
Abstract
In people without lower extremity peripheral artery disease (PAD), mitochondrial DNA copy number declines with aging, and this decline is associated with declines in mitochondrial activity and functional performance. However, whether lower extremity ischemia is associated with lower mitochondrial DNA copy number and whether mitochondrial DNA copy number is associated with the degree of functional impairment in people with PAD is unknown. In people with and without PAD, age 65 years and older, we studied associations of the ankle–brachial index (ABI) with mitochondrial DNA copy number and associations of mitochondrial DNA copy number with functional impairment. Calf muscle biopsies were obtained from 34 participants with PAD (mean age: 73.5 years (SD 6.4), mean ABI: 0.67 (SD 0.15), mean 6-minute walk distance: 1191 feet (SD 223)) and 10 controls without PAD (mean age: 73.1 years (SD 4.7), mean ABI: 1.14 (SD 0.07), mean 6-minute walk distance: 1387 feet (SD 488)). Adjusting for age and sex, lower ABI values were associated with higher mitochondrial DNA copy number, measured in relative copy number (ABI<0.60: 914, ABI 0.60–0.90: 731, ABI 0.90–1.50: 593; p trend=0.016). The association of mitochondrial DNA copy number with the 6-minute walk distance and 4-meter walking velocity differed significantly between participants with versus without PAD (p-value for interaction=0.001 and p=0.015, respectively). The correlation coefficient between mitochondrial DNA copy number and the 6-minute walk distance was 0.653 (p=0.056) among people without PAD and –0.254 (p=0.154) among people with PAD and ABI < 0.90. In conclusion, lower ABI values are associated with increased mitochondrial DNA copy number. Associations of mitochondrial DNA copy number with the 6-minute walk distance and 4-meter walking velocity significantly differed between people with versus without PAD, with stronger positive associations observed in people without PAD than in people with PAD. The cross-sectional and exploratory nature of the analyses precludes conclusions regarding causal inferences.
Introduction
Growing evidence suggests that lower extremity peripheral artery disease (PAD) is associated with calf skeletal muscle abnormalities, and these calf muscle abnormalities are associated with functional impairment and decline in PAD.1–7 The association of PAD with calf muscle mitochondrial activity is conflicting, with some studies reporting increased activity and others reporting lower activity of mitochondrial markers in people with PAD compared to those without PAD.5–13 Further information about the association of lower extremity ischemia with measures of mitochondrial function is needed.
In healthy men without PAD, mitochondrial DNA copy number correlates positively with mitochondrial volume and abundance of mitochondrial enzyme mRNA in response to exercise training. 14 In people without PAD, older age is associated with a lower abundance of mitochondrial DNA copy number and poorer activity of mitochondrial enzymes.15–17 Among older people, lower mitochondrial DNA copy number is associated with poorer health and poorer lower extremity functioning.15–17 If lower extremity ischemia accelerates the decline in mitochondrial DNA copy number that occurs with aging, people with PAD may have a lower abundance of mitochondrial DNA copy number and lower oxidative capacity than people without PAD. Alternatively, lower extremity ischemia could increase mitochondrial DNA copy number, if ischemia damages mitochondria and promotes a compensatory mitochondrial biogenesis or if ischemia impairs mitophagy and prevents removal of defective mitochondria.18,19 If lower extremity is-chemia damages mitochondrial DNA and also impairs mitophagy,20–23 mitochondrial DNA copy number could increase without improving mitochondrial activity.
This study delineated the association of lower extremity ischemia with abundance of mitochondrial DNA and the association of mitochondrial DNA copy number with mitochondrial activity and other meaningful outcomes in the setting of PAD. This study had the following aims. First, to assess the association of lower extremity ischemia severity, measured by the ankle–brachial index (ABI), with calf muscle mitochondrial DNA copy number in people with and without PAD. Second, to study the association of calf muscle mitochondrial DNA copy number with walking performance, measured by the 6-minute walk and 4-meter walking velocity, in people with PAD. Third, to determine whether associations of mitochondrial DNA copy number with 6-minute walk distance and 4-meter walking velocity differ in people with versus without PAD. Fourth, to determine whether greater mitochondrial DNA copy number is associated with an increased abundance of peroxisome proliferative activated receptor-γ co-activator 1α (PGC-1α), a marker of mitochondrial biogenesis, in people with PAD. Fifth, in people with PAD, to study the association of mitochondrial measures with brachial artery flow-mediated dilation (FMD). For this fifth aim, we hypothesized that poorer mitochondrial health and oxidative capacity would be associated with poorer brachial artery FMD. We proposed this hypothesis because poorer mitochondrial health and oxidative capacity are associated with increased oxidative stress and reduced nitric oxide availability, which is associated with poorer FMD. 2
Methods
PAD participants in this study were in the RESTORE trial, a pilot randomized trial of resveratrol in people with PAD, age 65 years and older. 22 Participants without PAD were identified for comparison. Analyses reported here are exploratory and represent cross-sectional data obtained from PAD participants in the RESTORE trial at baseline, prior to randomization, and participants without PAD identified from among those evaluated for eligibility in RESTORE and other randomized trials of PAD participants or observational studies of participants with and without PAD.22–25 The Institutional Review Board of Northwestern University approved the protocol. Participants provided written informed consent.
Recruitment
Participants with PAD were identified through postcards mailed to community dwelling older men and women living in the Chicago area. People with PAD who had previously participated in PAD-related research at Northwestern University and expressed interest in future research participation were contacted. Non-PAD participants were identified from among potential participants for RESTORE and other studies of participants with and without PAD22–25 who were found to have a normal ABI at their baseline visit and provided informed consent for muscle biopsy. Participants without PAD underwent the 6-minute walk test and measures of usual and fast paced 4-meter walking velocity, but did not have treadmill testing, measurement of brachial artery FMD, or mitochondrial measures other than mitochondrial DNA copy number.
Inclusion and exclusion criteria
Age ≥65 years was an inclusion criterion. PAD was defined as an ABI < 0.90 in either leg. 22 Individuals with PAD who had a resting ABI ≥ 0.90 were potentially eligible if their medical record documented lower extremity revascularization or evidence of PAD from a non-invasive vascular laboratory test performed at a medical center. Participants without PAD had an ABI between 0.90 and 1.40 at their baseline study visit.
Exclusion criteria have been reported 22 and are summarized briefly. For those with PAD, potential participants with a below-knee or above-knee amputation and those whose walking was primarily limited by a reason other than PAD were excluded. Participants with PAD and planned lower extremity revascularization in the next 6 months were excluded. For all participants, wheelchair confinement, use of a walking aid, and significant visual or hearing impairment were exclusion criteria. Potential participants on dialysis, those with lung disease requiring oxygen, and those with a myocardial infarction, stroke, lower extremity revascularization, or other major surgery in the past 3 months were excluded. Potential participants who were treated for cancer in the past 2 years were excluded unless their prognosis was excellent. Potential participants participating in another clinical trial were excluded. Potential participants with a Mini-Mental Status Examination score < 23 at baseline were excluded. 22
ABI measurement
A hand-held Doppler probe (Pocket Dop II; Nicolet Biomedical Inc., Golden, CO, USA) was used to obtain systolic pressures twice in the right and left brachial, dorsalis pedis, and posterior tibial arteries using established methods.22–26 The ABI was calculated by dividing the mean of the dorsalis pedis and posterior tibial pressures in each leg by the mean of the four brachial pressures. 26 Mean pressures in the arm with the higher pressure were used when one brachial pressure was higher than the opposite brachial pressure in both measurement sets and the two brachial pressures differed by ≥ 10 mmHg in one measurement set.22–26
Medical history
Medical history, race, and demographics were obtained through patient report by a trained and certified health interviewer using a questionnaire.
Six-minute walk test
Following a standardized protocol,22,23,27–29 participants walked up and down a 100-foot hallway for 6 minutes after instructions to cover as much distance as possible. The distance completed after 6 minutes was recorded.
Treadmill walking performance
Treadmill walking performance was measured among participants with PAD using the Gardner–Skinner protocol.22,23,30,31
Brachial artery flow-mediated dilation
Among participants with PAD, brachial artery FMD was measured after a 12-hour fast by trained Registered Diagnostic Cardiac Sonographers, at baseline and 6-month follow-up, using standard procedures.22,23,31 The proximal brachial artery was imaged (B-mode and Doppler) using a linear array vascular ultrasound transducer (frequency 8 MHz, range 5–8 MHz) (Sequoia Model #256; Siemens Medical Solutions, Erlangen, Germany).
Four-meter walking velocity
Walking velocity was measured with a 4-meter walk performed at ‘usual’ and ‘fastest’ pace. For the ‘usual’ pace walk, participants were instructed to walk at their usual pace, ‘as if going down the street to the store’. Each walk was performed twice. The faster walk in each pair was used in analyses.27,28
Calf skeletal muscle biopsy procedure
An open muscle biopsy was performed in the medial head of the gastrocnemius muscle of the leg with the lower ABI in participants with and without PAD. Anesthesia was achieved with subcutaneous lidocaine. Subcutaneous and adipose tissue were dissected until muscle was identified. Muscle tissue was removed and immediately prepared for freezing at −70°C.
Mitochondrial DNA copy number and measures of mitochondrial activity
Total DNA was isolated from human muscle using the Wizard Genomic DNA Purification Kit according to the manufacturer’s instructions (Promega, Madison, WI, USA). After purification, DNA was evaluated spectrophotometrically by NanoDrop 1000 (Thermo Scientific, Rockford, IL, USA). Quantification of the relative number of copies of mitochondrial DNA copy number (using nuclear DNA as a standard) was determined with the Human Mitochondrial DNA Monitoring Primer Kit (#7246; Takara Bio USA, Mountain View, CA, USA) using real-time polymerase chain reaction (RT-PCR). RT-PCR amplification reactions were performed on a CFX96 Touch™ Real-Time PCR Detection System (Bio-Rad Laboratories Inc., Hercules, CA, USA). Primers were used to amplify genes corresponding to mitochondrial NADH dehydrogenase subunits 1 and 5 (ND1, ND5) and the nuclear genes corresponding to solute carrier organic anion transporter family member 2b1 (SLCO2B1) and serpin family A member 1 (SERPINA1). 32 The reaction mixture consisted of 12.5 µL Terra qPCR Direct SYBR Premix (2X), 0.4 µM forward and reverse primers, and genomic DNA template (10 ng). Each sample was analyzed in triplicate. The quantification of the relative mitochondrial DNA content was performed according to the Pfaffl mathematical model. 33 The difference in threshold cycle values for the ND1/SLCO2B1 pair (ΔCt1 = Ct for SLCO2B1 − Ct for ND1) and the ND5/SERPINA1 pair (ΔCt2 = Ct for SERPINA1 − Ct for ND5) were calculated and the average of 2ΔCt1 and 2ΔCt2 was used as the measure of mitochondrial DNA copy number expressed as arbitrary units.
COX and citrate synthase were measured to assess mitochondrial enzyme activity. PGC-1α was measured because it is a major regulator of mitochondrial biogenesis. COX (nmol/min/mg total protein) and citrate synthase (µmol/min/g total protein) activities were measured in duplicate spectrophotometrically in whole muscle homogenates 33 and normalized to a standard cross sample included within each batch. For immunoblotting of PGC-1α, whole muscle tissue homogenates were prepared as described previously.22,34 Proteins were separated on 20% polyacrylamide gels, transferred to PVDF membranes and blocked for 1 hour in 5% milk in Tris-buffered saline Tween. Blots were probed with the appropriate primary antibodies (1:500; Millipore #516557, PGC-1α) and anti-rabbit secondary antibody conjugated with horseradish peroxidase (1:5000; #7074; Cell Signaling Technology, (Danvers, MA)). Proteins were visualized with SuperSignal West Femto Maximum Sensitivity Substrate (Thermo Scientific) using a ChemiDoc XRS imager from Bio-Rad. Bands were quantified using Image Lab Software from Bio-Rad and normalized to a standard cross sample included within each gel and to Ponceau stain for loading control.
Other measures
Height and weight were measured at baseline. Body mass index (BMI) was calculated as weight (kg)/[height (meters)] 2 .
Statistical analyses
Baseline characteristics of participants with versus without PAD were summarized as means and standard deviations for continuous variables and as frequencies and percentages for categorical variables. T-tests were used to compare continuous characteristics and chi-squared tests and Fisher’s exact test were used to compare categorical characteristics of participants with versus without PAD, when appropriate. Linear regression analyses were used to test for trend across mitochondrial DNA copy number tertiles, including an independent variable with values of ‘1, 2, and 3’ to represent 1st, 2nd, 3rd tertiles, respectively. Pearson correlation coefficients were used to measure and compare the association of the ABI with mitochondrial DNA copy number among participants with and without PAD and separately in PAD participants. Pearson correlation coefficients were used to relate mitochondrial DNA copy number to 6-minute walk performance, COX enzyme activity, citrate synthase activity, PGC-1α, and brachial artery FMD. Based on scatterplot data, in which associations appeared to vary by severity of lower extremity ischemia, analyses were repeated according to PAD severity. For the 6-minute walk, analyses were repeated among participants with normal ABI, participants with an ABI of 0.60–0.90, and participants with an ABI < 0.60, respectively. Associations of mitochondrial DNA copy number with remaining mitochondrial measures and the brachial artery FMD were estimated separately among participants with an ABI of 0.60–0.90 and among participants with an ABI < 0.60. The interaction terms for the indicator ‘PAD’ in the association between mitochondrial DNA copy number and functional measures were tested using regression models. One PAD participant with an ABI > 0.90 was excluded from analyses of interaction testing. Analyses were exploratory and were not adjusted for multiple comparisons. Analyses were performed using SAS version 9.4 (Cary, NC, USA).
Results
Of 66 participants in the RESTORE trial, 23 refused muscle biopsy, three did not receive permission from their physician to stop antiplatelet or anticoagulation therapy for muscle biopsy, one withdrew from the study, and the remaining 39 had a muscle biopsy. Of the 39, two did not yield sufficient muscle for analyses, and three did not have sufficient muscle tissue after analysis for the RESTORE trial to analyze mitochondrial DNA copy number. One participant with PAD had a history of revascularization and an ABI > 0.90. Ten participants without PAD, age 65 years and older, had muscle available for mitochondrial DNA analyses. Characteristics of participants are in Table 1. Participants with PAD included a higher proportion of men than those without PAD. Lower ABI values and higher COX enzyme activity were associated with significantly higher mitochondrial DNA copy number among participants with PAD (Table 2).
Characteristics of participants with versus without PAD.
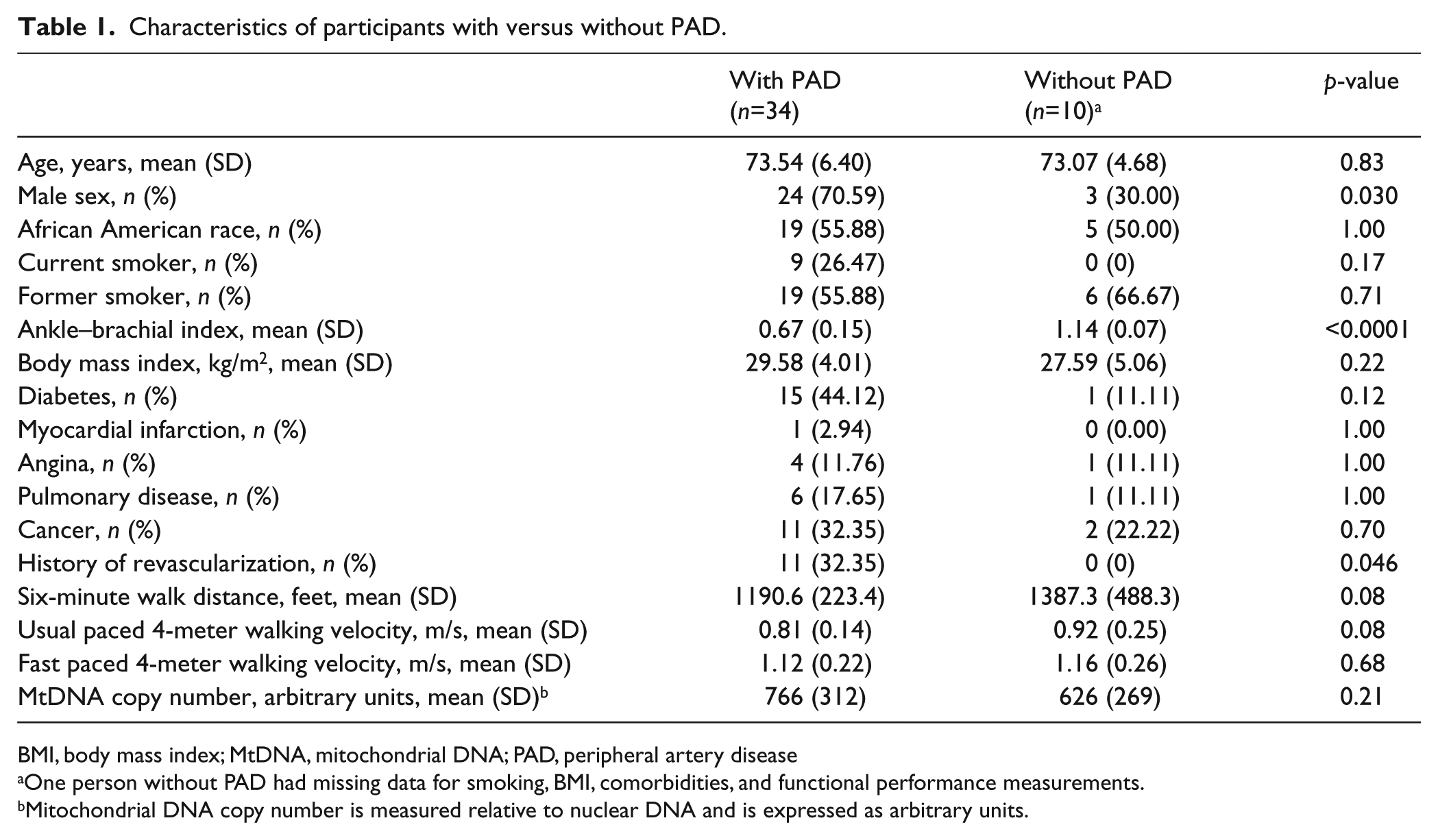
BMI, body mass index; MtDNA, mitochondrial DNA; PAD, peripheral artery disease
One person without PAD had missing data for smoking, BMI, comorbidities, and functional performance measurements.
Mitochondrial DNA copy number is measured relative to nuclear DNA and is expressed as arbitrary units.
Characteristics associated with higher mitochondrial DNA copy number among people with PAD (n=34). a
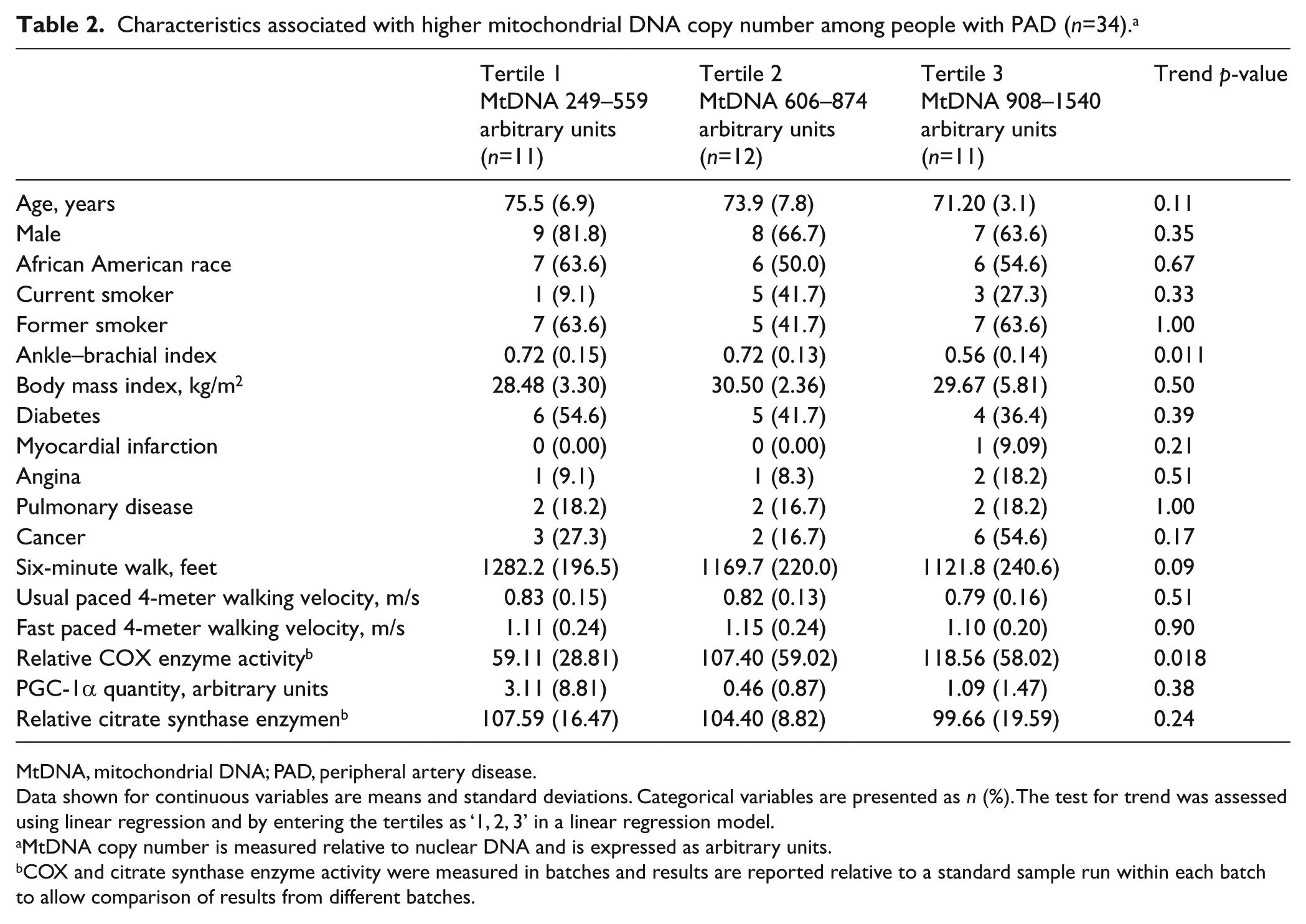
MtDNA, mitochondrial DNA; PAD, peripheral artery disease.
Data shown for continuous variables are means and standard deviations. Categorical variables are presented as n (%). The test for trend was assessed using linear regression and by entering the tertiles as ‘1, 2, 3’ in a linear regression model.
MtDNA copy number is measured relative to nuclear DNA and is expressed as arbitrary units.
COX and citrate synthase enzyme activity were measured in batches and results are reported relative to a standard sample run within each batch to allow comparison of results from different batches.
The ABI was associated positively with distance achieved in the 6-minute walk test among participants with PAD (Pearson correlation coefficient = 0.417, p=0.014), but there was no association of ABI with the 6-minute walk distance among participants without PAD (Figure 1).
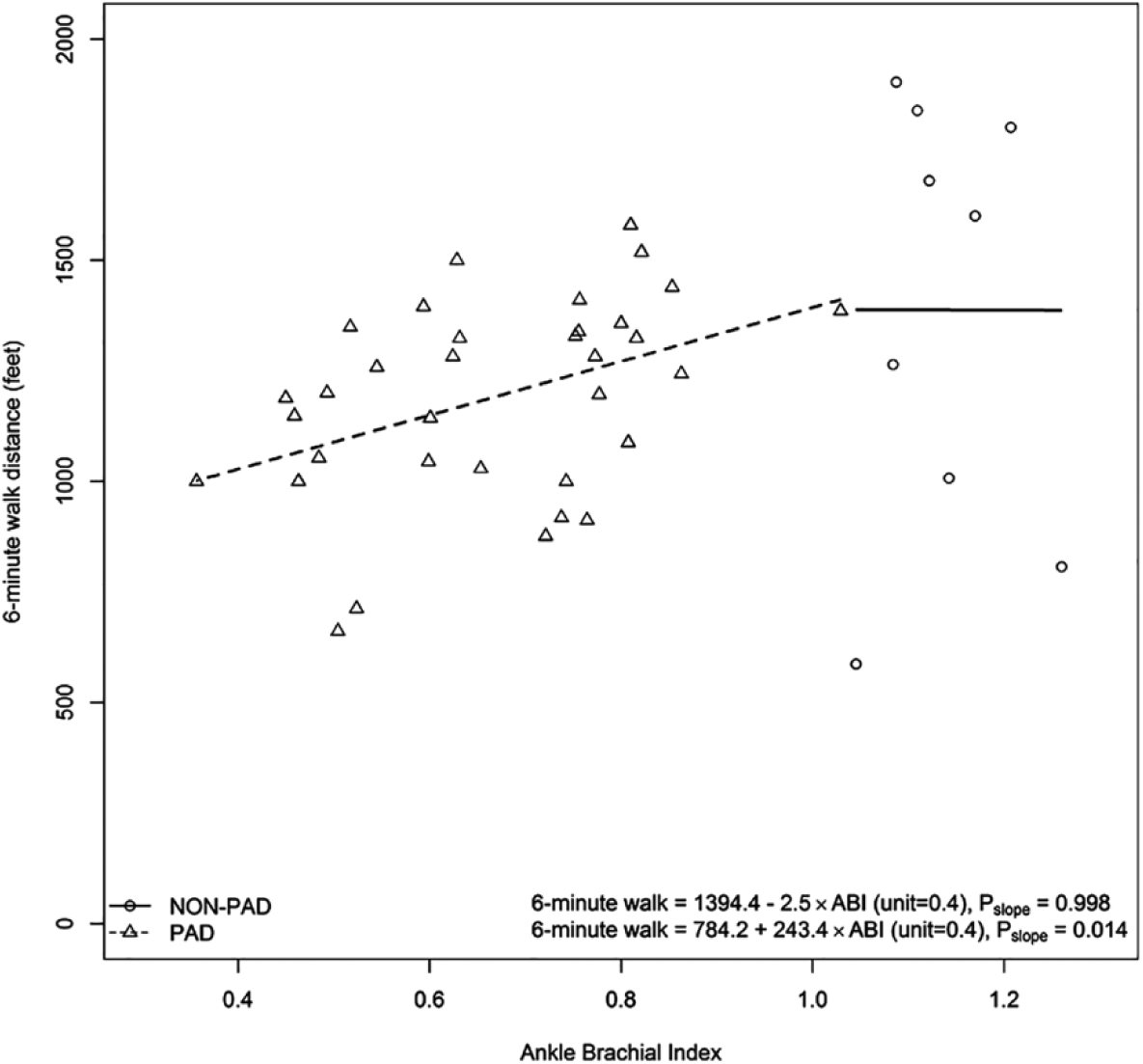
Associations of the ABI with 6-minute walk performance among participants with and without PAD.a
There was no significant difference in mitochondrial DNA copy number between participants with versus without PAD (Table 1). Overall, the association of ABI with mitochondrial DNA copy number was Pearson correlation coefficient = −0.350, p=0.020. Among participants with PAD, lower ABI values were associated with higher mitochondrial DNA copy number (Pearson correlation coefficient = −0.355, p=0.040) (Figure 2). Among participants without PAD, the Pearson correlation coefficient for the association of ABI with mitochondrial DNA copy number was –0.299 (p=0.402) (Figure 2).
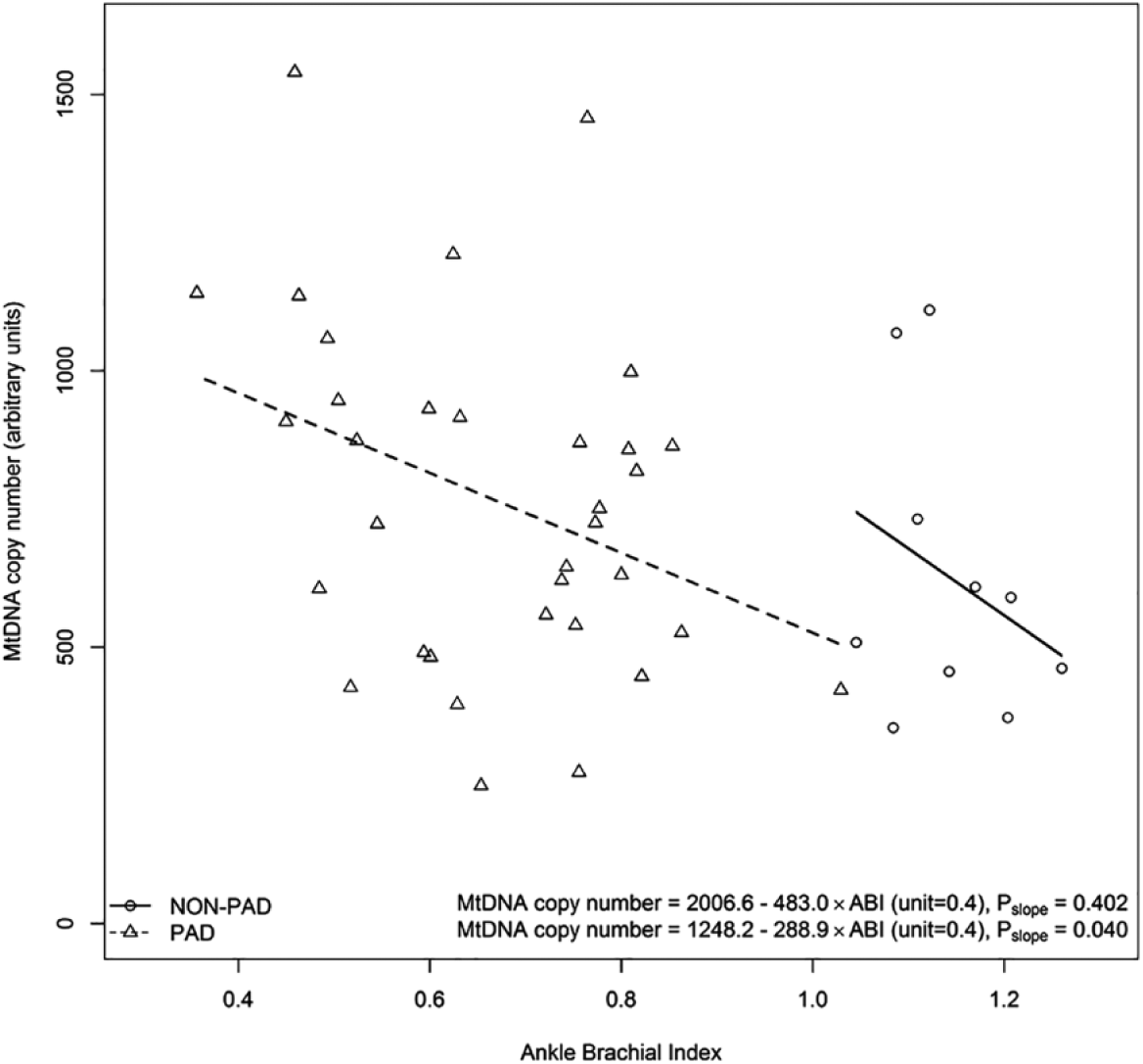
The ABI and MtDNA copy number in participants with and without PAD.a
There was a statistically significant interaction of presence versus absence of PAD and the association of mitochondrial DNA copy number with the 6-minute walk (p for interaction = 0.001). This meant that the association of mitochondrial DNA copy number with the 6-minute walk distance was significantly different between participants with versus without PAD and this difference was not likely due to chance. The correlation coefficient between mitochondrial DNA copy number and the 6-minute walk distance was 0.653 (p=0.056 ) among people without PAD and –0.254 (p=0.154) among people with PAD and ABI < 0.90 (Figure 3).
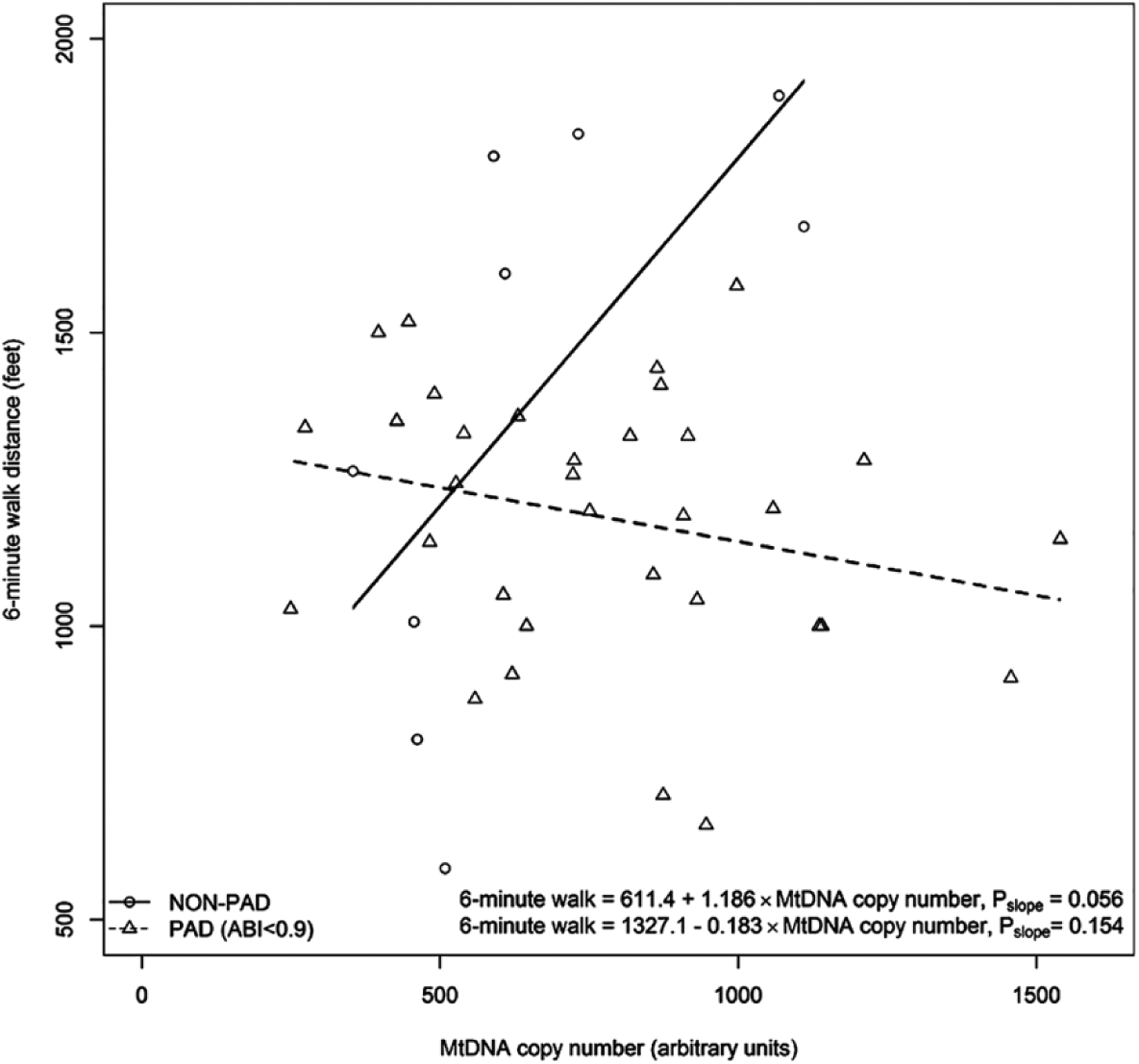
Association of MtDNA copy number and 6-minute walk distance for PAD and non-PAD participants.a
There was a statistically significant interaction of presence versus absence of PAD and the association of mitochondrial DNA copy number with the usual paced 4-meter walking velocity (p for interaction = 0.015) (Table 3). This meant that the association of mitochondrial DNA copy number with the 4-meter walking velocity test was significantly different between participants with versus without PAD and this difference was not likely due to chance. The correlation coefficient between mitochondrial DNA copy number and usual paced 4-meter walking velocity was 0.579 (p=0.102) among people without PAD and –0.09 (p=0.601) among people with PAD.
Correlations coefficients of MtDNA copy number with functional performance measures, according to ABI value.
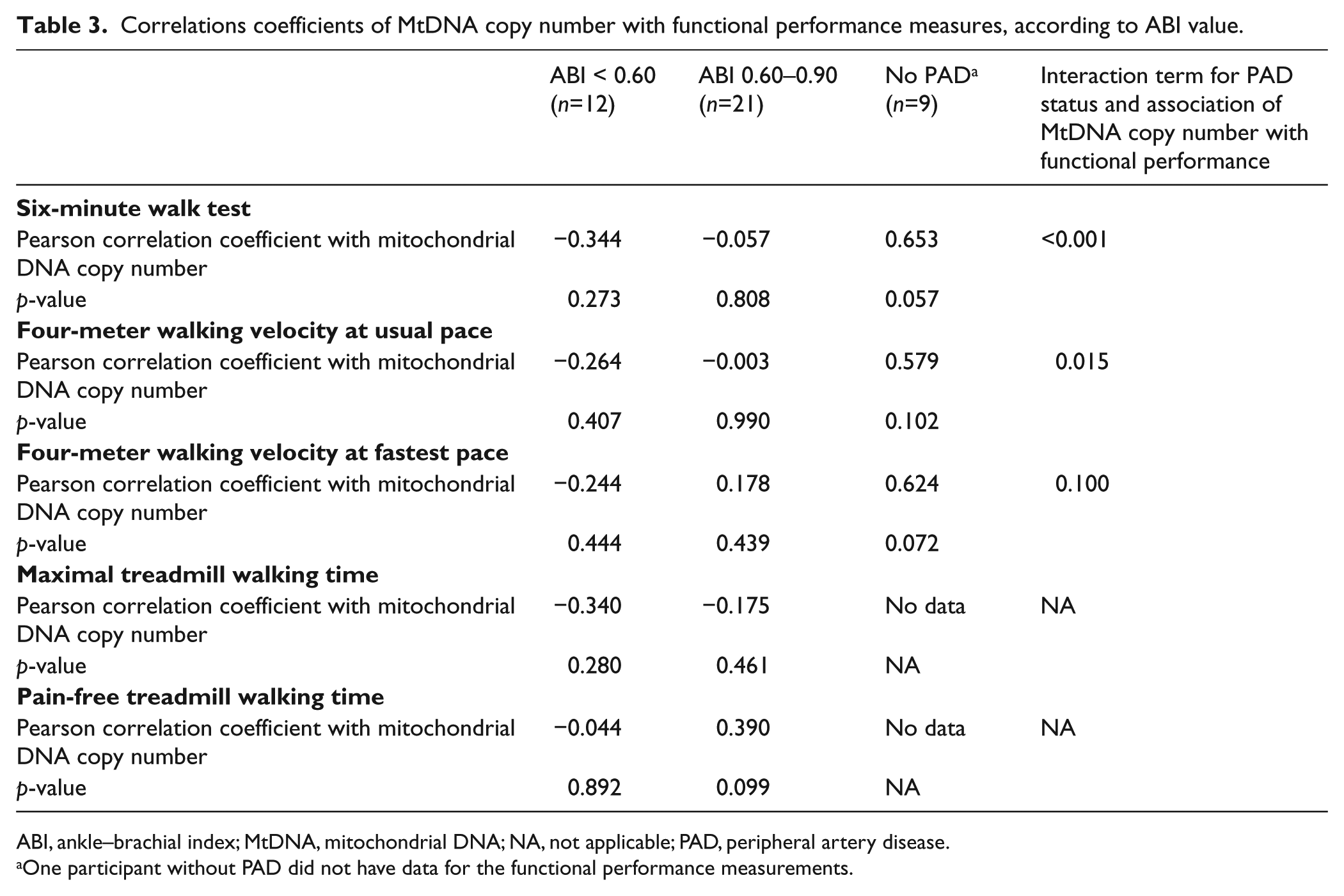
ABI, ankle–brachial index; MtDNA, mitochondrial DNA; NA, not applicable; PAD, peripheral artery disease.
One participant without PAD did not have data for the functional performance measurements.
Among all participants with PAD, a statistically significant association of mitochondrial DNA copy number with COX enzyme activity was observed (Pearson correlation coefficient = 0.385, p=0.033). People with the most severe ischemia had no significant associations of mitochondrial DNA copy number with any mitochondrial measures or brachial artery FMD. However, among participants with mild to moderate PAD (ABI 0.60–0.90), higher mitochondrial DNA copy number was associated with greater citrate synthase activity and with greater relative brachial artery FMD, a measure of vascular function (Table 4).
Correlations of MtDNA copy number with markers of mitochondrial activity and mitochondrial biogenesis among participants with PAD. a
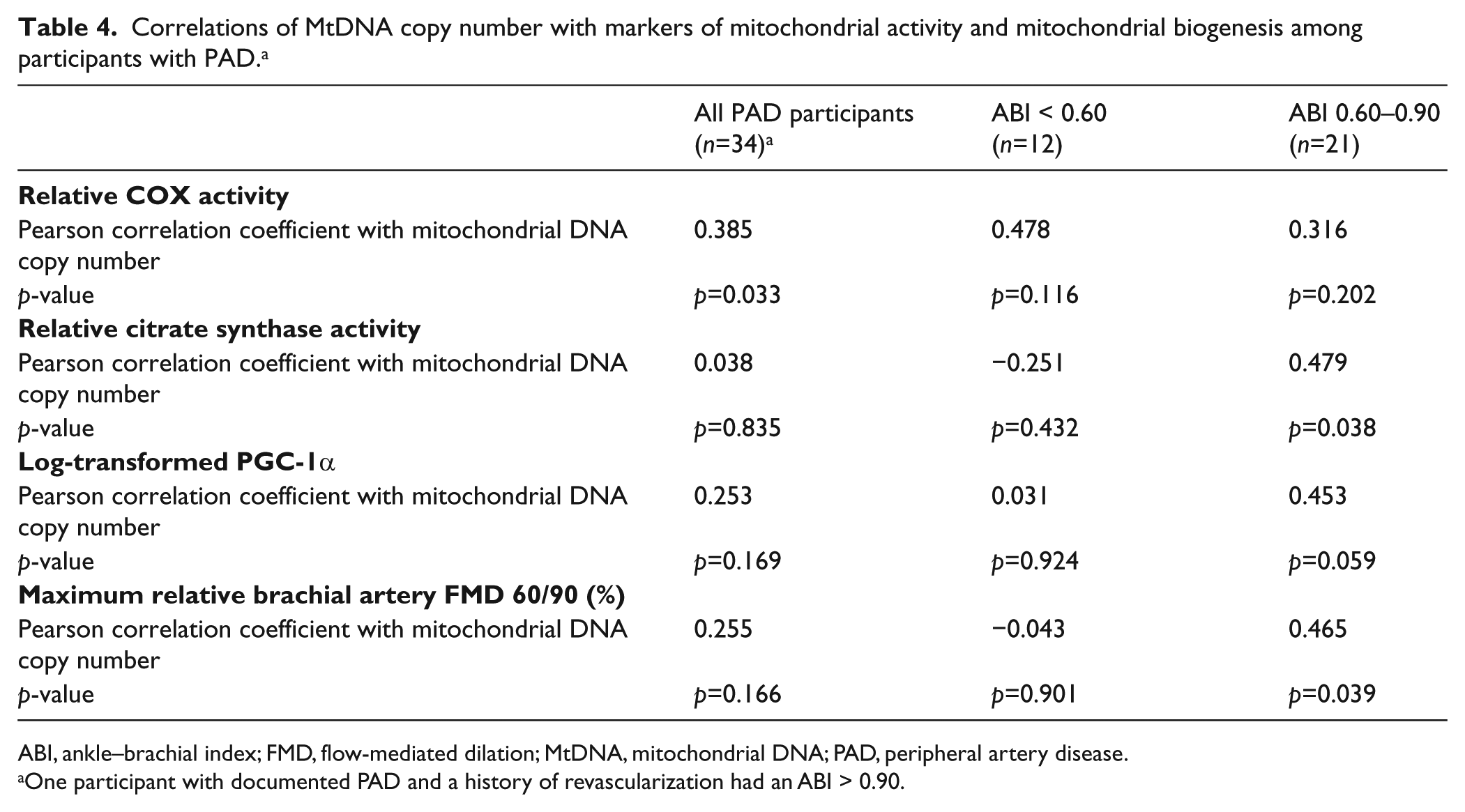
ABI, ankle–brachial index; FMD, flow-mediated dilation; MtDNA, mitochondrial DNA; PAD, peripheral artery disease.
One participant with documented PAD and a history of revascularization had an ABI > 0.90.
Discussion
Results reported here showed that more severe lower extremity ischemia, measured by the ABI, was associated with significantly higher mitochondrial DNA copy number. Results also showed a statistically significant interaction for the association of mitochondrial DNA copy number with the 6-minute walk distance and 4-meter walking velocity. Specifically, results showed that the magnitude of association of mitochondrial DNA copy number with functional performance measures was statistically significantly more positive in participants without PAD, compared to those with PAD. To our knowledge, this is the first study of mitochondrial DNA copy number to include participants with and without classical symptoms of intermittent claudication in a cohort of PAD participants without critical limb ischemia.
A prior study reported no difference in mitochondrial DNA copy number between people with versus without PAD, 35 consistent with results reported here. However, to our knowledge, no prior studies have reported on the association of greater lower extremity ischemia with mitochondrial DNA copy number. Our finding that more severe lower extremity ischemia was associated with higher mitochondrial DNA copy number may be due to a compensatory increase in mitochondrial DNA copy number in the setting of ischemia-related reductions in mitochondrial activity. Our finding that mitochondrial DNA copy number was not significantly associated with any mitochondrial or functional measures or with brachial artery FMD in people with severe lower extremity ischemia suggests that a compensatory increase in mitochondrial DNA copy number was inadequate in people with severe lower extremity or that mitochondria in people with severe lower extremity ischemia are damaged. Consistent with this possibility, results reported here showed that PAD participants with mild to moderate PAD had statistically significant and positive correlations of mitochondrial DNA copy number with calf muscle citrate synthase activity and brachial artery FMD, but positive associations were not observed among PAD participants with severe PAD.
Prior research has been contradictory regarding the association of PAD with mitochondrial measures.5–13 PAD patients who successfully compensate may have higher measures of both mitochondrial activity and abundance, while those with severe ischemia may be unable to fully compensate, resulting in lower mitochondrial activity despite greater mitochondrial abundance. Increased mitochondrial damage, mitochondrial DNA deletions, and impaired mitophagy have been reported in the calf muscle of people with PAD.18–21 These phenomena may also potentially explain higher mitochondrial DNA copy number in people with more severe ischemia. For example, damaged mitochondrial DNA may accumulate in the setting of impaired mitophagy. 21
To our knowledge, no prior studies have related mitochondrial DNA copy number to the 6-minute walk performance or 4-meter walking velocity in people with PAD. Our finding of a statistically significant interaction term for the presence versus absence of PAD and the association of mitochondrial measures with the 6-minute walk and 4-meter walking velocity is consistent with, but distinct from, a previous study demonstrating that calf muscle mitochondrial DNA copy number correlated with aerobic exercise capacity, measured by VO2 max, in people without PAD but not in people with PAD. 35
Impaired mitochondrial activity is associated with increased oxidative stress and lower nitric oxide availability. 2 For this reason, it is conceivable that impaired mitochondrial activity may be correlated with impaired brachial artery FMD, a measure of vascular function. Our finding that mitochondrial DNA copy number was correlated with brachial artery FMD in people with an ABI of 0.60–0.90 is consistent with this hypothesis. To our knowledge, this association has not been reported previously.
Limitations
This study has limitations. First, the study was cross-sectional. The biologic pathways responsible for the associations described here cannot be determined. Second, the sample size was small, limiting statistical power, particularly in the group of participants with an ABI < 0.60. Third, the analyses were performed as exploratory analyses in a trial of resveratrol for people with PAD 21 and the results were not adjusted for multiple testing due to the sample size limitations. Results require confirmation. Fourth, mitochondrial DNA copy number has not been associated consistently with mitochondrial volume or abundance in young healthy males. 36 Furthermore, in people with chronic disease, a compensatory increase in mitochondrial DNA copy number may occur that is not associated with improved mitochondrial activity. 37 Therefore, the significance of an increase in mitochondrial DNA copy number in people with PAD remains uncertain. Fifth, calf muscle biopsy measures of COX activity, citrate synthase activity, and PGC-1α and brachial artery FMD were not measured in participants without PAD. Sixth, data on respirometry or oxidative stress were not available. Seventh, it is possible that associations of lower extremity ischemia and mitochondrial DNA copy number may differ between PAD participants with versus without a history of lower extremity revascularization. Finally, results may have been influenced by the fact that the PAD participants had more males than the non-PAD participants.
Conclusion
In conclusion, more severe lower extremity ischemia is associated with an increased mitochondrial DNA copy number. Findings reported here are consistent with the hypothesis that greater mitochondria abundance in the calf muscle of people with lower extremity ischemia may reflect a compensatory response that is inadequate, particularly in the setting of severe lower extremity ischemia. A prospective study is needed to confirm these findings and delineate the biologic pathways responsible for the associations reported here.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institute on Aging (R21-AG047510), National Heart, Lung, and Blood Institute (R01-HL107510, R01HL109244, R01-HL088589, R01HL122846), and the Office of Dietary Supplements.