
Abstract
Few studies have explicitly identified factors that explain an individual’s willingness to engage in community-based exercise for claudication. Identifying the unique characteristics of those inclined toward physical activity would inform interventions that encourage walking. We examined the utility of behavioral economics-related concepts in understanding walking among Veterans with claudication. Patients who received care at the Michael E. DeBakey Veterans Affairs Medical Center in Houston, Texas, were surveyed on symptom severity, behavioral economics, stress, and depression. The primary outcome was a binary variable measuring current walking for exercise and defined as walking for at least 30 minutes every day. Multivariable logistic regression models were used to identify variables, both clinically and statistically significant, at a p-value < 0.05. Between April 2017 and March 2018, we received 148 (30%) responses. A total of 35% (n = 51) of respondents indicated that they walked recreationally for exercise compared to 65% (n = 94) who did not. Characteristics that were significantly associated with walking included regularly saving money (adjusted odds ratio (aOR) = 10.7, p = 0.001), seeking complex problem-solving (aOR = 0.12, p = 0.002), and severe symptoms (aOR = 0.24, p = 0.017). Individuals describing a preference for the future rather than immediate benefit also reported currently walking for exercise. Defining the characteristics of those who exercise may help inform strategies designed to increase walking among those who do not adhere to recommendations.
Keywords
Introduction
Claudication (reproducible calf pain that occurs when walking) affects approximately 20–40 million people worldwide, 1 with the prevalence increasing fourfold as a person ages. 2 In addition to surgery, exercise – particularly walking – is an established and effective treatment for claudication.3,4 Despite this, the number of people with claudication who adhere to exercise recommendations is relatively low. 2 Identifying factors that explain adherence in a cohort of individuals whose ability to walk is impeded by pain would streamline strategies aimed at increasing walking and improving patient-perceived quality of life.5–8
In the past decade, economists have demonstrated that rational models driven by theory-based economics are poor predictors of human decision-making. 9 Rather, behavioral economics10–16 that incorporate psychological and cognitive factors better describe individual decision-making in repeated and predictable ways. 9 Using existing decision-drivers identified in the context of exercise behavior could help broadly distinguish between cohorts willing and unwilling to exercise. For example, intertemporal choice is a behavioral economics concept that describes the value placed on immediate reward versus future, greater rewards. 17 Recent studies have demonstrated the influences that intertemporal choices have on adherence to physical activity recommendations. 13 Individuals oriented to immediate benefits over future utility – characteristics that could be measured using current behaviors – may be less likely to implement treatment recommendations whose benefits have lower immediate return but increased future yield. From a clinical perspective, developing a brief model may be useful in identifying individuals at a higher risk of failing to accept exercise recommendations, thereby taking the first step in highlighting a path forward for both provider and patient. The objective of this study was to examine the efficacy of behavioral economics-associated characteristics, while accounting for other related factors, in describing walking behavior in a cohort of Veterans with claudication.
Methods
Eligible participants were identified by reviewing clinic lists for patients who were diagnosed with claudication between January 2013 and December 2015. Through a cross-sectional study design, participants completed surveys that were mailed to their home addresses. A survey was mailed to a patient if they were: (1) older than 50 years, and (2) received care or an initial confirmed diagnosis by a board certified vascular surgeon from the Michael E. DeBakey Veterans Affairs Medical Center in Houston, Texas. We excluded patients who were diagnosed with rest pain and toe pressures of < 50 mmHg. Patients with tissue loss of the foot or leg (ulcer, gangrene, or other non-health wound) were also excluded. Patients with a history of intervention for claudication were not excluded to examine associations between receiving an intervention and activity. Using a priori sample size calculations that accounted for a response rate of 30%, 18 500 surveys were mailed out to individuals who met the eligibility criteria. Data collection was completed through (1) a review of the medical record for information on co-morbidities, and (2) a self-reported survey on behavioral and psychological predictors of adherence to physical activity. The Baylor College of Medicine’s Institutional Review Board (H-40824) and the Veterans Affairs Research and Development Committee (17E01.H) approved a waiver of informed consent. Participants were advised return of the survey indicated acceptance of participation in the study and were provided pre-paid envelopes. Compensation for completing and returning the survey was not provided. An alternative hypothesis examining whether successful smoking cessation was associated with current walking behavior was described using the same patient population and methodology. 19 The primary and secondary outcomes described in this manuscript are unique and exclusive from those described previously.
Primary outcome
Owing to the self-reported nature of the measure, the primary outcome – exercise – was validated through multiple sources. Total physical activity scores were calculated as a product of frequency (days per week spent walking and time per day spent walking) and intensity (slow, moderate, fast). 20 To further validate this continuous physical activity measure, responses were only counted if participants indicated that they walked specifically for exercise.
Binary variables, informed by the Compendium of Physical Activities, 20 were used to measure: current walking (current walker vs non-current walker), regular walking: walking for at least 30 minutes per day over the past 6 months (regular walker vs non-regular walker), and receiving surgical intervention for claudication-related peripheral artery disease (PAD). Questions about walking behavior were phrased to distinguish between recreational and utilitarian walking and an individual was classified as a walker if they reported walking specifically for exercise. The primary model was constructed on the variable measuring current walking.
Exposure variable measurements
A survey was designed using validated measures of (1) symptom severity, (2) health-related quality of life, (3) behavioral economics, (4) perceived stress, (5) fear-avoidance beliefs, (6) depression, and (7) stages of health behavior change. Specifically, the distance and speed subscales of the Walking Impairment Questionnaire (WIQ), 21 and the Intermittent Claudication Questionnaire 22 were used to measure symptom severity and health-related quality of life, respectively. The Barratt’s Impulsivity Questionnaire (BIS), 23 Cohen’s Perceived Stress Scale 4, 24 Fear-Avoidance Beliefs Questionnaire, 25 and the Center for Epidemiologic Studies Depression Scale (CES-D) 26 were used to measure the economics of behavior, stress, and depression, respectively. In particular, the self-control and cognitive complexity (11 items) subscales of the 30-item BIS measured nonplanning, while the attentional and motor subscales were excluded for the purposes of this study. The BIS questionnaire has been used extensively to quantify impulsivity, and its reliability and validity has been tested across age groups and demographics.27–29 A validated, short-form version of the Cohen’s Perceived Stress Scale was used to assess the perception of stress in an easily interpreted format. The CES-D is a highly sensitive measure of depression that is assessed across a 20-point scale. (Online Supplemental Table 1 provides further detail on study measures.) Finally, questions based on the concepts outlined in the Transtheoretical Model 30 – pre-contemplation, contemplation, preparation, decision/action, and maintenance – were used to measure the individual’s stage of physical activity behavior change. Medical history data were abstracted from the medical records. The Area Deprivation Index (ADI) – a measure of socioeconomic deprivation – was derived from the participant’s zip+4 code and used as a measure of socioeconomic status. 31 Responses to each of these questionnaires, both subscale scores and individual items, were examined for their ability to explain the likelihood of an individual’s current or regular walking.
Statistical analysis
Data were described using counts, proportions, means, and SD. Pearson’s-χ2 and t-tests or its non-parametric counterpart – the Wilcoxon rank-sum test – were used to conduct univariable comparisons between categorical and continuous independent variables for characteristics of the study population. Contingent on the dependent variable, univariable linear and logistic regressions were used to first identify significant variables at a p-value < 0.10. Multivariable associations were described by retaining variables that were statistically and clinically significant. Variables were tested to maximize model fit by examining the area under the receiver operating characteristic (ROC) curves (AUC), and the likelihood-ratio test was also used to improve model fit while developing multivariable models. Model assumptions including linearity and multi-collinearity between the independent variables in the final models were examined. Interactions between potential effect modifiers were examined prior to finalizing models. Data management and analyses were conducted using Stata 13 software (StataCorp LP, College Station, TX, USA).
Results
Descriptive characteristics of the study population
Between April 2017 and March 2018, 500 surveys were mailed to potential participants across the United States. Responses were received from 148 participants (30%). Respondents were a representative sample (with respect to sex and race/ethnicity) of the total population of survey recipients (male respondents = 97% vs male recipients = 98%; non-Hispanic white respondents = 66% vs non-Hispanic white recipients = 59%; African American respondents = 31% vs African American recipients = 36%). The mean age was 70 years (SD = 6.3 years). The proportion of participants with a history of hypertension, hyperlipidemia, diabetes, and coronary artery disease did not significantly vary between reports of walking for exercise (Table 1). Among non-walkers, median self-reported symptom severity was higher for both the speed and distance subscales of the WIQ. Online Supplemental Table 2 describes characteristics across four potential walking groups (non-walker, current and regular walker, current walker only, and past walker only).
Demographic, psychological, and cognitive characteristics of individuals reporting walking every day for exercise.
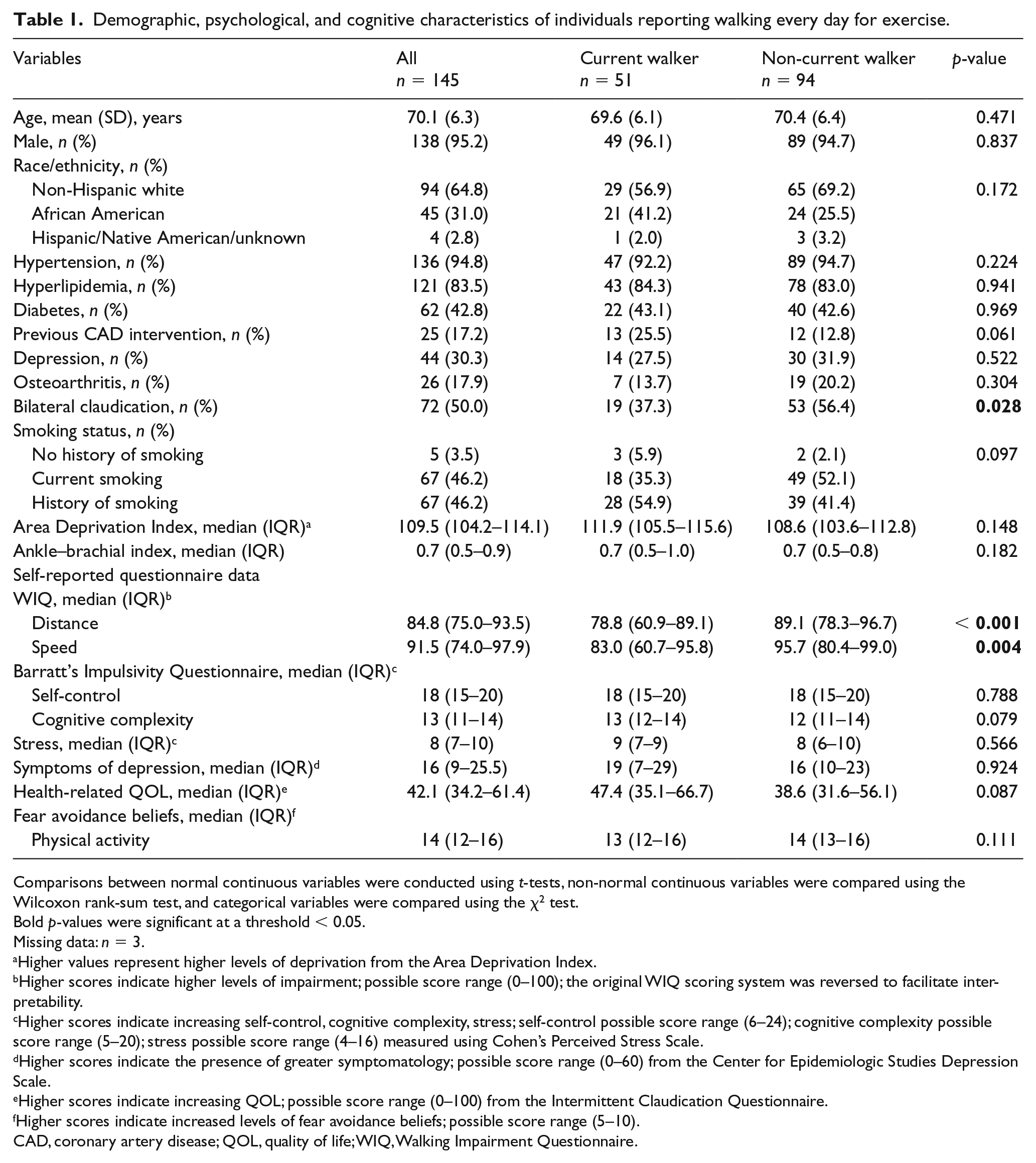
Comparisons between normal continuous variables were conducted using t-tests, non-normal continuous variables were compared using the Wilcoxon rank-sum test, and categorical variables were compared using the χ2 test.
Bold p-values were significant at a threshold < 0.05.
Missing data: n = 3.
Higher values represent higher levels of deprivation from the Area Deprivation Index.
Higher scores indicate higher levels of impairment; possible score range (0–100); the original WIQ scoring system was reversed to facilitate interpretability.
Higher scores indicate increasing self-control, cognitive complexity, stress; self-control possible score range (6–24); cognitive complexity possible score range (5–20); stress possible score range (4–16) measured using Cohen’s Perceived Stress Scale.
Higher scores indicate the presence of greater symptomatology; possible score range (0–60) from the Center for Epidemiologic Studies Depression Scale.
Higher scores indicate increasing QOL; possible score range (0–100) from the Intermittent Claudication Questionnaire.
Higher scores indicate increased levels of fear avoidance beliefs; possible score range (5–10).
CAD, coronary artery disease; QOL, quality of life; WIQ, Walking Impairment Questionnaire.
Physical activity and walking
The primary model was constructed using participant responses to whether they currently walked for exercise. A total of 51 (35%) people indicated that they reserved a dedicated time to walk for exercise compared to 94 (65%) who did not walk for exercise. Among those who currently walked for exercise (n = 50), 22 individuals (44%) reported that they had followed this routine for at least 30 minutes every day for the past 6 months. Median walking time, among walkers, was 5 days per week and median walking time per day was 45 minutes (Table 2). Stage of physical activity behavior change compared between walkers and non-walkers is provided in Table 3.
Variables describing total activity and walking.
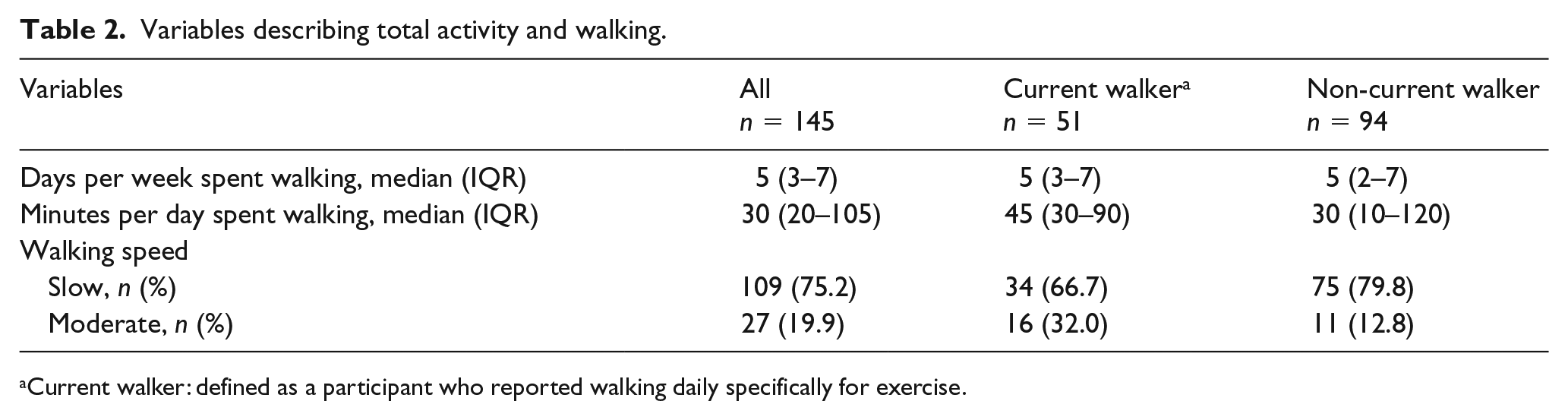
Current walker: defined as a participant who reported walking daily specifically for exercise.
Stages of change for walking.
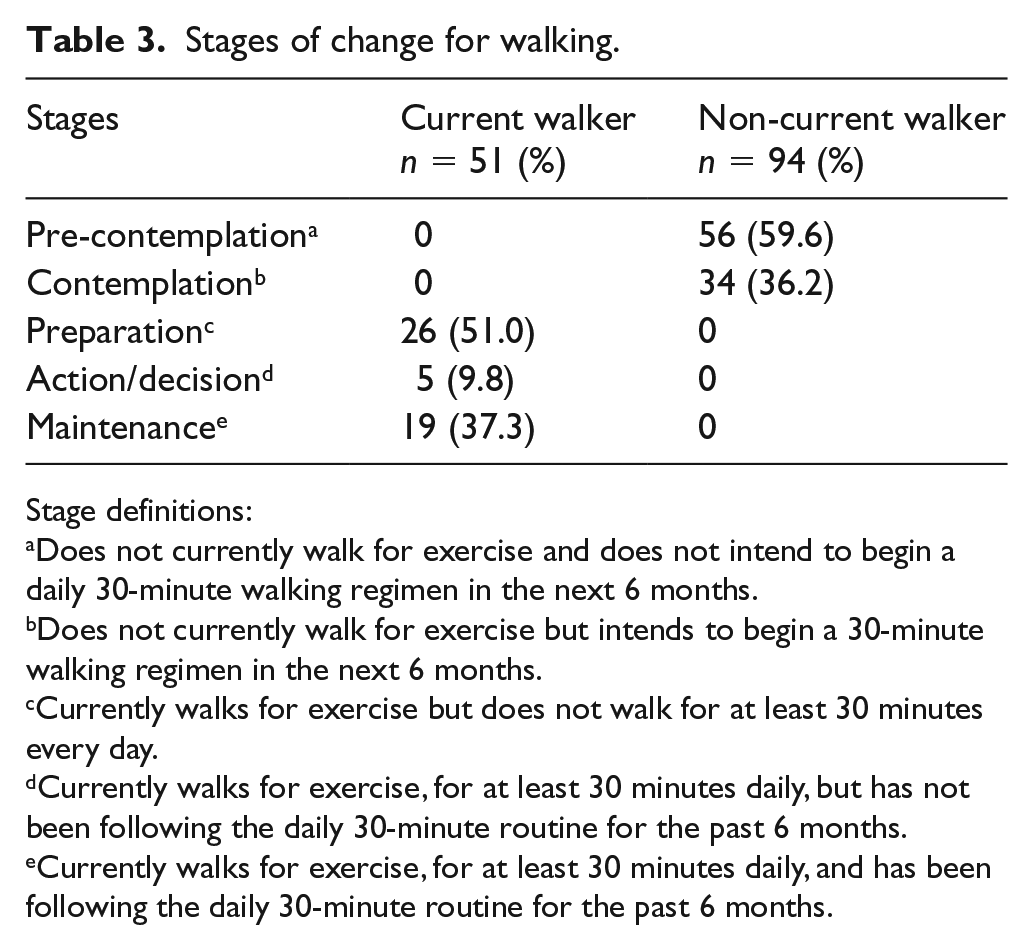
Stage definitions:
Does not currently walk for exercise and does not intend to begin a daily 30-minute walking regimen in the next 6 months.
Does not currently walk for exercise but intends to begin a 30-minute walking regimen in the next 6 months.
Currently walks for exercise but does not walk for at least 30 minutes every day.
Currently walks for exercise, for at least 30 minutes daily, but has not been following the daily 30-minute routine for the past 6 months.
Currently walks for exercise, for at least 30 minutes daily, and has been following the daily 30-minute routine for the past 6 months.
Factors associated with current walking
In describing the characteristics of individuals who reported currently walking for exercise, self-reported symptom severity, African American race, and the behavioral economics-related concepts of complex thinking and financial planning were significant descriptors (Table 4). When BIS total subscale scores were assessed in the multivariable model, a significant association was not observed between cognitive complexity, self-control, and current walking. Individual questions of the subscales were introduced in the model to further examine associations. Participants who reported saving money regularly were 10 times more likely to report setting aside time to walk compared to those who never saved (adjusted odds ratio (OR): 10.7, p = 0.001). Similarly, complex thinking, as measured by interest in complex problem-solving, was a significant indicator of walking for exercise. In other words, walkers were less likely to avoid complex problem-solving compared to non-walkers (adjusted OR: 0.12, p = 0.002). Ankle–brachial indices (ABIs) of the most symptomatic leg did not contribute significantly to explaining the variation observed in the dataset.
Variables associated with factors describing individuals who reported walking every day for exercise based on a multivariable regression model (current walker vs non-current walker).
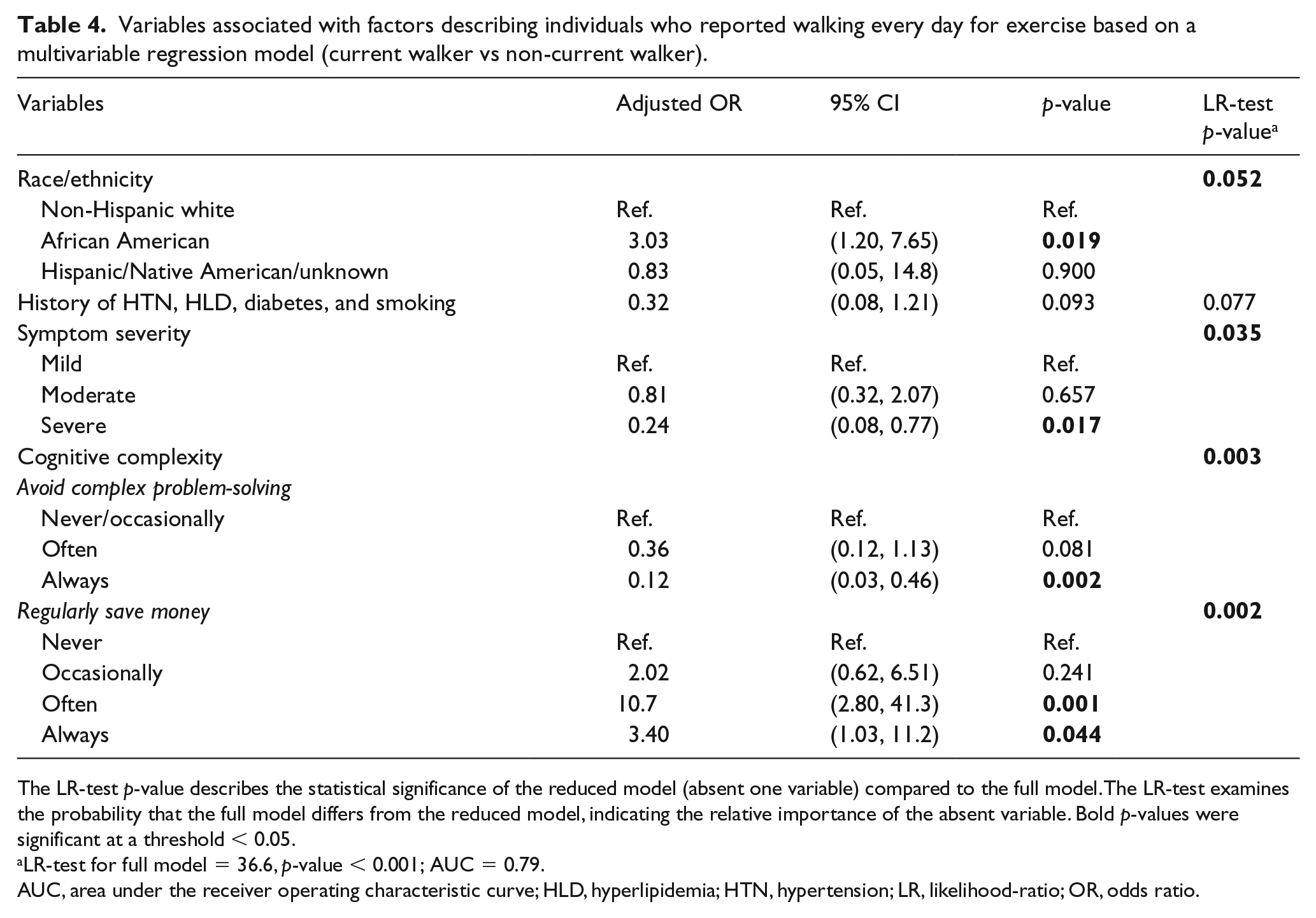
The LR-test p-value describes the statistical significance of the reduced model (absent one variable) compared to the full model. The LR-test examines the probability that the full model differs from the reduced model, indicating the relative importance of the absent variable. Bold p-values were significant at a threshold < 0.05.
LR-test for full model = 36.6, p-value < 0.001; AUC = 0.79.
AUC, area under the receiver operating characteristic curve; HLD, hyperlipidemia; HTN, hypertension; LR, likelihood-ratio; OR, odds ratio.
Factors associated with regular walking
In the univariable analysis, factors that were significantly associated with a history of walking included health-related quality of life, diabetes, and total cognitive complexity. On further examination of the specific cognitive complexity aspects that described a regular walker, we found that participants who reported walking daily for at least 30 minutes over the previous 6 months were more likely to report saving money regularly (adjusted OR: 5.9, p = 0.006) and enjoy puzzle-solving (adjusted OR: 3.7, p = 0.042). The final multivariable model describing a regular walker was adjusted for hypertension, hyperlipidemia, diabetes, current smoking, body mass index (BMI) categories, and self-reported symptom severity (Table 5).
Variables associated with individuals who reported walking for at least 30 minutes every day for the past 6 months based on a multivariable regression model (regular walker vs non-regular walker).
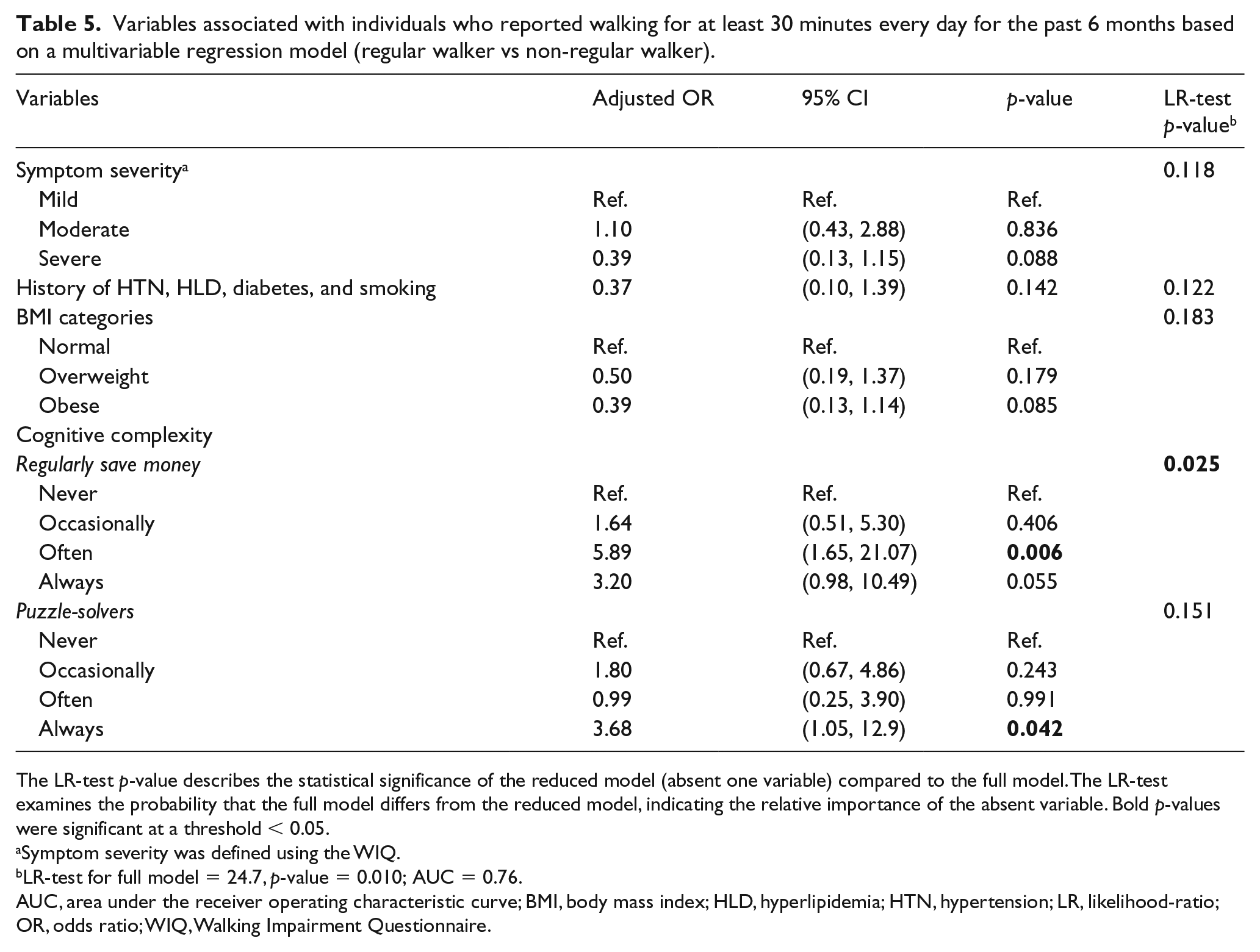
The LR-test p-value describes the statistical significance of the reduced model (absent one variable) compared to the full model. The LR-test examines the probability that the full model differs from the reduced model, indicating the relative importance of the absent variable. Bold p-values were significant at a threshold < 0.05.
Symptom severity was defined using the WIQ.
LR-test for full model = 24.7, p-value = 0.010; AUC = 0.76.
AUC, area under the receiver operating characteristic curve; BMI, body mass index; HLD, hyperlipidemia; HTN, hypertension; LR, likelihood-ratio; OR, odds ratio; WIQ, Walking Impairment Questionnaire.
Factors associated with receiving a surgery to relieve claudication symptoms
Surgical intervention (either endovascular or open revascularization) was identified in 49% (72/146) of the cohort. Participants who received an intervention were older and reported experiencing severe symptoms (Table 6). From a previous secondary analysis, 32 we hypothesized that knowing a friend or relative who received an intervention would be associated with an intervention; however, this was not the case in this cohort. We also expected that a belief in the benefit of surgical intervention may be associated with the receipt of intervention. Among those who had not received an intervention, belief in the benefit of surgery was 42% (31/74). Fifty-one individuals (71%) who had previously received surgery indicated that they experienced beneficial improvements. Importantly, among those with a surgical history, a greater proportion reported that they did not currently walk for exercise (45/72, 63%). ABIs were included in the final model as they improved the model fit; however, this variable was not significantly associated with the likelihood of receiving a surgical intervention.
Variables associated with receiving an intervention for PAD-related claudication based on a multivariable regression model.
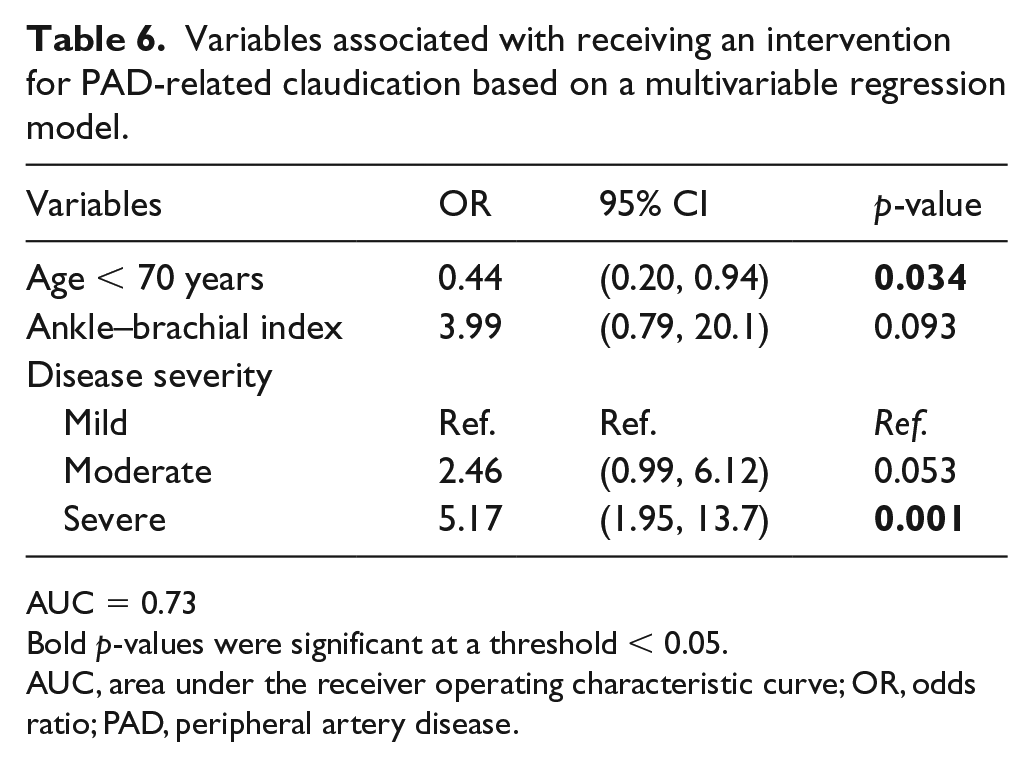
AUC = 0.73
Bold p-values were significant at a threshold < 0.05.
AUC, area under the receiver operating characteristic curve; OR, odds ratio; PAD, peripheral artery disease.
Symptom severity and stage of change for walking
Finally, we examined the association between stage of change and self-reported symptom severity. In a model adjusted for hypertension, hyperlipidemia, diabetes, total activity, BMI, and ABIs, the likelihood of being classified in the maintenance phase decreased as symptom severity increased (WIQ distance: mean difference = −15.6, p = 0.002; WIQ difficulty: mean difference = −10.8, p = 0.010).
Discussion
Walking is a non-invasive, effective treatment for symptomatic PAD. Because of the wide-ranging benefits of exercise and its cost-effectiveness,33–36 studies have emphasized the similar efficacy and effectiveness of supervised exercise therapy (SET) compared to surgical intervention in patients with claudication.37–39 Recent American Heart Association and American College of Cardiology guidelines recommend structured exercise therapy as a first-line management option for claudication – particularly, physical activity that is beyond utilitarian. 40 Home-based walking is a beneficial alternative to SET that more closely simulates daily over-ground walking.37,41
Despite the breadth of literature highlighting the efficacy of SET and home-based exercise, critical barriers to the effectiveness of these treatments – adherence and recommendation acceptance – remain problematic. Access to SET through Centers for Medicare and Medicaid 42 reimbursement has simplified exercise prescription; yet, the issue of adherence is unresolved. Previous SET studies demonstrate that individuals who were offered exercise through the study at no incurred cost declined participation in large proportions, suggesting that the effects of increasing access may be attenuated. In the context of our study on home-based walking, we noted that a significant proportion of participants (64%) did not routinely walk for exercise.
Given the challenges associated with adherence, it is important to incorporate concepts designed to increase adherence in the numerous proposed home-based and SET interventions. Even broadly classifying and targeting appropriate interventions to those who have a proclivity to walking based on existing habits, compared to those who have characteristics that put them at higher risk of failing to adhere, may help increase adherence rates. Often, physical, environmental barriers are given more attention than some of the more innate, intangible obstacles of behavioral change. As behavioral patterns most extensively impact overall survival, 43 the implications of behavioral algorithms on physical activity are naturally significant. Discounting the effect of existing behavioral patterns contributes to an ineffective cycle of encouraging new behavior change with interventions that are inherently dependent on other fundamental behavioral characteristics. 44 This study attempts to utilize markers of existing behavioral patterns to describe individuals who were less likely to identify as current or regular walkers, given the recommendation to walk for exercise.
To ensure appropriate model specification, we examined factors that were closely associated with health behavior change and symptom characteristics (i.e., leg pain), including depression, stress, fear avoidance beliefs, and health-related quality of life. In line with the primary objective of this study, we assessed the effects of previous habits or behaviors as a marker for future behaviors using concepts attributed to behavioral economics.12,13,45 We found that a ‘walker’ was less likely to (a) report severe subjective symptoms, (b) avoid complex problem-solving, and was more likely to (c) save money regularly. These characteristics highlight that the concept of intertemporal choices – where present benefit is preferred over delayed benefit – is especially applicable when exercise (delayed benefit) is recommended over surgical intervention (immediate benefit).46,47 In this study, we quantified intertemporal choices by asking participants about their saving habits and gauged their interest in activities that inherently required patience and tenacity (i.e., complex problem-solving, puzzle-solving, etc.). Our study is similar to Shuval et al.’s examination of behavioral economic associations with increased levels of physical activity among low-income adults in minority populations. 13 We found that individuals reporting regular savings and interests in complex problem-solving describe a view toward future benefit rather than immediate reward. Similar characteristics were observed when describing factors associated with a history of walking: regular saving and puzzle-solving. Among the range of factors that were examined, the most significantly predictive descriptors of walking were factors measuring intertemporal choices. In interpreting our findings, it is important to note that the overall BIS subscale scores (i.e., self-control and cognitive complexity) did not significantly differ between groups. While it is indisputable that the subscale scores are the most complete assessment of the given characteristics, our sample may be susceptible to a lack of variability sourced from a response bias. The study is also limited with respect to the power, and the broad definition of our outcome variable may not definitively delineate the two groups. We did not, however, want to discount the contribution of specific questions in describing the variability between groups – especially as the responses that were significant captured behaviors that emphasized delayed benefit. We also noted that these responses were significant in both the currently walking and regularly walking groups. This replication gives some credibility to a signal of association between these characteristics and walking behavior. To further contextualize our results, we acknowledge that other sources of residual confounding related to the associations between savings and walking include direct measures of income, employment status, financial burden, and social support. Finally, we report that individuals identifying as black or African American were more likely to report walking when compared to individuals identifying as white or Caucasian. This is a fairly unique finding in the physical activity literature. Unless these findings are replicated, we could attribute this association to a combination of the relatively smaller proportion of African American individuals in the sample and some aspects of response bias. Although, the possibility that this is a true association also cannot be discounted at this stage in the context of this question.
Apart from statistical thresholds, we also considered the practicality of the model that we were developing (i.e., time to complete, information requested, and likelihood of accurate responses). With respect to the measure of physical activity, although we collected self-reported data on daily physical activity, we observed repeated instances of over-estimation – a problem that has been previously reported in the activity literature. 48 Lacking quantitative daily activity data and considering the inaccuracy of self-reported data, we used a simple yes or no question that is already asked in clinic on a routine basis (‘do you currently walk for exercise?’) to measure activity. By explicitly asking about walking for exercise, we emphasized the difference between recreational walking and walking as part of daily routine activities (utilitarian walking) – a factor that could potentially explain the overestimation in total activity. Acknowledging that the our subjective measure of activity limits the immediate applicability of our findings, we intend to validate our results using quantitative measures that will help inform future interventions specifically targeted to our population of interest.
Limitations and strengths
Some limitations of this study include those that are inherent to the cross-sectional study design. We cannot comment on how these behavioral reports change over time or fully account for confounding factors that are best adjusted for using randomized controlled trials. We also interpret the association between saving and walking cautiously in the context of a potential for residual confounding from data unavailable in our study. Particularly, we were unable to directly examine the effects of income, occupation, and financial status. The National Bureau of Labor Statistics indicate that 81.7% of the Veteran population aged 65 years and over are no longer in the labor force 49 – data that may be extrapolated to describe the employment status of individuals who responded to this study’s survey. However, we anticipate that the Area Deprivation Index (a measure of geographic area-based disadvantage) conservatively addressed some of the potential bias. In addition, the sampling frame for this study, limited largely to male, non-Hispanic white Veterans, impedes our ability to generalize these results. Because of the specific nature of our target population, caution is necessary when extrapolating the results of this study to cohorts that are dissimilar to ours. To our knowledge, this is the first study in the PAD literature that examines concepts of behavioral economics in the context of walking behavior. Another unique aspect of the study is that it approaches physical activity behavior change from the perspective of optimizing an individual for the intervention most beneficial rather than attempting to generally target activity barriers.
Conclusion
We identified the intertemporal choices of regular saving habits, complex problem-solving, and subjective symptom severity as predictors associated with walking behavior (current and previous). Results from this study may be used to identify patients with claudication who are at risk for failure to adhere to walking recommendations. Once identified, these patients could be offered focused support and counseling designed to enhance adherence to an exercise regimen.
Supplemental Material
10.1177_1358863X19865610_Supplemental_tables – Supplemental material for Delayed gratification and adherence to exercise among patients with claudication
Supplemental material, 10.1177_1358863X19865610_Supplemental_tables for Delayed gratification and adherence to exercise among patients with claudication by Sherene E Sharath, MinJae Lee, Panos Kougias, Wendell C Taylor, Nader Zamani and Neal R Barshes in Vascular Medicine
Footnotes
Acknowledgements
This work is based on a presentation at the Scientific Forum of the American College of Surgeons Clinical Congress, Boston, MA, USA in October 2018.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.