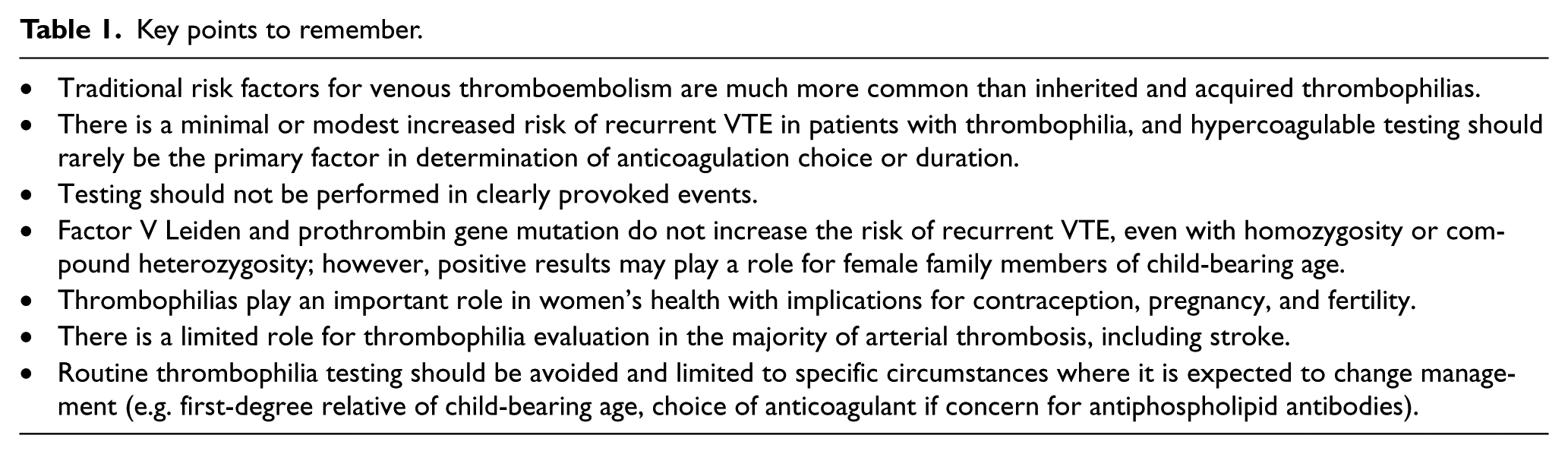
Thrombophilias can be categorized according to prevalence, associated risk with venous and/or arterial thrombosis, implications for women’s health, and contribution to recurrent thrombotic events. This review will discuss the major thrombophilias, role for appropriate testing, utility of testing in arterial thrombosis, in women’s health, and for risk assessment of recurrent VTE (Table 1).
Key points to remember.
Major thrombophilias
Factor V Leiden
Factor V Leiden is a result of a guanine-to-adenine substitution at nucleotide 1691 with translation of a glutamine rather than an arginine at amino acid residue 506. This mutation in factor V results in resistance to cleavage by activated protein C and a relative increase in thrombin production. The prevalence of heterozygosity for factor V Leiden varies by ethnicity, with the highest rate in Caucasian patients (5%) and lower in Hispanic (2%), African American (1.2%), and Asian (0.4%) patients. 6 Testing for factor V Leiden usually occurs in a two-step process: initially with a screening assay for activated protein C resistance, followed by direct DNA-based genotyping in those with a positive screen. Direct DNA testing can be considered as the first and only test in those patients with a family member known to have the gene.
Heterozygotes have a three- to fourfold increased risk of first VTE event (Table 2). Though rare, the risk is further elevated to 11-fold in homozygotes.7,8 Though frequently considered in young patients with VTE, studies from two decades ago showed that the incidence of VTE was similar in men <50 years old with or without factor V Leiden; however, VTE was sixfold higher in those ≥70 years old with factor V Leiden compared to those without the mutation, demonstrating factor V Leiden remains associated with thrombosis into elderly age. 9 Although it increases the risk of an initial VTE, factor V Leiden has not been associated with recurrence across a number of studies.10,11 Factor V Leiden has also not been consistently associated with arterial thromboembolism.12,13
Risk of initial and recurrent VTE.
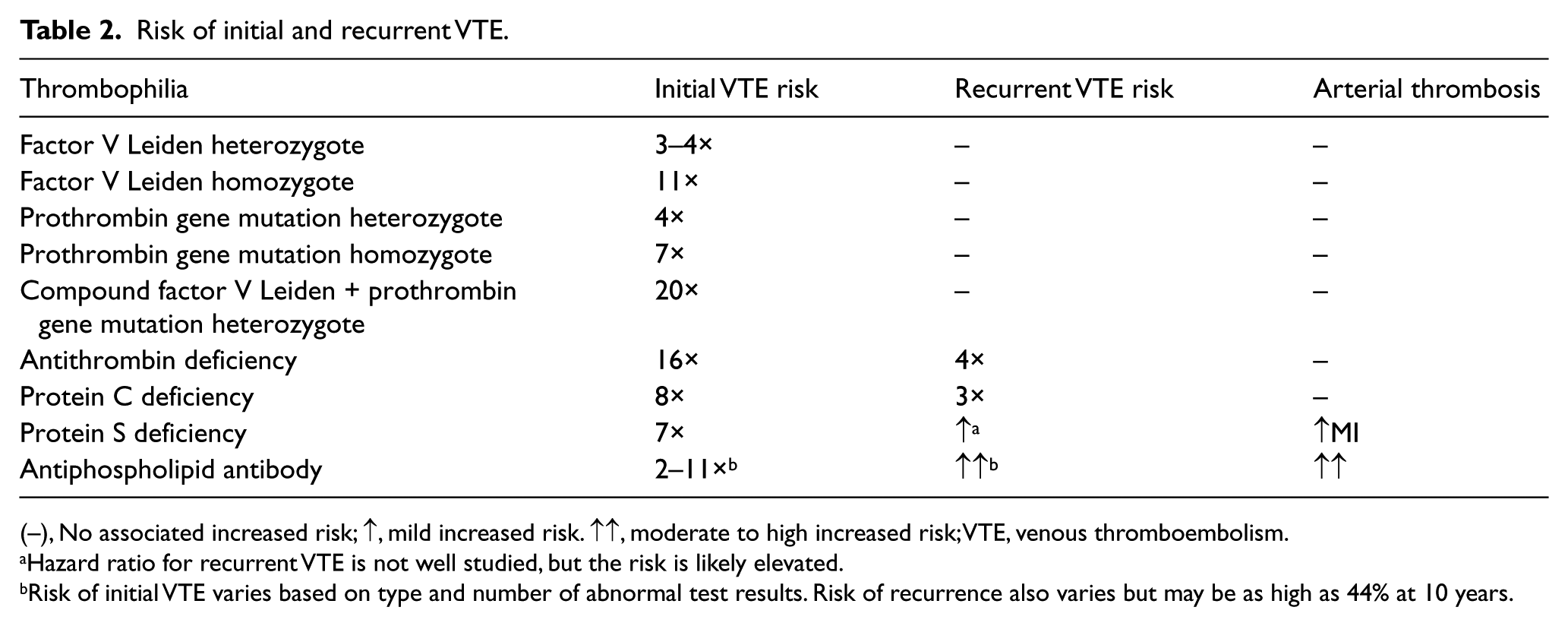
(–), No associated increased risk; ↑, mild increased risk. ↑↑, moderate to high increased risk; VTE, venous thromboembolism.
Hazard ratio for recurrent VTE is not well studied, but the risk is likely elevated.
Risk of initial VTE varies based on type and number of abnormal test results. Risk of recurrence also varies but may be as high as 44% at 10 years.
Prothrombin gene mutation
The most frequent genetic defect involving the prothrombin gene is substitution of a guanine to adenine at nucleotide 20210 in the 3’ untranslated region. The polymorphism causes up to a 30% increase in plasma prothrombin levels in heterozygotes compared with non-carriers. Prothrombin gene mutation is most commonly found in the Caucasian population and is rare in African or Asian descent. 14 Prevalence in Caucasian populations ranges from 1% to 6%, with an overall prevalence of approximately 2%. 14 Testing for prothrombin gene mutation is performed by direct DNA-based genotyping.
Heterozygotes have an associated fourfold increased risk of VTE.7,8 Homozygotes are rare, but have an estimated sevenfold increased risk. 7 Some patients may have compound heterozygosity for both factor V Leiden and prothrombin gene mutation. The reported elevated risk of first VTE event varies, but may be increased as high as 20-fold.7,8 Similar to factor V Leiden, prothrombin gene mutation does not appear to be associated with an increased risk of VTE recurrence.11,15 Prothrombin gene mutation has not been consistently demonstrated to increase the risk of arterial thromboembolism. 12
Antithrombin deficiency
Antithrombin is a serine protease inhibitor that acts as a natural anticoagulant via inhibition of thrombin, factor Xa, and other serine proteases in the coagulation cascade. Deficiency of antithrombin is inherited in an autosomal dominant fashion with variable penetrance. Type I deficiency is a decreased amount of antithrombin most often caused by a genetic defect that results in the reduction in synthesis of the protein and less frequently the stability of the protein. Type II defects result in functionally defective antithrombin. Antithrombin levels can be decreased in various clinical conditions and should not be checked in such circumstances to avoid false positive testing (Table 3).16,17 The increased thrombotic risk associated with antithrombin deficiency occurs when levels are reduced by approximately 50% from normal range. 18 Antithrombin deficiency should be suspected in patients that have difficulty achieving therapeutic partial thromboplastin time while receiving heparin. Heparin is an indirect inhibitor of thrombin and factor Xa and requires antithrombin to be effective; thus, acquired or hereditary antithrombin deficiency can limit the ability to achieve adequate anticoagulation with heparin.
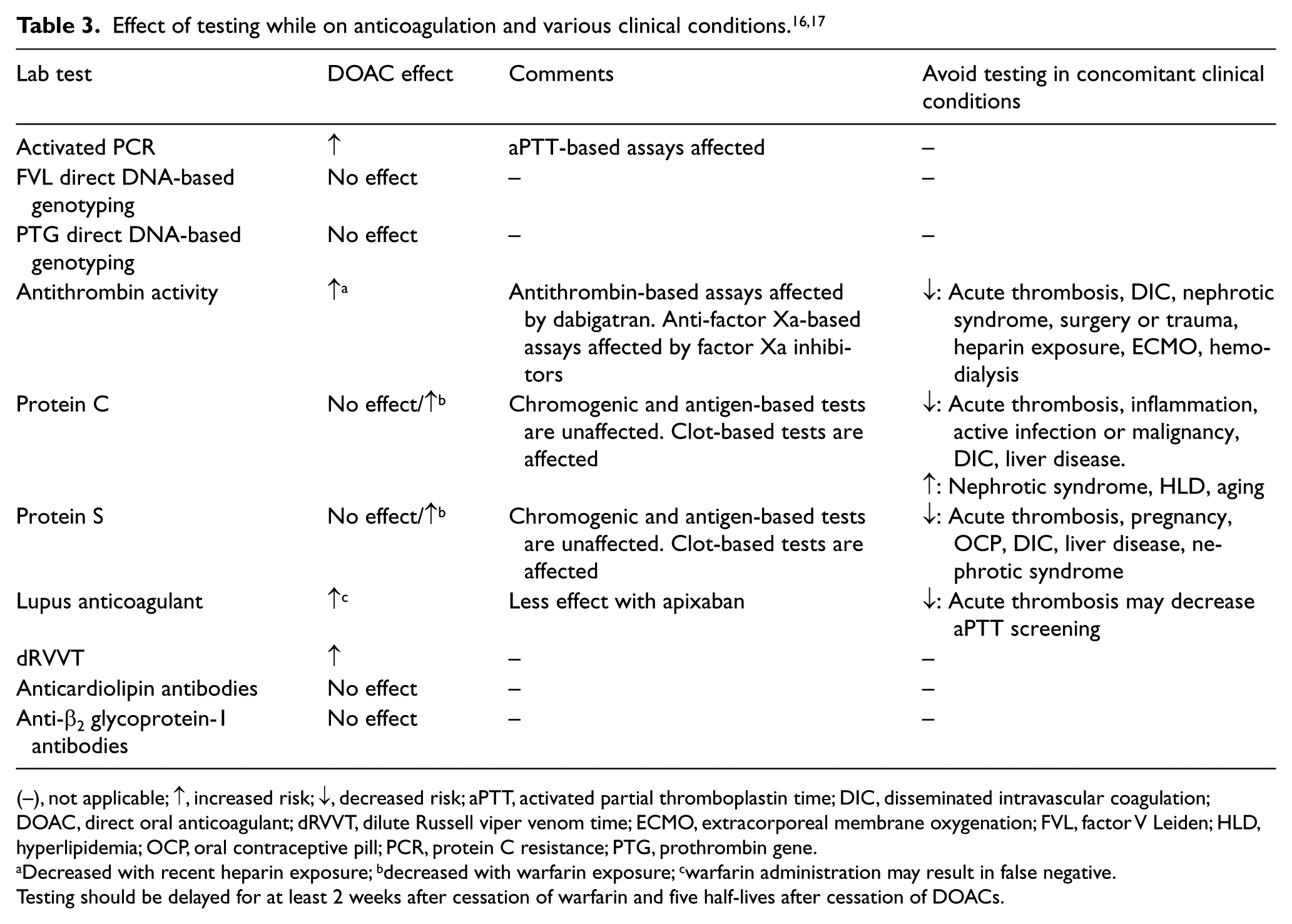
(–), not applicable; ↑, increased risk; ↓, decreased risk; aPTT, activated partial thromboplastin time; DIC, disseminated intravascular coagulation; DOAC, direct oral anticoagulant; dRVVT, dilute Russell viper venom time; ECMO, extracorporeal membrane oxygenation; FVL, factor V Leiden; HLD, hyperlipidemia; OCP, oral contraceptive pill; PCR, protein C resistance; PTG, prothrombin gene.
Decreased with recent heparin exposure; bdecreased with warfarin exposure; cwarfarin administration may result in false negative.
Testing should be delayed for at least 2 weeks after cessation of warfarin and five half-lives after cessation of DOACs.
Antithrombin deficiency occurs in 1/5000 to 1/500 individuals and is present in 0.5% of patients with a VTE. 19 In a recent meta-analysis of observational studies, the risk of first VTE was increased 16-fold in those with antithrombin deficiency. 20 However, the risk of recurrent VTE was elevated only fourfold. 20 There is no association of antithrombin deficiency with arterial thrombosis.
Protein C and protein S deficiencies
Protein C is a vitamin K-dependent anticoagulant that circulates as a zymogen, and once in its activated form it inactivates factors Va and VIIIa. Protein S functions as a cofactor for activated protein C. Both protein C and protein S are associated with genetic polymorphisms that result in either a decreased amount of protein or abnormal function. Both deficiencies are inherited in an autosomal dominant fashion. Both are rare in the general population. In patients with VTE, protein C and S occur with similar frequency, ranging from 3% to 7%.19,21 The preferred method for testing protein C is a functional assay to evaluate both levels and function. Assessing protein S is best performed by checking the free protein S level.
Protein C is associated with an eightfold increased risk of VTE and protein S is associated with a five- to sevenfold increased risk of VTE. 22 Risk of VTE recurrence was found to be at least threefold higher in patients with protein C deficiency. Reported rates of recurrent VTE in patients with protein S deficiency range from 7% to 16% per year.23,24 Protein S deficiency has been associated with coronary artery disease in otherwise healthy middle aged men. 25 No association between stroke in protein C or protein S deficiencies has been demonstrated.
Antiphospholipid antibody syndrome
Antiphospholipid antibody syndrome is an acquired thrombophilia that involves the development of one or more autoantibodies against antigens on cell membrane phospholipids, the associated plasma proteins, or plasma coagulation molecules. These antibodies increase the risk of both arterial and venous thrombosis through multiple mechanisms that may result in endothelial injury and activation of coagulation. 26 Though VTE and stroke are the most common clinical presentations of antiphospholipid antibodies, any arterial or venous circulation can be affected. Positive anticardiolipin antibodies after VTE has been associated with an increased VTE recurrence, along with increased risk of death at 4-year follow up compared to patients with VTE and negative antibodies. 27 Antiphospholipid antibodies also play an important role in maternal complications, as will be discussed below. A rare presentation of antiphospholipid antibody syndrome is the development of acute thromboses in multiple vascular beds with resultant multisystem organ failure, referred to as catastrophic antiphospholipid antibody syndrome.
Diagnosis of antiphospholipid syndrome requires both clinical and laboratory abnormalities in accordance with the Sappora criteria (Table 4). 28 Antiphospholipid antibodies are assessed individually, with tests for lupus anticoagulant, anticardiolipin antibodies, anti-β2 glycoprotein-1 antibodies, and antiprothrombin antibodies being some of the more frequently utilized. The initial screening test for lupus anticoagulant is most commonly with activated partial thromboplastin time (aPTT). If aPTT is prolonged, the patient’s plasma is mixed with normal plasma, and if it remains prolonged a confirmatory test is performed with the hexagonal phase phospholipid (HPPL) test. HPPL is a soybean extract of phospholipid that will bind to lupus anticoagulant, thus the aPTT will shorten if HPPL is added in the presence of lupus anticoagulant. An additional screening test for lupus anticoagulant includes dRVVT, which will be prolonged in the presence of lupus anticoagulant.
Diagnostic criteria for antiphospholipid antibody syndrome. 28
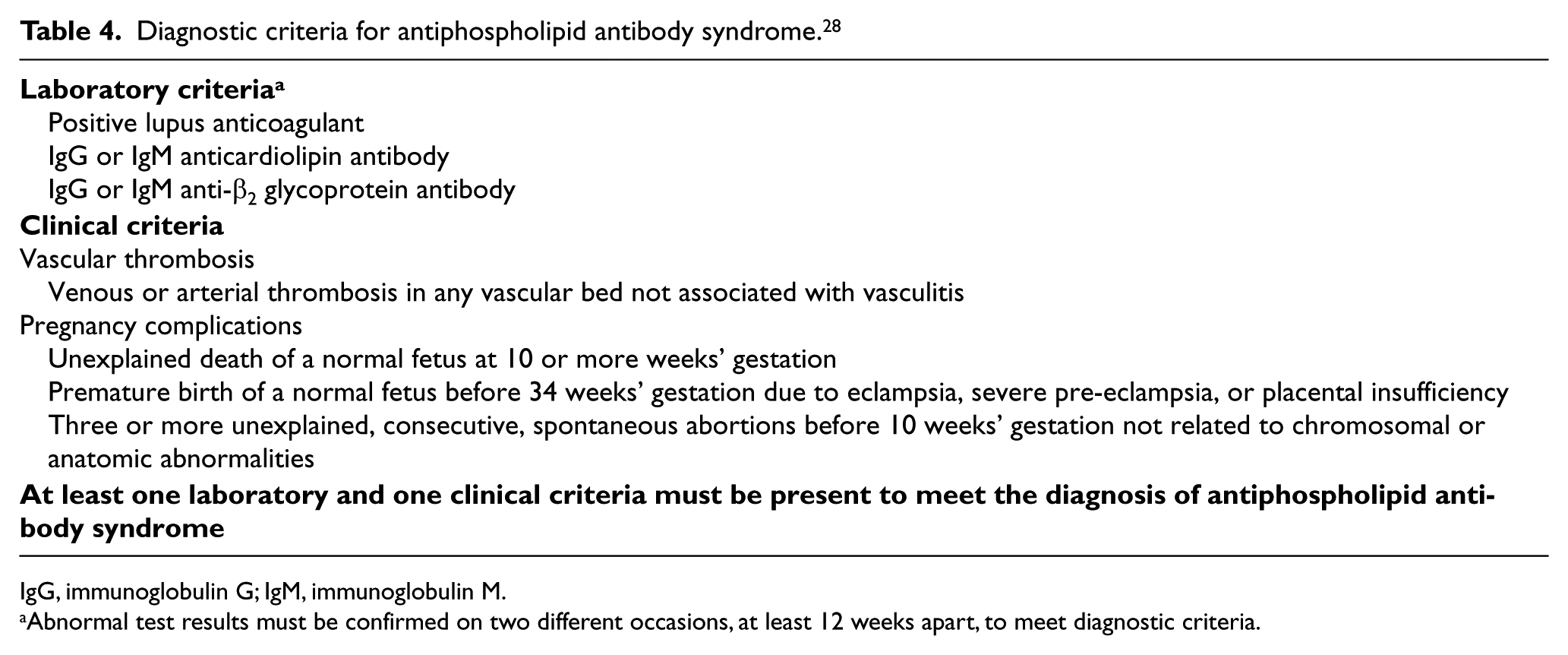
IgG, immunoglobulin G; IgM, immunoglobulin M.
Abnormal test results must be confirmed on two different occasions, at least 12 weeks apart, to meet diagnostic criteria.
Unlike many of the thrombophilias discussed above, antiphospholipid antibodies are clearly associated with arterial thrombosis. Antiphospholipid antibodies are estimated to be present in 9% of women with pregnancy loss, 14% with stroke, 11% with myocardial infarction (MI), and 10% with DVT. 29 Risk of thrombosis appears to vary with the type and number of antiphospholipid antibodies present. Lupus anticoagulant is associated with an 11-fold increased risk of thrombosis, with a milder increased risk of 1.6-fold in those with anticardiolipin antibodies. 30 Risk appears to be higher when triple positivity is present. 31 Risk of recurrent thrombosis is high with estimates of 12% at 1-year follow up, 17–26% at 5 years, and 30–44% at 10 years.31,32
Hyperhomocysteinemia
Risk of VTE increases up to fourfold if homocysteine levels are >22 µmol/L; levels less than this are associated with minimal risk. 33 Markedly elevated levels of homocysteine are also associated with arterial thromboembolism. Though the risk of thrombosis may be elevated in patients with methylenetetrahydrofolate reductase (MTHFR) polymorphisms, which result in elevated homocysteine levels, there is a high prevalence in the general population and it has not been shown to increase the risk of first or recurrent VTE. 7 Most thrombosis specialists do not regularly check homocysteine levels in patients with thrombosis as no therapy targeted to lower homocysteine has been shown to change thromboembolic risk.
Lipoprotein(a)
Lipoprotein(a) is a type of low-density lipoprotein. Levels can vary and are primarily determined by various polymorphisms. Elevated lipoprotein(a) is believed to have a causal relationship with MIs and is a risk factor for stroke. Increased lipoprotein(a) levels, particularly in low molecular weight phenotypes, have also been implicated in thrombosis via numerous mechanisms, including inhibition of the fibrinolytic pathway via attenuation of plasminogen binding to fibrin and enhancement of the tissue factor-mediated pathway. 34 Though there is a clear association with lipoprotein(a) and cardiovascular disease, there are contradicting data regarding an association with VTE in adults; however, one meta-analysis did demonstrate an almost twofold increased risk with levels >300 mg/L.35,36 Another meta-analysis showed a fivefold increased risk for initial VTE in children, with no significant increased risk in rate of recurrent VTE. 37 Lipoprotein(a) is rarely checked in VTE, but can be considered in a patient with premature coronary artery disease without other risk factors.
Thrombophilia and women’s health
There are unique considerations in women’s health that warrant specific note when considering thrombophilia evaluation, including contraception selection, pregnancy associated VTE, and infertility.
Contraception and thrombophilia
Combination oral contraceptive pills (OCPs), particularly those with third generation progestins, are associated with at least a three- to fourfold increased risk of VTE and a doubling of the risk of recurrence if continued after an initial event.15,38 Estrogen-based OCPs compound the baseline risk of VTE in patients with a thrombophilia and are associated with a 20- to 40-fold increased risk of an initial VTE event. The risk appears to be highest within the first 6 months after OCP initiation. 39 When compared with women without factor V Leiden and no OCP use, VTE risk was fourfold higher in those with OCP use and a non-carrier of factor V Leiden, sevenfold higher in heterozygotes for factor V Leiden and no OCP use, and 35-fold higher with OCP use in heterozygotes for factor V Leiden. 39 A recent meta-analysis suggests only a slightly greater risk of VTE in those with high-risk thrombophilia and OCP use (sevenfold) compared with those with low-risk thrombophilia and OCP use (sixfold). 40 In a study evaluating women who had VTE while taking an OCP, the presence of a family history of VTE was not associated with risk of VTE with OCP use; however, the presence of thrombophilia did (odds ratio (OR) 2.13, 95% confidence interval (CI) 1.32–3.51; p = 0.003). 41 Interestingly, in the same study, smoking similarly increased risk of VTE as the presence of thrombophilia (OR 1.65, 95% CI 1.30–2.10; p<0.0001) and a body mass index ≥35 kg/m2 was associated with an even higher risk than thrombophilia (OR 3.46, 95% CI 1.81–7.03; p = 0.0003).
Second generation OCPs with low-dose estrogen and progestins, such as levonorgestrel, are the safest combination formulations. Reduction of the estrogen component from 50 μg to 30–40 μg reduces the risk of VTE, with lower doses (20–30 μg) associated with the lowest risk. The progestin only pill, the Mirena® intrauterine device (IUD) (which releases approximately 20 μg of levonorgestrel), and copper intrauterine devices are not associated with VTE. We advise against the use of depot medroxyprogesterone acetate injections as some association of increased risk has been demonstrated. 42 We do not recommend the regular screening of inherited thrombophilias prior to initiation of OCPs; however, testing can be considered in those patients with a known family history of thrombophilia as it may alter the contraceptive choice in discussion with the patient.
Infertility and pregnancy risks
Thrombophilias have been associated with increased risk of both early and late miscarriages. Increased risk of miscarriage for the majority of thrombophilias ranges from two- to fourfold, but may be as high as 20-fold for late miscarriages in women with protein S deficiency. 43 Thrombophilia is also associated with increased risk of severe pre-eclampsia, abruptio placentae, and fetal growth retardation. 44 Both heterozygosity for factor V Leiden or prothrombin gene mutation are associated with an approximate doubling of the risk of recurrent pregnancy loss. 45 The rate of thrombophilia among women with infertility has been estimated to be quite high. In one small study of 45 women undergoing in vitro fertilization, all underwent thrombophilia testing: 32 (71%) were found to have a thrombophilia. 46
Common scenarios for thrombophilia testing in the women’s health setting include: history of prior thrombosis, unexplained fetal death at >10 weeks’ gestation, history of premature delivery at <34 weeks’ gestation, history of eclampsia or severe pre-eclampsia, and history of two or more unexplained miscarriages. Although some guidelines suggest reserving testing to patients with three or more miscarriages, we emphasize minimizing the repetitive emotional and psychological trauma of miscarriage before thrombophilia testing. Guidelines also suggest only testing for thrombophilia in women with first trimester pregnancy loss. Observational studies show that miscarriage can occur at any point in pregnancy, early or late, in patients with thrombophilia.
Thrombophilia, pregnancy, and VTE
During pregnancy, there are multiple physiologic changes that establish a hypercoagulable state, including increased resistance to activated protein C, fibrinogen, and factors II, VII, VIII, IX, and X, and decreased protein S. Non-coagulation-related changes that further increase risk of VTE include greater venous capacitance, uterine compression of pelvic veins, and a tendency for decreased mobility, especially in the late stages of pregnancy. Pregnancy is additive in the baseline risk of VTE in patients with thrombophilia. Compared to pregnant women without a thrombophilia, there is a ninefold increased risk of an initial VTE in heterozygote carriers of factor V Leiden, a sevenfold increased risk in heterozygote carriers of prothrombin gene mutation, and a 34-fold increased risk in pregnant homozygote carriers of factor V Leiden. A recent study found those with homozygosity for factor V Leiden or prothrombin gene mutation or compound heterozygosity experienced a nearly 8% risk of VTE during pregnancy regardless of family history of VTE. 47 A meta-analysis of observational studies demonstrated the absolute risk of VTE with high-risk thrombophilias ranged from 1% to 7% in the antepartum period and 3–11% in the postpartum period. Low-risk thrombophilias were associated with a total risk of <3% during the peripartum period. 48 Despite these associated increased risks, given the overall low prevalence of thrombophilias and number of women who become pregnant, thrombophilia testing is not routinely performed in pregnant women. Testing can be considered in those with a suggested personal or family history of thrombosis.
Thrombophilia and stroke
Thrombophilia testing is frequently performed in patients with an ischemic stroke, particularly those of an unclear etiology and in younger patients (<50 years old).49,50 The benefit of such testing has not been well supported in the literature. A case–control study of 219 patients with a first ischemic stroke found a prevalence of thrombophilia to be 14.7% in those with a stroke and 11.7% in the control group. 51 The presence of thrombophilia was thought to be more likely coincidental rather than causative in the majority of cases. A systemic review evaluated the prevalence of specific thrombophilias after an ischemic stroke and found a lupus anticoagulant in 3%, anticardiolipin antibodies in 17%, factor V Leiden in 7%, and prothrombin gene mutation in 5%, with a slightly higher rate in those ≤50 years of age. Protein C, protein S, and antithrombin deficiencies were rare. 50
The Antiphospholipid Antibodies and Stroke Study was a prospective cohort study within the Warfarin–Aspirin Recurrent Stroke Study (WARSS). Of the 1770 patients included, all of whom had an ischemic stroke, 720 (41%) were classified as antiphospholipid antibody positive. However, there were equal rates of thrombo-occlusive events in those with or without antiphospholipid antibodies. Further, in those patients with antiphospholipid antibodies, there was no decrease in risk of events in those receiving warfarin versus aspirin. There was a suggestion of a higher event rate in those who tested positive for both lupus anticoagulant and anticardiolipin antibodies compared with those who were negative for both (unadjusted relative risk (RR) 1.36, 95% CI 0.97–1.93; p = 0.07). 52 Other data demonstrated an increased risk of recurrent stroke in those with persistently elevated antiphospholipid antibodies in patients 18–45 years old (hazard ratio (HR) 2.74, 95% CI 1.75–4.30; p < 0.001). 53 There was no increased risk in patients with factor V Leiden or prothrombin gene mutation.
Limited thrombophilia testing with antiphospholipid antibodies can be considered in young patients with no other clear source of stroke, particularly those with systemic lupus erythematosus; however, it remains unclear how such results should inform management of these patients based on the data above. Thrombophilia testing in patients with recurrent cryptogenic stroke or prior thrombosis may also be reasonable if there is consideration for long-term anticoagulation, though the data to support such a practice are limited. There are no definitive data supporting testing for factor V Leiden, prothrombin gene mutation, protein C, protein S, and antithrombin deficiencies.
There are conflicting data regarding the association and causal relationship of hyperhomocysteinemia and stroke. In the Vitamin Intervention for Stroke Prevention trial, there was no difference in rates of stroke, MI or death in those who received high versus low-dose vitamin B supplementation for reduction of homocysteine levels. 54 The combined endpoint was also negative in the HOPE-2 trial in which patients received folic acid or vitamin B supplementation, though there was a slightly decreased risk of stroke (RR 0.75, 95% CI 0.59–0.97; p = 0.03). 55 Testing for hyperhomocysteinemia in the setting of an ischemic stroke is of low yield given the rare prevalence of very elevated levels; though it can be considered in those with recurrent cryptogenic stroke. In a review of 19,678 patients with thrombosis who underwent thrombophilia testing, two per 1000 had severely elevated levels (>100 µmol/L) and only two out of 10,000 had a stroke as their first thrombotic event. As noted above, targeted intervention to lower homocysteine levels does not appear to impact thrombotic risk. 56
Testing strategies
When considering thrombophilia testing, a patient-centered approach is paramount together with an understanding of what the clinical implications of such results are and if/how the results would ultimately change management. Testing is often contemplated when determining the duration of anticoagulation after a thrombotic event, to aid in the prediction of recurrence, to establish the optimal intensity of thromboprophylaxis, to assess the risk during pregnancy or hormonal contraceptive use, or to identify family members at elevated risk.
We consider thrombophilia testing in select patients with specific clinical characteristics that are suggestive of a potential thrombophilia, such as patients with thrombosis at a young age, particularly those with weak provoking factors or an unprovoked event, a family history of VTE (specifically a first-degree relative with an event at a young age), recurrent VTE, and VTE in unusual sites like the splanchnic or cerebral veins, and recurrent pregnancy loss (Figures 1 and 2). VTE is more common with aging due to increased concomitant non-inherited hypercoagulable states. Rates of VTE increase significantly in those >60 years old; 49 thus, those patients who are younger are more likely to have a thrombophilia as the cause of their VTE.
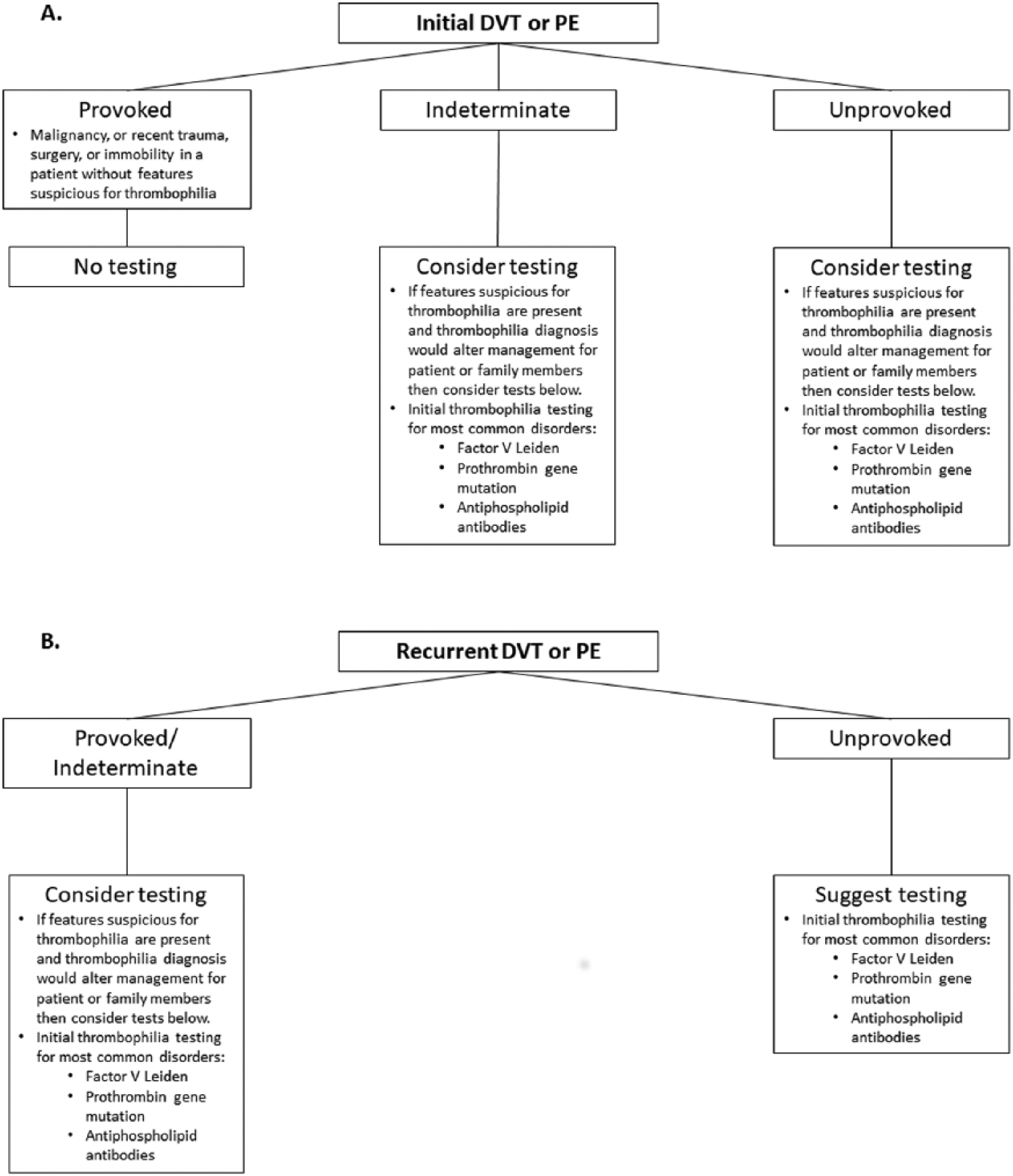
Approach to thrombophilia testing in deep vein thrombosis (DVT) and pulmonary embolism (PE). (A) The provocation of an initial deep vein thrombosis or pulmonary embolism should be the main factor in determining the role of testing. (B) Testing should be considered in all patients with a recurrent venous thromboembolism.
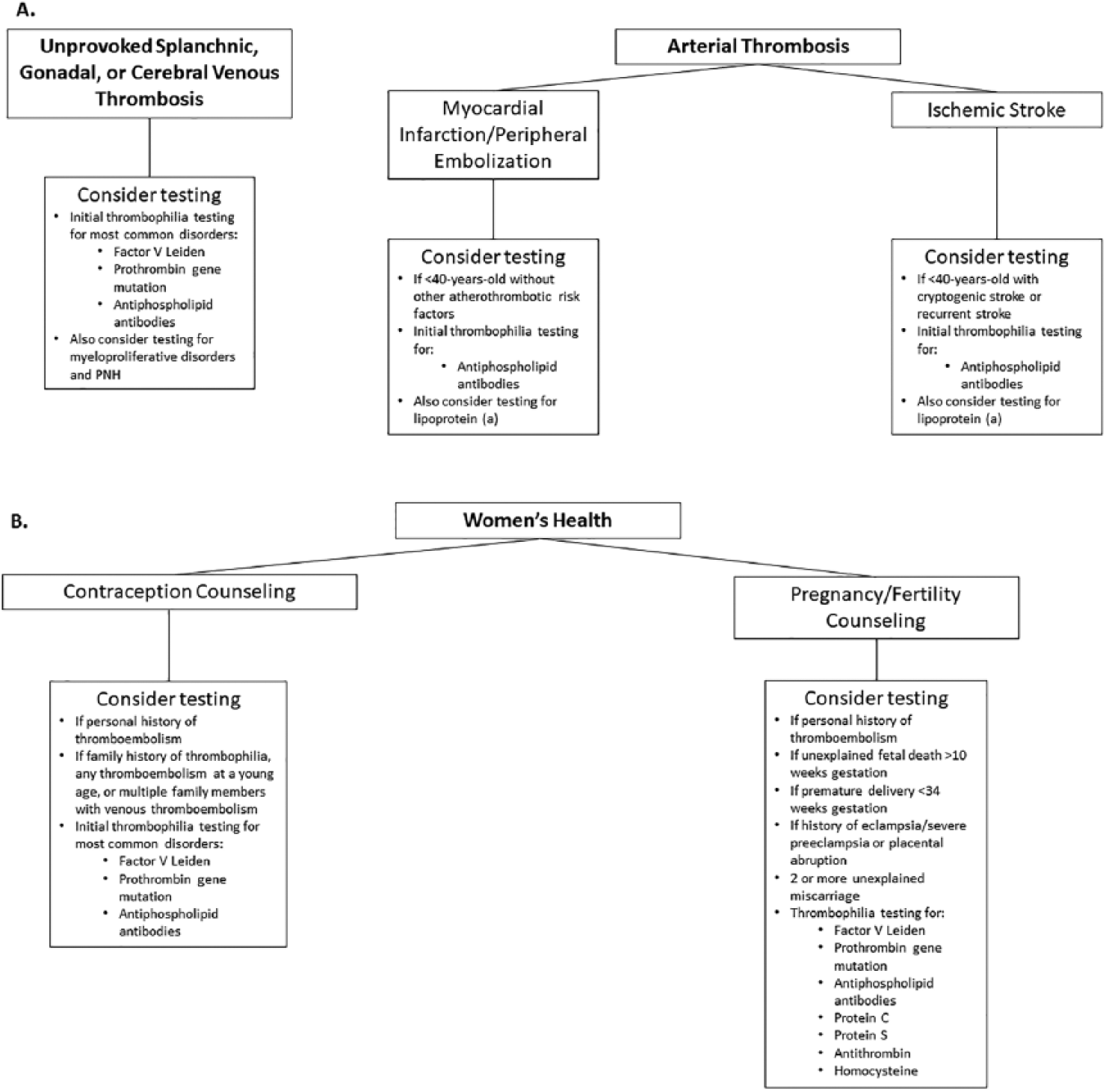
Approach to thrombophilia testing in unusual venous thrombosis, arterial thrombosis, and women’s health. (A) Testing should be considered in patients with unprovoked splanchnic, gonadal, or cerebral venous thrombosis, including evaluation of myeloproliferative disorders with JAK2 gene mutation analysis. Testing in patients with arterial thrombosis should be limited to young patients without other risk factors for their presentations. (B) There are various clinical circumstances where testing can be considered in women’s health. (DVT, deep vein thrombosis; PNH, paroxysmal nocturnal hemoglobinuria; PE, pulmonary embolism.)
There is an increased association of thrombophilias with splanchnic and cerebral venous thromboses. 57 Though testing is commonly performed, such events are more often associated with other contributing factors such as cirrhosis, anatomic abnormalities (e.g. local compression by a mass), or elevated estrogen states. The role of such testing and the implications of thrombophilia results is not well defined and mostly based on expert consensus. Patients with unprovoked splanchnic vein thrombosis should also be assessed for myeloproliferative neoplasms and paroxysmal nocturnal hemoglobinuria. 58
Testing can be considered in those with a strong family history of VTE, particularly in those with a first-degree relative with an unprovoked VTE at an age <50 years with a known thrombophilia status. Issues can arise when testing patients with a family history but an unknown thrombophilia status in the effected family member. Negative test results can lead to inappropriate reassurance and under treatment or prophylaxis. First-degree relatives of patients that have had a prior VTE are at elevated risk even if thrombophilia testing is negative in the index patient. 59
A meta-analysis and cost-effectiveness analysis that evaluated thrombophilia screening in select patient populations in the United Kingdom demonstrated screening in patients prior to hormone replacement therapy was most cost-effective. 60 Screening prior to initiation of combination OCP was least cost-effective. Testing prior to major orthopedic surgery was intermediate in terms of cost-effectiveness. Overall, screening was more cost-effective when performed in patients with a previous personal and/or family history of VTE. A Markov model evaluated testing or no testing followed by 6–36 months of anticoagulation in a cohort of patients with unprovoked DVT. Thrombophilia testing followed by 24 months of anticoagulation in those with a positive test was more cost-effective than no testing with 6 months of anticoagulation. Lifetime anticoagulation was preferred based on cost for patients with antiphospholipid antibody syndrome and homozygous carriers of factor V Leiden. 61
Testing should not be performed when there is a clear provoking event in the absence of other factors suspicious for thrombophilia or in those with concomitant malignancy, as such results should not alter the treatment plan.1,58 If testing is pursued, it can be performed all at once or in a stepwise fashion. We recommend focused testing for those particular thrombophilias that are most likely to affect clinical decision-making or are most prevalent, rather than sending all-inclusive ‘thrombophilia panels’. Factor V Leiden, prothrombin gene mutation, and antiphospholipid antibodies are more prevalent than the other thrombophilias. Protein C, protein S, antithrombin deficiencies, and homocysteine levels tend to be of low yield and should generally be limited to individuals with particularly high-risk and unique presentations. Testing for factor VII activity, elevated IX, and XI activity, levels of fibrinogen and plasminogen activator inhibitor-1, and MTHFR gene mutation are not definitively associated with risk or require further validation prior to implementation in thrombophilia testing. 58
When deemed appropriate, factor V Leiden, prothrombin gene mutation, and antiphospholipid antibodies (excluding lupus anticoagulant) can be tested in the acute phase of thrombosis in the initial evaluation, as they are neither affected by acute thrombosis or anticoagulants, though such results rarely alter the initial anticoagulation plan. Protein C, protein S, and antithrombin deficiencies can be considered in secondary evaluation in select patients after the completion of anticoagulation. Other than the rare circumstance where testing is felt to be of particular importance in the initial evaluation or treatment plan, we recommend deferring testing to an outpatient follow up appointment. Such a strategy allows for more time for discussion with the patient of the implications of such testing and the management options, compared to the often hectic and overwhelming acute hospital setting.
Thrombophilia and recurrent VTE
Much of the debate regarding utility of thrombophilia testing after an initial VTE is the implication of such results on treatment decisions. Though associated with initial VTE events, inherited thrombophilias have either a modest or no association with risk of recurrence. Thus, such testing should play a limited role in decisions regarding choice or duration of anticoagulation. A prior study evaluated the role of thrombophilia testing after an initial VTE and demonstrated no difference in recurrence whether testing had been performed or not. 62 There are multiple prediction models available to aid in assessing risk of VTE recurrence. Notably, most models do not include thrombophilia status in the risk calculation for recurrence.63,64
Antiphospholipid antibodies, protein C, protein S, and antithrombin deficiency likely increase the risk of recurrence. Factor V Leiden and prothrombin gene mutation do not appear to increase the risk in heterozygotes, homozygotes, or compound heterozygotes. 11 In a study of 474 patients with a first VTE event, extensive thrombophilia testing was performed and patients were followed for 7 years. 15 The cumulative incidence of recurrent PE was 19% and was similar between those with a thrombophilia and those without a thrombophilia (HR 1.4, 95% CI 0.9–2.2). Patient factors were significantly associated with an increased recurrence rate, including male sex (HR 2.7, 95% CI 1.4–5.1) and idiopathic event (HR 1.9, 95% CI 1.2–2.9).
In an analysis of 1626 patients with initial VTE, unprovoked VTE (adjusted HR 2.30, 95% CI 1.82–2.9) and presence of thrombophilia were similarly associated with recurrence (adjusted HR 2.02, 95% CI 1.52–2.69). 65 However, recurrence rate was similar between those who underwent thrombophilia testing and those who did not (21.9% vs 21.5%). Even antiphospholipid antibodies are associated with a variable risk of recurrence when evaluated in a systematic review. 66 Location of the venous thrombosis and the number and severity of positive antiphospholipid antibodies should also be considered when assessing recurrence risk. A randomized, controlled trial to evaluate the role of thrombophilia testing at the time of initial VTE and subsequent risk of recurrent VTE was stopped early due to low enrollment and funding issues. 67
Duration and choice of anticoagulation
Standard, therapeutic intensity anticoagulation should be prescribed in the acute phase of VTE treatment according to guidelines regardless of whether a thrombophilia is suspected or detected. The more difficult management decision arises in determining the duration of anticoagulation. Thrombophilia status has been utilized to justify continuation or cessation of anticoagulation. However, as noted above, given no or minimal elevated risk of recurrence with most thrombophilias, we recommend the provoked or unprovoked nature of the initial VTE event should be primary in guiding decisions about the duration of anticoagulation. A negative thrombophilia evaluation should not be the sole justification for cessation of anticoagulation. We recommend indefinite anticoagulation in patients with an unprovoked VTE, regardless of whether a patient has heterozygosity or recurrence that may be as high as 50% at 10 years. 65 Patients with a clearly provoked VTE warrant 3–6 months of anticoagulation, regardless of whether a patient has heterozygosity or homozygosity for factor V Leiden or prothrombin gene mutation, or are compound heterozygote carriers.1,2,15 Patients with provoked or unprovoked VTE who are confirmed to have antiphospholipid antibodies with two positive tests at least 12 weeks apart should receive indefinite duration anticoagulation because of a high risk of VTE recurrence. Of note, in a study evaluating VTE recurrence while taking warfarin, 42% of the 661 patients had a thrombophilia. The rate of recurrence was similar between those with and without a thrombophilia while on warfarin. 68
Direct oral anticoagulants (DOACs) are recommended as first-line treatment for VTE by recent guidelines. 1 A small proportion of patients with inherited thrombophilia were included in the initial studies of DOACs in VTE and case series of patients with thrombophilia suggest efficacy. 69 Growing evidence suggests a role for longer-term anticoagulation with ‘half-dose’ DOACs in patients with unprovoked and even some patients with provoked events. Such a management approach may further limit the role for thrombophilia testing.70,71 A post hoc analysis and case series demonstrate the efficacy of DOACs in the setting of antiphospholipid antibodies, but given the overall small sample size to date many still prefer warfarin in patients with antiphospholipid antibodies.72,73 Focused testing may be considered in patients where there is concern for antiphospholipid antibodies, being mindful that DOACs may result in a false positive lupus anticoagulant test.
Cases
Conclusions
Evaluation of inherited and acquired thrombophilias remain a difficult area of clinical decision-making. Routine thrombophilia testing should not be performed in the majority of patients with venous and arterial thrombosis. Testing should be guided by each individual patient’s clinical circumstances and with consideration of how the potential results would change management.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Gregory Piazza receives research grant support from EKOS, a BTG International Group company, Bristol-Myers Squibb, Daiichi-Sankyo, and Janssen, and consulting fees from Portola and Bayer. Brett Carroll has disclosed no financial relationship or interest with any proprietary entity producing healthcare goods or services.
Funding
This authors disclosed no financial support for the research, authorship, and/or publication of this article.