
Abstract
Venous thromboembolism (VTE) and coronary artery disease are major health issues that cause substantial morbidity and mortality. New data have emerged suggesting that these two conditions could have a close relationship. Thus, we sought to determine the trends in annual rate of VTE occurrence in patients with ST-segment elevation myocardial infarction (STEMI) and measure its impact on in-hospital mortality, bleeding complications, and cost and length of hospitalization. We queried the 2003–2013 Nationwide Inpatient Sample databases to identify adults with primary diagnosis of STEMI. VTE events were then allocated. Inpatient outcomes of patients with VTE were compared to those without VTE. Out of 2,495,757 hospitalizations for STEMI, VTE was diagnosed in 25,149 (1%) hospitalizations. Patients who experienced VTE were older (mean age: 67.5 vs 64.8, p < 0.01) and had a higher proportion of black patients (10.1% vs 7.7%, p < 0.001) and females (40.1% vs 35%, p < 0.001) compared to patients without VTE. There was an increasing trend in the rate of VTE during the study period (2003: 0.8% vs 2013: 1.0%, p < 0.001). Patients with VTE had a prolonged hospitalization (median: 9 vs 3 days, p < 0.001), increased cost, higher risk of gastrointestinal bleeding (OR: 2.13, p < 0.001), intracranial hemorrhage (OR: 2.14, p < 0.001), blood transfusions (OR: 1.94, p < 0.001), and mortality (OR: 1.39, p < 0.001). The rate of VTE occurrence in patients with STEMI in our study was 10 per 1000 admissions. VTE was associated with more bleeding complications, longer hospital stays, higher costs, and mortality. These findings suggest that a more aggressive approach for VTE prophylaxis may be warranted in this population.
Keywords
Introduction
Venous thromboembolism (VTE) and coronary artery disease (CAD) cause substantial morbidity and mortality and increase healthcare expenses significantly.1,2 Historically, VTE and atherosclerotic cardiovascular disease have been studied and managed as two different processes. Venous thrombosis, formed mainly by fibrin, has been linked with risk factors such as immobility, trauma, malignancy, and genetic factors, 3 whereas arterial thrombosis, formed primarily by platelets, has typically been attributed to conditions responsible for atherosclerosis like diabetes, hypertension, hyperlipidemia, and tobacco smoking. 4 New data have emerged suggesting that these two conditions could have a closer relationship involving a common underlying pathophysiological mechanism. This relationship is not well understood, and it remains unclear whether there is a common intrinsic biomolecular mechanism. This hypothesis is supported by data from studies such as the Pulmonary Embolism Prevention trial, in which antiplatelet drugs decreased VTE occurrence. 5 Similarly, a meta-analysis showed that statins can reduce the rates of VTE. 6 Hence, we sought to determine the rate of VTE events and its impact on mortality, bleeding complications, cost, and length of hospitalization in patients admitted for ST-segment elevation myocardial infarction (STEMI) and to investigate the underlying risk factors that could potentially play a role in the development of these two conditions.
Methods
Data source
Data were obtained from National Inpatient Sample (NIS) database files. The NIS is part of the Healthcare Cost and Utilization Project (HCUP), a family of healthcare databases and related software tools and products developed through a federal/state/industry partnership and sponsored by the Agency for Healthcare Research and Quality (AHRQ). The NIS is the largest publicly available all-payer inpatient healthcare database in the United States, yielding national estimates of hospital inpatient stays. It consists of a stratified systematic sample of discharges from all hospitals in HCUP, equal to approximately 20% of all discharges in US community hospitals. The NIS contains information on patient demographics, discharge diagnoses, procedures, outcomes, comorbidities, and hospital characteristics. The NIS provides discharge weights to produce regional or national estimates. 7 Weighted, it estimates more than 35 million hospitalizations per year nationally. We used modified discharge weights (trend weights) provided by the NIS for years prior to 2012 to obtain accurate national estimates. 8
Study population
We analyzed NIS databases from 2003 to 2013 to identify all patients ⩾ 18 years old admitted with STEMI as their primary diagnosis. STEMI was defined by International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) codes 410.01, 410.11, 410.21, 410.31, 410.41, 410.51, 410.61, 410.81, and 410.91. This method has been used in multiple studies previously to accurately identify patients with a principal diagnosis of STEMI.9,10 Subsequently, we identified patients who developed VTE using ICD-9-CM codes 415.1, 415.11, 415.13, and 415.19 for pulmonary embolism; 451.11, 451.19, 451.2, 451.81, 453.40, 453.41, and 453.42 for deep vein thrombosis (DVT) of the lower extremity; and 451.83, 451.84, 451.89, 453.2, 453.3, 453.8, 453.9, 453.82, 453.83, 453.84, 453.85, 453.86, 453.87, and 453.89 for VTE of other locations. Superficial and splanchnic vein thromboses were excluded. VTE events were allocated if present in any of the NIS’s 24 secondary diagnoses positions. ICD-9-CM codes for VTE have a positive predictive value of 95% when present in the principal position, and 75% when present in a secondary position. 11
Patient and hospital variables
Patients’ baseline characteristics were obtained using variables provided by the NIS databases. These consisted of demographics (age at admission, sex, and race), Elixhauser comorbidities as defined by the AHRQ, 12 and other relevant clinical comorbidities (dyslipidemia and smoking). The NIS database provides 29 comorbid conditions (Elixhauser comorbidities), which are identified using ICD-9-CM codes and the Diagnosis Related Group in effect on the discharge date. These comorbidities are considered as coexisting medical conditions that are not related directly to the principal diagnosis, and are likely to have existed prior to the hospital stay. 13 ICD-9-CM codes used by the NIS to ascertain these comorbidities can be found in the supplementary document. The NIS variables ‘Metastatic cancer’, ‘Solid tumor without metastasis’, and ‘Lymphoma’ were grouped into a single variable that we named ‘Malignancy’. Moreover, hospital characteristics (bed size, location/teaching status, and region of the hospital) were included.
Outcomes definition
Our primary aim was to determine inpatient outcomes including mortality, bleeding complications, average length of stay, and hospitalization cost. Bleeding complications were defined as intracranial bleeding, gastrointestinal bleeding, and the need for blood transfusions. The accuracy of the ICD-9-CM codes used to define intracranial bleeding was reported to be 94.7% in a validation study. 14 The clinical classification codes used to identify gastrointestinal bleeding and blood transfusion were developed and provided by the AHRQ, and have been used in multiple studies.15,16 We also aimed to measure the annual rates of VTE in hospitalized patients admitted with STEMI and evaluate the temporal trends in annual rates of VTE events during the study period. The ICD-9-CM and Clinical Classification Software codes used to identify outcomes are listed in Supplementary Table 1.
Statistical analysis
Discharge weight provided by the NIS was applied to unweighted data to infer national estimates. Weighted data were used in all analyses. We used descriptive statistics to summarize the distribution of baseline parameters and hospital characteristics. Continuous variables are expressed as mean ± SD or median and IQR according to normality. Categorical variables are expressed by the absolute numbers and percentages. To ascertain differences between VTE and non-VTE patients, we used the Pearson chi-squared test, independent t-test, and Mann–Whitney U test as appropriate. We used binary-logistic regression to explore the association between VTE and inpatient outcomes such as in-hospital mortality and bleeding complications. First, we conducted a univariate analysis, and variables significantly associated to our outcomes (p < 0.1) were moved to our multivariate model. We adjusted for demographics, clinical comorbidities, and hospital characteristics. Length of stay was not included in our regression models. All variables that were used in constructing the regression models are listed in Supplementary Table 2. For trend analyses, multivariable logistic regression, adjusted for demographics, comorbidities, and hospital characteristics, was used to assess whether outcomes changed over time. The variable ‘year’ was included as a continuous variable to obtain the adjusted odds ratio (OR) per year.
The Mann–Whitney U test was used to assess the difference in length and cost of stay between patients with and without VTE.
All statistical analyses were conducted using IBM SPSS Statistics 23.0 (IBM Corp., Armonk, NY, USA). All p-values were two sided and statistical significance was defined as p < 0.05.
Results
Baseline patient characteristics
Between the years 2003 and 2013, a total of 2,495,757 STEMI cases were identified. Of these, the majority were men (65%) and white (79%) with a mean age of 64.8 ± 14.5 years. Close to half of the cases (44.9%) were admitted to urban teaching hospitals. Hypertension (57.8%), dyslipidemia (49.4%), smoking (36.3%), and diabetes (27%), were the most prevalent comorbidities (Table 1).
Baseline characteristics of the patients.
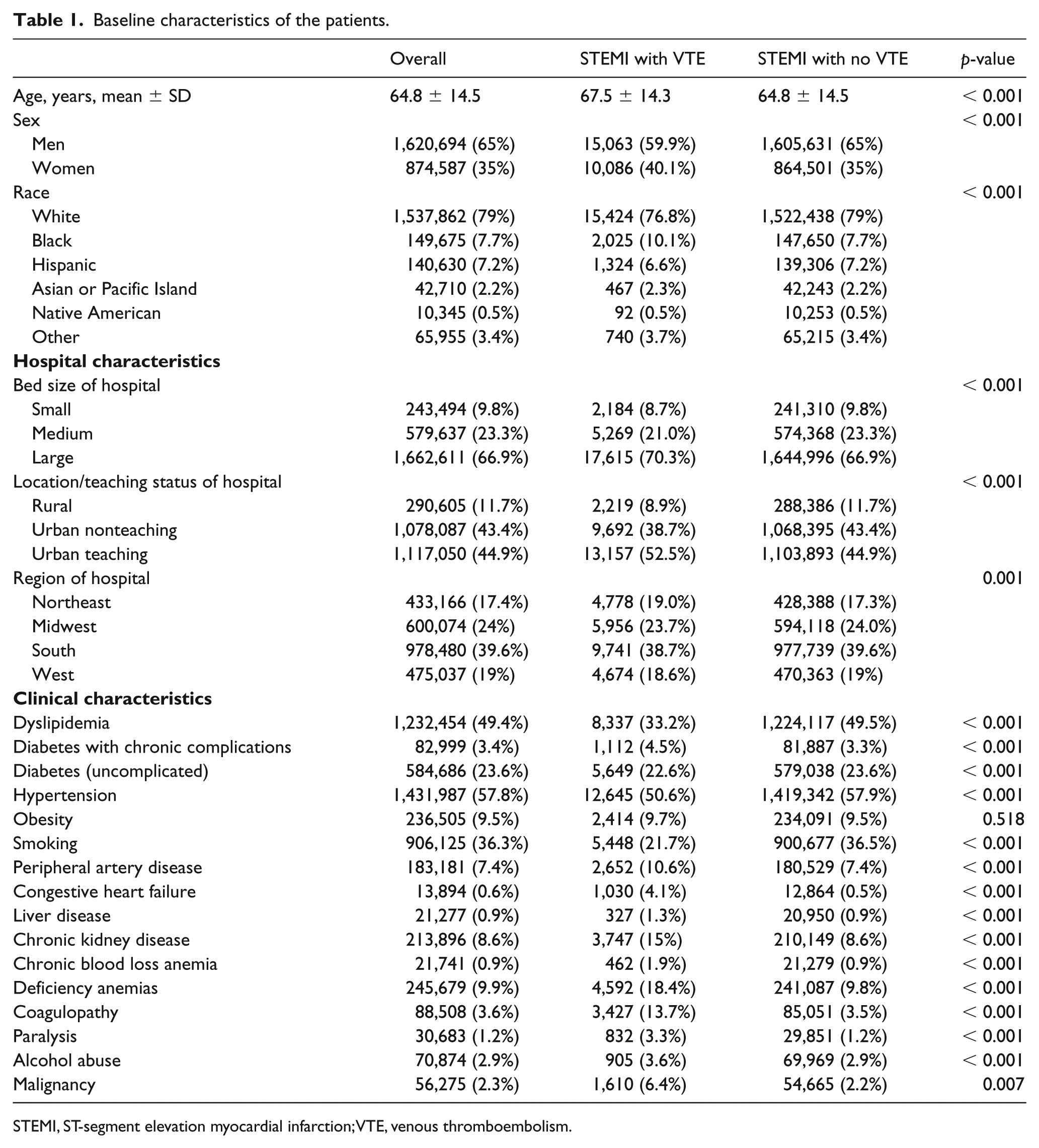
STEMI, ST-segment elevation myocardial infarction; VTE, venous thromboembolism.
VTE rates
Of 2,495,757 hospitalizations for STEMI, 25,149 (1%) experienced a VTE event. Pulmonary embolism was noted in 8134 (0.3%) patients, while lower extremity and other locations VTE were observed in 7852 (0.3%) and 11,391 (0.5%) patients. The main reason for the higher number of VTE at other locations was ICD-9 code 435.8 (thrombosis of other specified vein). Compared to patients without VTE, those who experienced VTE were older patients (mean age: 67.5 vs 64.8, p < 0.001) and there were a higher proportion of black patients (10.1% vs 7.7%, p < 0.001) and females (40.1% vs 35%, p < 0.001). Rates of VTE increased slightly from 0.8% in 2003 to 1.0% in 2013 (Figure 1) (unadjusted OR per year: 1.021, 95% CI: 1.017–1.025, p-trend < 0.001); the trend remained significant after adjusting for demographics, clinical comorbidities, and hospital characteristics (adjusted OR per year: 1.036, 95% CI: 1.032–1.040, p-trend < 0.001). Independent predictors of VTE included older age (OR: 1.001, p = 0.039), female sex (OR: 1.11, p < 0.001), history of congestive heart failure (OR: 4.19, p < 0.001), malignancy (OR: 2.35, p < 0.001), coagulopathy (OR: 3.07, p < 0.001), and paralysis (OR: 2.11, p < 0.001). Whereas, smoking (OR: 0.56, p < 0.001) appeared to have a protective effect (Table 2).
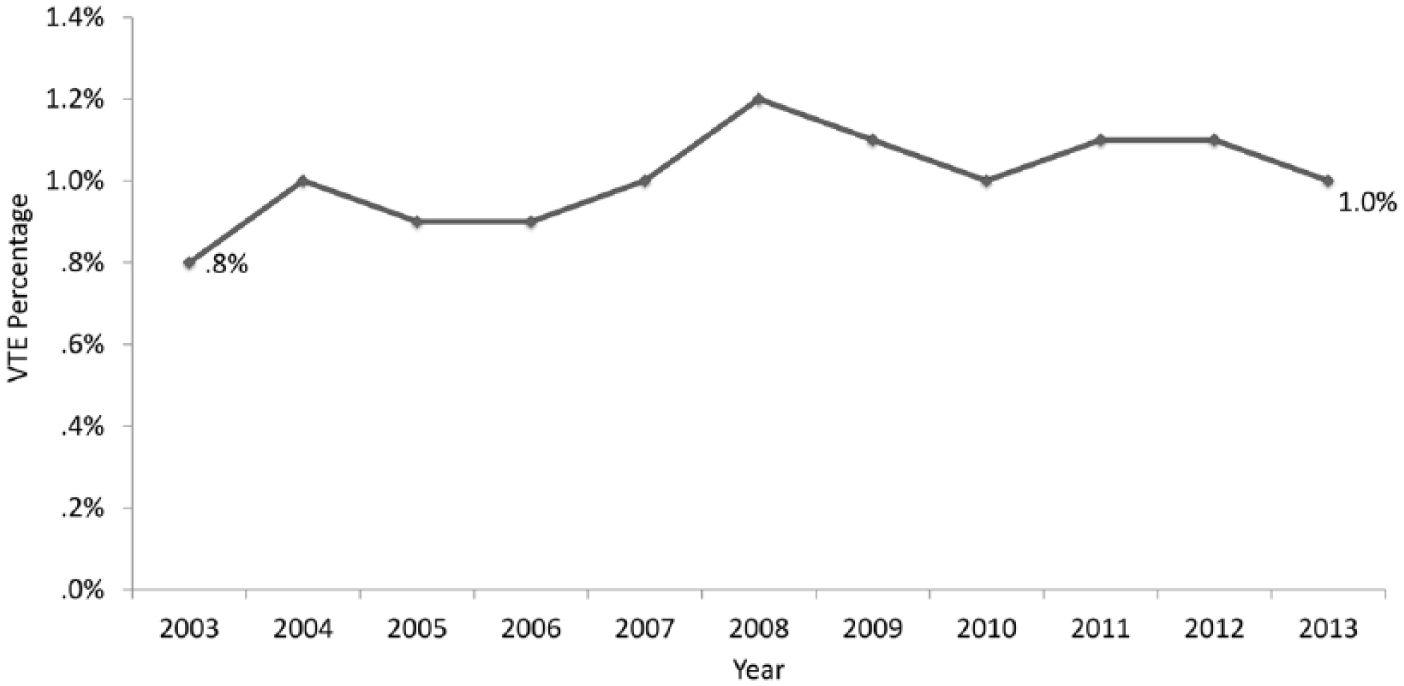
Temporal trend of VTE rates in patients with STEMI between 2003 and 2013.
Predictors of VTE.
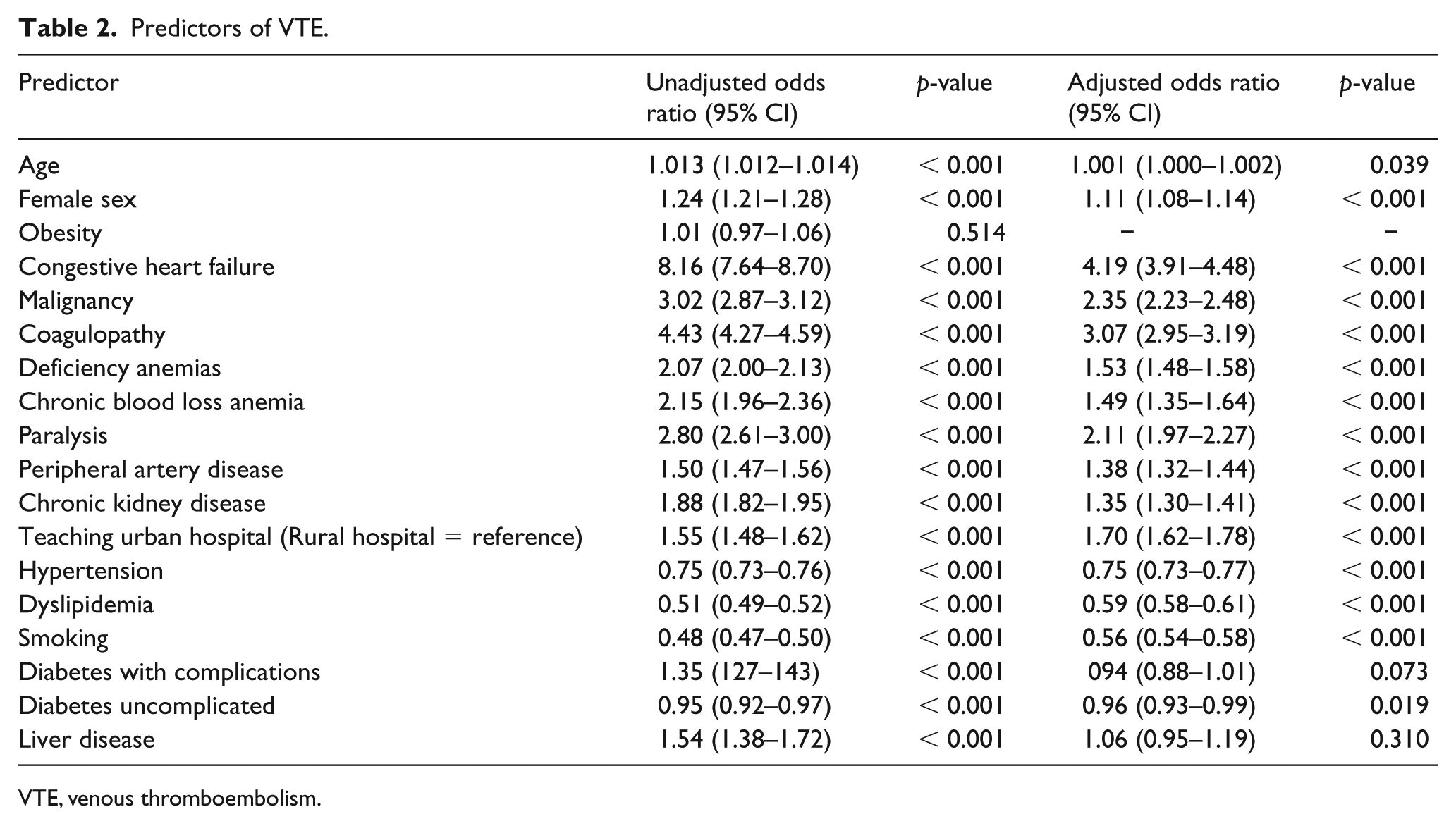
VTE, venous thromboembolism.
In-hospital mortality
Overall in-hospital mortality in patients who developed VTE after STEMI was 17.3%, which was significantly higher compared to those without VTE (8.9%) (unadjusted OR: 2.14, 95% CI: 2.07–2.21, p < 0.001; adjusted OR: 1.39, 95% CI: 1.34–1.44, p < 0.001). There was no statistically significant trend in rates of in-hospital mortality among patients with VTE (21.4% in 2003 to 16.8% in 2013, p = 0.072) (Figure 2).
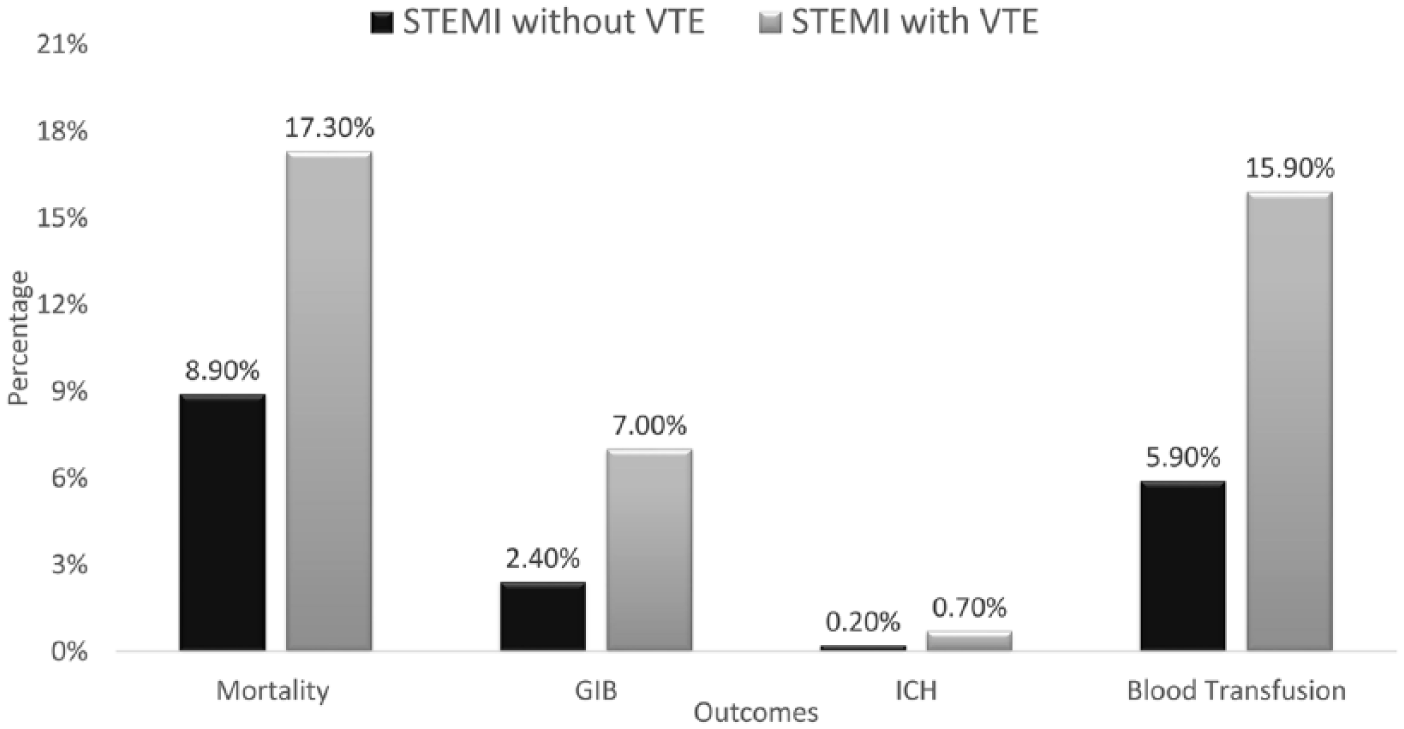
Comparison of mortality and bleeding rates between patients with STEMI with and without VTE.
Bleeding
Bleeding events were more common among patients with VTE. Compared to patients without VTE, those with VTE had significantly higher rates of gastrointestinal bleeding (2.4% vs 7%, adjusted OR: 2.13, 95% CI: 2.02–2.25, p < 0.001), intracranial bleeding (0.2% vs 0.7%, adjusted OR: 2.14, 95% CI: 1.84–2.49, p < 0.001), and need for blood transfusions (5.9% vs 15.9%, adjusted OR: 1.94, 95% CI: 1.87–2.02, p < 0.001) (Figure 2).
Cost and length of stay
STEMI patients with VTE had higher hospitalization costs compared to those without VTE (median [IQR] cost: $29,540 [44,698] vs $16,767 [15,368], p < 0.001). The cost of stay increased further in VTE patients who had a bleeding complication compared to those who did not experience bleeding (median [IQR] cost: $49,503 [58,621] vs $26,148 (38,209), p < 0.001). Similarly, VTE in the same population was associated with a longer hospital stay (median [IQR] length of stay: 9 [12] days vs 3 [3] days, p < 0.001).
Discussion
To date, very limited data exist on rates of VTE in patients admitted with STEMI. 3 In our analysis of a large nationwide cohort of STEMI patients in the United States, we demonstrated that VTE is not an uncommon complication. Notably, occurrence of VTE was associated with higher rates of mortality and bleeding complications. Additionally, higher cost and longer hospitalizations were observed among patients with VTE. In our study, patients with congestive heart failure, coagulopathy, malignancy, and paralysis had the highest likelihood of VTE occurrence.
The association between myocardial infarction and VTE has been explained by shared risk factors, transient systemic inflammation, and hypercoagulability following myocardial injury, and immobilization seen after complicated myocardial infarction.17–19 The percentage of VTE occurrence among our STEMI population was 1%, a rate that is almost comparable to in-hospital VTE rates of high-risk populations, such as cancer and surgical patients, in which VTE rates range from 1% to 4%.20–24 Similar to prior results from high-VTE-risk populations,21,22,25 we found a small but statistically significant uptrend in annual rates of VTE throughout the study period, which could potentially be explained by more aggressive diagnostic protocols, wider availability of biomarkers, and easier access to high-resolution multidetector computed tomography (CT) scanners. 26 Furthermore, our results showed that elderly patients (p < 0.001), black patients (p < 0.001), and females (p < 0.001) were more likely to develop VTE. These results are in agreement with current literature.27–31 There is a sizeable body of evidence linking heart failure, coagulopathy, malignancy, and paralysis30,32–36 with VTE occurrence, and indeed these factors were among the independent predictors of VTE in our analysis.
The management of VTE in the setting of acute myocardial infarction is challenging. Dual antiplatelet therapy (DAPT) is part of the standard of care treatment in patients presenting with STEMI. 37 VTE occurrence after MI is an indication for triple anticoagulation therapy (two antiplatelet agents plus therapeutic anticoagulation). Not surprisingly, the use of triple therapy following an acute coronary syndrome has been associated with increased risk of bleeding in several studies.38–40 Likewise, in our cohort of patients with STEMI, bleeding was more commonly observed in patients who experienced a VTE episode. In fact, patients with STEMI and VTE had higher rates of GI bleed (7% vs 2.4%), blood transfusion (15.9% vs 5.9%), and intracranial hemorrhage (0.7% vs 0.2%). These findings raise a question of whether a subset of these patients with an elevated bleeding risk may benefit from a lower intensity of anticoagulation or an agent with safer bleeding profile. Two recent trials showed that in atrial fibrillation patients undergoing PCI, a novel oral anticoagulant plus a P2Y12 inhibitor was associated with a lower risk of clinically significant bleeding compared to standard triple therapy (DAPT plus warfarin).39,41 Despite a lower risk of bleeding, the efficacy of dual therapy compared to triple therapy in patients receiving PCI remains unclear, particularly with STEMI patients as they have a high incidence of stent thrombosis.42,43 Thus, treatment of these patients represents a dilemma where the use of careful clinical judgment by weighing the risk of stent thrombosis against the hazards of bleeding is considered essential, and where further trials are necessary to draw evidence-based conclusions.
The occurrence of VTE carries significant prognostic implications in surgical and oncology patients.44–48 However, the clinical significance in patients with STEMI has not yet been elucidated. In our cohort of patients, those who developed VTE were more likely to die when compared to patients without VTE (17.3% vs 8.9%), even after adjusting for potential confounders. The unfavorable effect of VTE on mortality can be at least partly attributed to fatal VTEs in the form of pulmonary embolism. In addition, VTE might be a reflection of a more extensive myocardial injury, sicker patients, more immobilization, and pre-existing comorbidities.
In addition to the elevated bleeding complications and mortality, in our analysis, VTE management was associated with higher hospitalization costs, and length of stay. Similar findings were described in different cohorts of VTE patients. 49
Strengths and limitations
The main strength of our study is the scrutiny of a large pool of patients obtained from the NIS, one of the largest medical data sources in the US, that not only allowed us to obtain significant information and understand the relationship between VTE and STEMI, but also provided a real-world scenario making the results generalizable. Despite its strengths, our study is not free from limitations, including those inherent to any retrospective analysis. First, there are limited data on the validity of the ICD-9 codes used to ascertain STEMI. In addition, administrative databases are prone to erroneous diagnosis entering or misclassification that can result in under- or overestimation of diseases. Moreover, there is the possibility of inaccurate differentiation of comorbidities from complications. However, we tried to use all available and validated ICD codes to identify the variables relevant to our study. The database does not contain biochemical data, information on medication utilization, echocardiographic and angiographic reports, and cause of death, which prevented us from exploring their association with our outcomes. Lastly, data on long-term outcomes were lacking.
Conclusion
VTE occurrence among patients with STEMI was not only associated with higher mortality rates, but also increased bleeding risk, creating a therapeutic dilemma for treating physicians. Furthermore, VTE management was costly and associated with higher utilization of healthcare resources. This suggests that accurate identification of patients at high risk of VTE coupled with targeted administration of thromboprophylaxis to patients not on therapeutic anticoagulation should be more strictly applied to patients with STEMI to minimize the drastic consequences of VTE in this population. There is a paucity of literature on this topic and, after confirmation of our findings, future research should focus on the prevention and management of VTE in patients with STEMI.
Supplemental Material
Supplementary_Data – Supplemental material for Rate and impact of venous thromboembolism in patients with ST-segment elevation myocardial infarction: Analysis of the Nationwide Inpatient Sample database 2003–2013
Supplemental material, Supplementary_Data for Rate and impact of venous thromboembolism in patients with ST-segment elevation myocardial infarction: Analysis of the Nationwide Inpatient Sample database 2003–2013 by Ahmed Al-Ogaili, Ali Ayoub, Luis Diaz Quintero, Christian Torres, Harry E Fuentes, Setri Fugar, Ahmed A Kolkailah, Wael Dakkak, Alfonso J Tafur and Neha Yadav in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.