
Abstract

There is no definitive consensus on which patients and/or family members should be tested for thrombophilia. Multiple guidelines have been published by professional medical societies about testing for thrombophilia, but recommendations vary widely.1–4 Despite dissemination of these guidelines, thrombophilia testing remains pervasive following provoked venous thromboembolism (VTE) in the acute inpatient setting. 5
As a first step, we set out to define the scope of the problem and to identify areas for improvement at our institution. We performed a retrospective chart review of consecutive unselected patients who had a Thrombosis Panel ordered from 1 July 2015 to 1 July 2016. A thrombosis panel includes testing for factor V Leiden (FVL) mutation, prothrombin G20210A gene mutation, protein C (PC) activity, free protein S (PS) antigen, antithrombin (AT) activity, prothrombin time (PT), activated partial thromboplastin time (aPTT), lupus anticoagulant (LA), dilute Russell viper venom time (DRVVT), anticardiolipin (aCL) antibody (immunoglobulin G (IgG) or IgM), anti-β2-glycoprotein (GP) I antibody (IgG or IgM) and a pathologist interpretation of the results that takes into account patients’ medications at time of testing. Individual thrombophilia tests can also be ordered separately by clinicians but are not included in this study.
We found that 155 Thrombosis Panels were ordered in 152 hospitalized adult patients during the study period: 43 (28.3%) men and 109 (71.7%) women. Mean and median age at time of testing was 48.1 and 47 years, respectively (range: 18–82 years). The following services ordered 85% of thrombosis panels: neurology (n=85, 54.8%), neurosurgery (n=21, 13.5%), emergency medicine (n=13, 8.4%) and internal medicine (n=12, 7.7%). The indications for thrombophilia testing are shown in Table 1.
Indications for thrombophilia testing.
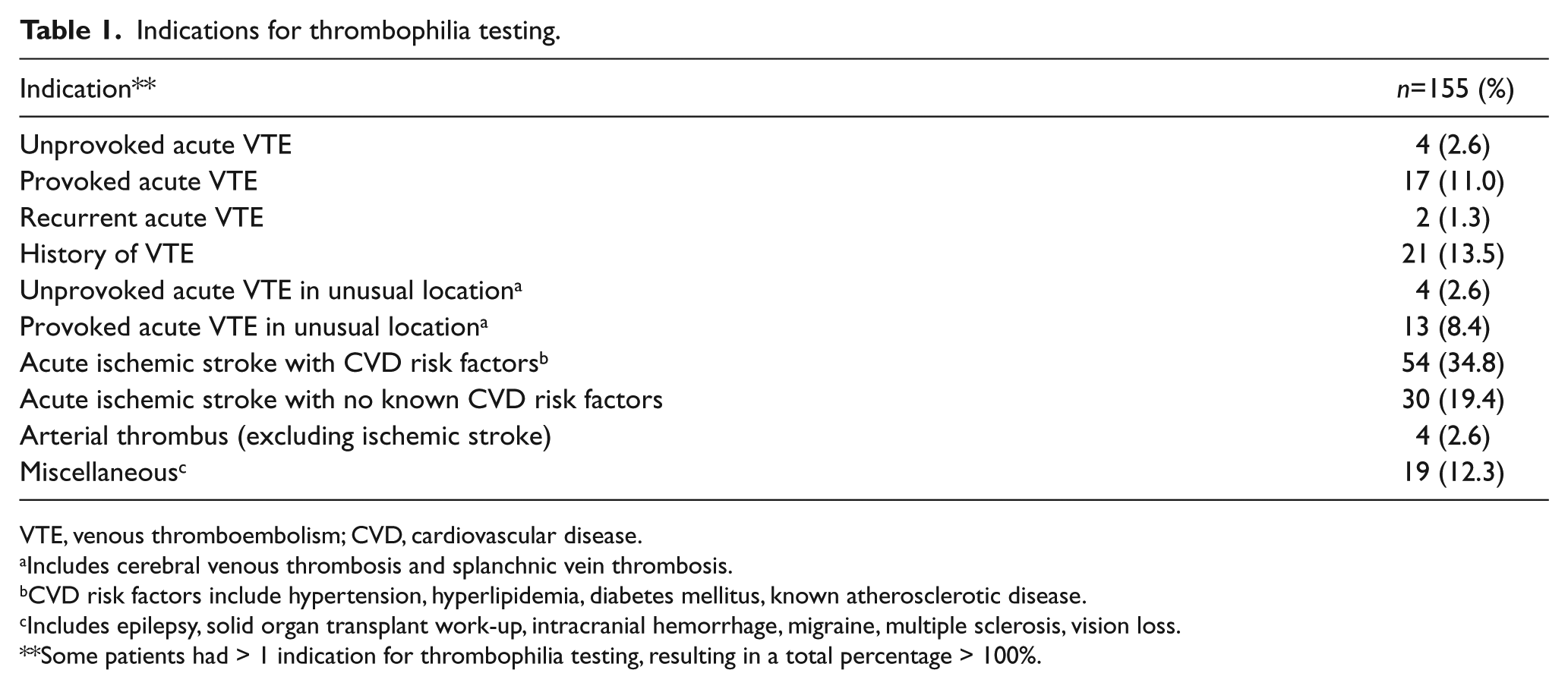
VTE, venous thromboembolism; CVD, cardiovascular disease.
Includes cerebral venous thrombosis and splanchnic vein thrombosis.
CVD risk factors include hypertension, hyperlipidemia, diabetes mellitus, known atherosclerotic disease.
Includes epilepsy, solid organ transplant work-up, intracranial hemorrhage, migraine, multiple sclerosis, vision loss.
Some patients had > 1 indication for thrombophilia testing, resulting in a total percentage > 100%.
Eighty three (54%) thrombosis panels did not reveal any thrombophilia, while 72 (46%) had one or more abnormal results. The majority of these abnormal results, specifically PC, PS and AT, were falsely abnormal as testing was performed during an acute thrombotic state and/or on concurrent anticoagulation therapy. Ten (7%) patients were found to be heterozygous for FVL mutation while six (4%) patients were heterozygous for prothrombin G20210A gene mutation. Only 10 out of 152 patients had a family history of VTE. There was no documentation of informed consent or genetic counseling occurring prior to testing in any of the cases.
Given the scope of the problem, a practical ordering plan utilizing computerized physician order entry that prevented providers from ordering a thrombosis panel in the inpatient setting was implemented. When clinicians attempt to order a thrombosis panel, an advisory note appears stating: ‘Inpatient testing is inappropriate due to suboptimal conditions, and that testing should be deferred to the outpatient setting, if clinically indicated. If inpatient testing is requested, a hematology consult is required for approval for inpatient testing to ensure appropriate indication and timing of testing.’ The hematology consult service would evaluate each patient case and selectively order individual thrombophilia tests appropriately.
In addition, the top ordering services received service-specific education on indications and appropriate timing of thrombosis panel testing. A didactic lecture on ‘Thrombophilia Testing’ was also presented to the Internal Medicine Residency Class.
Following implementation of the above recommendations, an audit of inpatient thrombophilia testing was performed over a 3-month period (June to August 2017). As the order for a thrombosis panel was no longer available, individual thrombophilia tests that included all/some of the components of the thrombosis panel was reviewed. Testing for a lupus anticoagulant panel alone, which includes PT, aPTT, LA, DRVVT, aCL IgG/IgM and GP IgG/IgM, was excluded from the audit as this test is frequently ordered by rheumatologists in patients with lupus, and not as a thrombophilia work-up. Over the 3-month period, thrombophilia testing was ordered on eight inpatients (a 79% reduction compared to pre-intervention).
Thrombophilia testing is an expensive evaluation with limited data on cost-effectiveness. 6 We identified the scope of practice and areas that could be improved by the adoption of a centralized approach to reduce inpatient thrombosis panel testing. This simple modification significantly reduced the number of thrombophilia tests in a 3-month period, leading to patient charge savings of an estimated US$332,100 per year (US$2700 per thrombosis panel test).
A major limitation to this study is that it was a retrospective chart review and was subjected to the accuracy of documentation by the clinical services. However, the authors made every effort to perform a comprehensive and detailed chart review for data collection. In addition, this is a single-center study and thus generalizability to other institutions is uncertain.
In conclusion, this study demonstrates the impact that healthcare system technology and targeted clinician education has on changing practice habits and subsequently on reducing healthcare costs. We hope that the dissemination of our study results will encourage other institutions to evaluate the practice pattern at their respective institution as an effort to improve patient care and safety, and reduce healthcare costs.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.