
Abstract
Patients with peripheral artery disease (PAD) and intermittent claudication (IC) have impaired functional status and quality of life. However, little is known about which factors are associated with poorer health status at the time of initial presentation for PAD specialty care. Characterization of such features might provide insight into disparities that impact health status in this population. A total of 1258 patients from the United States, the Netherlands and Australia with new or worsened IC were enrolled at their first PAD specialty care visit between June 2011 and December 2015. The mean Peripheral Artery Questionnaire (PAQ) Summary Score (range 0–100), a disease-specific health status measure, was 49.2 ± 21.9. Hierarchical, multivariable linear regression was used to relate patient characteristics to baseline PAQ. Patient characteristics independently associated with poorer health status were age (p < 0.001), female sex (p < 0.001), not being married (p = 0.02), economic burden (moderate/severe vs none, moderate/severe vs some; p = 0.03), difficulty getting care (moderate/severe vs none, moderate/severe vs some; p < 0.001), chronic lung disease (p = 0.02), back pain (p < 0.001), bilateral vs unilateral PAD (p = 0.02), intermittent claudication severity (moderate vs mild, severe vs mild, p < 0.001), and lack of prior participation in an exercise program (p = 0.005). Disparities in both vascular and non-vascular factors were associated with patients’ health status at the time of presentation and should be addressed by all who care for patients with vascular disease.
Introduction
Peripheral artery disease (PAD) significantly impairs the health status of affected individuals.1,2 PAD is present in 5.9% of subjects ≥40 years of age, resulting in an estimated prevalence of 7.2 million affected individuals in the United States 3 and >200 million people worldwide. 1 Because of impaired functional status,4,5 patients with PAD have a quality of life (QoL) 6 similar to those with chronic lung disease or heart failure. In part, because only 10% of patients with PAD have classic claudication (the majority of symptomatic patients report atypical leg pain), 7 PAD remains under-diagnosed 8 and undertreated. 3 Among patients referred for vascular specialty care, the patient characteristics associated with poorer health status have not been previously described. Disparities in sociodemographic, clinical, and treatment-related factors may all contribute to poorer health status, and their elucidation may help identify populations of patients presenting later in the course of their disease who could benefit from earlier access to PAD care. To address this gap in knowledge, we related patient characteristics to health status at the time of presentation for PAD specialty care among an international cohort of patients enrolled in the Patient-centered Outcomes Related to TReatment Practices in Peripheral Arterial Disease: Investigating Trajectories (PORTRAIT) registry. 9
Methods
Study population
PORTRAIT was a prospective, observational cohort study of adult patients with new or worsened intermittent claudication enrolled at the time of their first evaluation for PAD specialty care. After excluding those who had a history of amputation (n=16) or were missing their baseline Peripheral Artery Questionnaire (PAQ) score (n=1), the study population included 1258 patients enrolled in PORTRAIT between 2 June 2011 and 3 December 2015 at 16 PAD specialty clinics in the United States, the Netherlands and Australia. Men and women aged 21 years and older presenting with new-onset exertional leg symptoms, or a recent exacerbation of symptoms, and a resting ankle–brachial index (ABI) ≤0.90 or a drop in post-exercise ankle pressure of ≥20 mmHg were eligible for participation. Those with non-compressible vessels (ABI ≥1.30), critical limb ischemia, or who had undergone lower-limb endovascular or open vascular surgical procedures within the past year were excluded. Enrollment occurred before initiation of new or modification of existing treatments. The study was approved by the Institutional Review Boards of each participating center and all patients provided informed consent.
Clinical and health status characteristics
Demographic and clinical characteristics, psychosocial assessments, current and past treatments, disease severity, and PAD-specific health status were recorded at baseline and are summarized in Table 1. PAD-specific health status was measured using the PAQ, a 20-item, multi-dimensional instrument that is validated, reliable and responsive.2,10,11 A single item identifies the more symptomatic limb and the remaining 19 are answered according to variable Likert response scales to assess six domains: physical function, symptoms, symptom stability, social limitation, treatment satisfaction, and QoL. Each domain is transformed to a 0–100 score, with higher scores indicating better function, fewer symptoms, greater satisfaction with treatment, and higher QoL. The PAQ Summary Score, which also ranges from 0 to 100, combines all scales except treatment satisfaction and symptom stability. 10
Baseline sociodemographic, clinical and treatment characteristics in the overall population and according to baseline Peripheral Artery Questionnaire (PAQ) Summary Score tertile.

Continuous data are presented as mean ± standard deviation.
TIA, transient ischemic attack; CVA, cerebrovascular accident; MI, myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft.
Statistical analysis
Continuous variables were expressed as means (± standard deviations (SD)) and were compared across PAQ summary tertiles using linear trend tests. Categorical variables were reported as frequencies and percentages and were compared using the Mantel–Haenszel chi-squared test. In unadjusted analyses, continuous variables were related to the PAQ Summary Score using simple linear regression while categorical variables were related to this outcome using analysis-of-variance. Hierarchical, multivariable linear regression analyses, which accounted for the clustering of patients within site, assessed the independent association between patient characteristics and baseline PAQ Summary Scores. Variables that were considered for inclusion in the full model are listed in Table 1. All analyses were conducted with SAS software, Version 9.4 (SAS Institute Inc., Cary, NC, USA). A two-tailed p-value <0.05 was considered statistically significant.
The majority of patients (70%) were not missing any covariate information; 99% of patients were missing fewer than three covariates. The covariates had a missing rate ranging from 0 to 21%, with BMI (21.3%) and prior exercise (5.6%) having the highest rates. Missing covariate data were assumed to be missing at random and were imputed using multiple imputation methods. The imputation model consisted of all variables used in the multivariable model. Analyses were replicated on five imputed data sets and pooled to obtain final model estimates. 12
Results
The mean patient age was 68 years and 38% were women. The overwhelming majority (86%) described their symptoms as typical, defined as painful muscle cramping in the lower extremities when walking or exercising that resolves with rest, and half had bilateral symptoms. The US, Netherlands, and Australia accounted for 62%, 30% and 8% of enrollment, respectively. Vascular specialists included interventional cardiologists (41.1%), vascular surgeons (39.6%), non-invasive cardiologists (11.5%), vascular medicine specialists (5.2%), and interventional radiologists (0.1%). Baseline clinical and sociodemographic characteristics and treatment strategies for the overall population, stratified by tertiles of the PAQ Summary Score, are provided in Table 1. The mean (±SD) overall PAQ Summary Score was 49.2 (21.9). The PAQ Summary Score in the first (n=416), second (n=419) and third (n=423) tertiles, ranged from 0 to 38.8, 38.9 to 60.3 and 60.4 to 100, respectively. Baseline PAQ scores for the overall population and by PAQ Summary Score tertile are presented in Table 2.
Health status measures for the overall population and according to baseline Peripheral Artery Questionnaire (PAQ) Summary Score tertile.
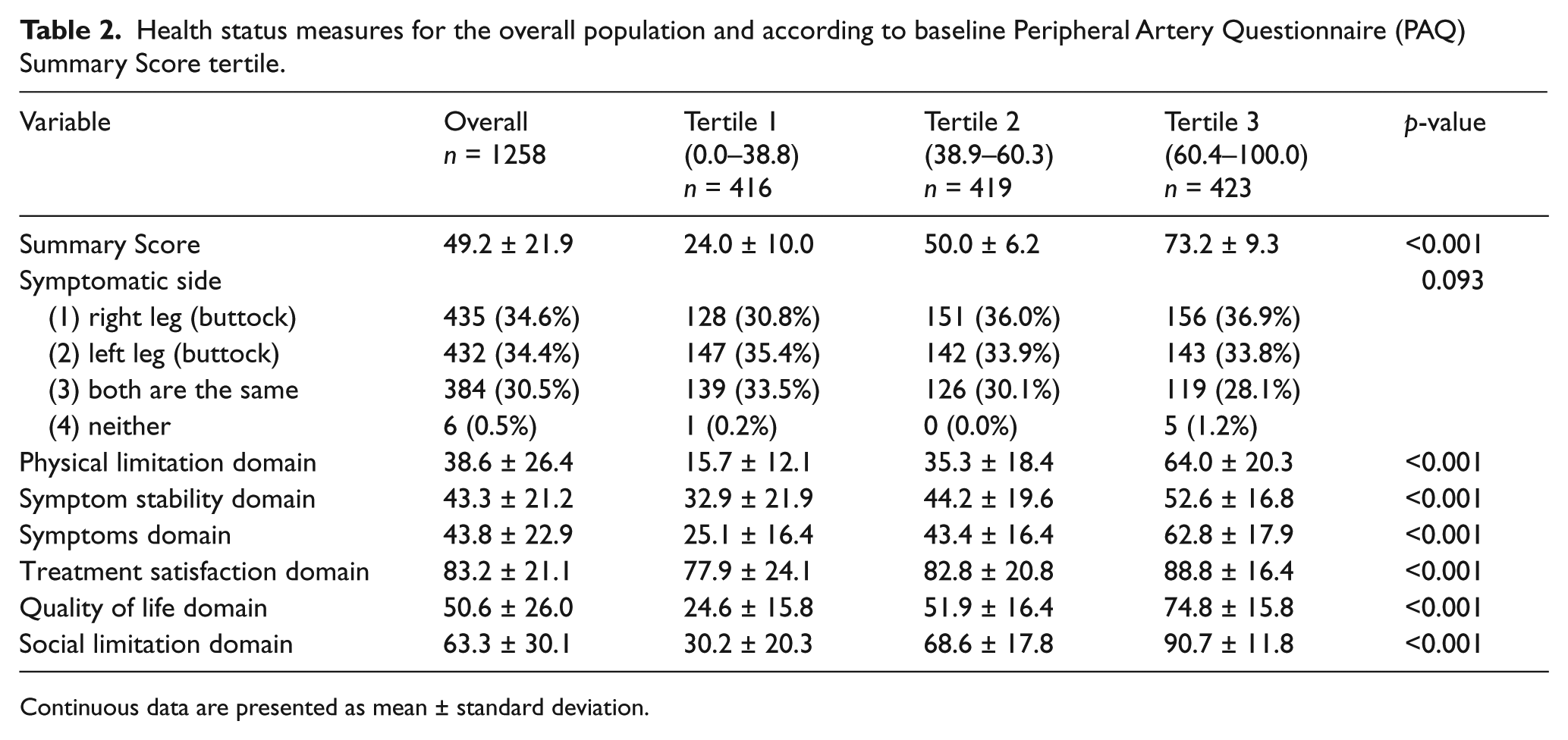
Continuous data are presented as mean ± standard deviation.
A number of patient characteristics were independently associated with lower baseline PAQ Summary Scores (i.e. poorer health status), including age (β = −3.0 per 10-year decrease, p < 0.001), female sex (β = −6.6, p < 0.001), not being married (β = −2.8, p = 0.02), economic burden (moderate/severe vs none: β = −3.7, moderate/severe vs some: β = −0.5, p = 0.03), difficulty getting care (moderate/severe vs none: β = −16.5, moderate/severe vs some: β = −10.9, p < 0.001), chronic lung disease (β = −3.6, p = 0.02), back pain (β = −5.8, p < 0.001), bilateral (vs unilateral) PAD (β = −2.7, p = 0.02), intermittent claudication severity (moderate vs mild: β = −6.9, severe vs mild: β = −12.9, p < 0.001), and lack of prior participation in an exercise program (β = −4.0, p = 0.005) (Figure 1). Cilostazol did not modify the relationship between claudication severity and PAQ Summary Score (interaction p = 0.29). No independent covariate interactions with country were significant.
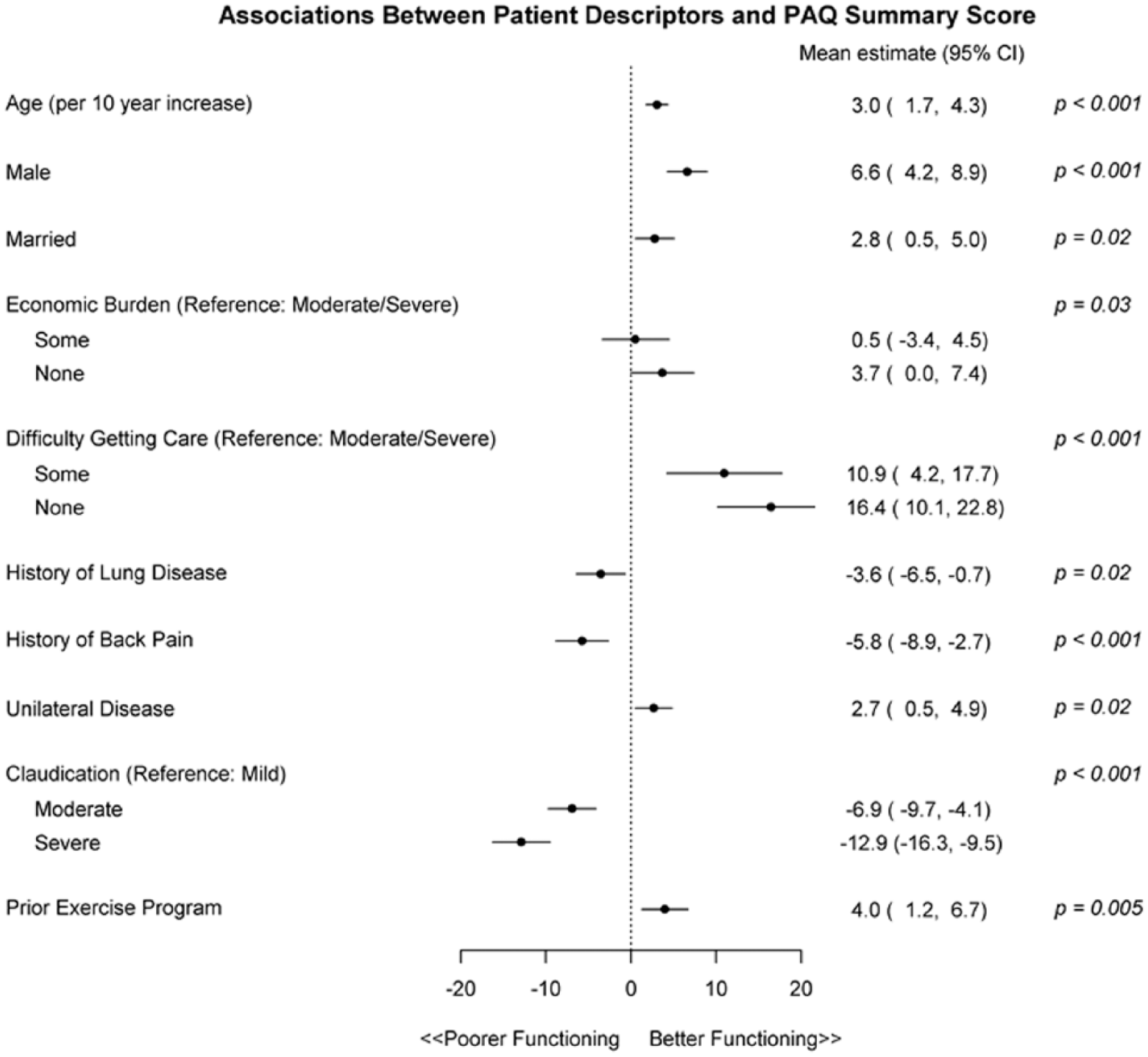
Independent predictors of the Peripheral Artery Questionnaire (PAQ) Summary Score.
Domain-specific predictors
Independent predictors were also identified for the individual PAQ domains (QoL, physical limitations, social limitations and symptom score) and are reported in Supplemental Tables 1–4. In general, domain-specific predictors were similar to those for PAQ Summary Score, although there were some differences. Independent predictors of QoL did not include lung disease or unilateral PAD. Independent predictors of physical limitations included having a high school level education, history of malignancy, ABI value and country of enrollment but not marital status. Independent predictors of social limitations included care avoidance due to cost but not economic burden, lung disease or prior participation in an exercise program. Finally, independent predictors of symptom score did not include economic burden, unilateral disease or prior exercise program participation.
Discussion
Understanding the profile of patients presenting for PAD specialty care can both identify potential patients with poorer access to care and assist physicians in considering additional factors that might influence treatment. In this international, prospective cohort study of patients with new or worsening intermittent claudication presenting for vascular specialty care, we identified important demographic, socioeconomic, vascular and non-vascular comorbid, symptom, and treatment-related characteristics associated with patient-reported health status, as captured by the PAQ. Younger age, female sex, not being married, greater economic burden, more difficulty getting care, chronic lung disease, back pain, bilateral (vs unilateral) PAD, more severe intermittent claudication and lack of prior participation in an exercise program were associated with poorer health status.
These findings extend the work of others 13 and provide new insights into the profiles of patients presenting with worse health status at the time of an initial visit with a vascular specialist. Prior reports, using generic questions about how patients are feeling or what they are experiencing,14,15 or through disease-specific QoL questionnaires13,16,17 designed to explore a particular range of problems and experiences confronting patients with PAD, 18 have found that sex, 13 age, 19 worsening ABI 20 and treatment predict QoL. We also observed that unmarried patients and those with back pain have significantly poorer disease-specific health status, relationships that have not been described to date. Finally, we identified several potentially modifiable characteristics associated with poorer health status, including difficulty in getting care and lack of participation in an exercise program.
It is notable that access to care was independently associated with health status in our population, in that those who had ‘no problem at all’ accessing care had higher PAQ scores. These results resonate with previous findings that health reform efforts, which increase access to care, are associated with a lower probability of presenting with severe PAD. 21 Efforts to improve health care access in this population seem like an important opportunity for policy makers and health care systems to consider in reducing health care disparities. With respect to exercise, the Centers for Medicare & Medicaid Services (CMS) have published a National Coverage Decision for supervised exercise therapy (SET) in patients with symptomatic PAD. 22 This measure will allow providers to translate the vast evidence base supporting SET into practice with expected improvements in health status.
Limitations
Our findings should be considered in the context of the following potential limitations. Given its observational design, selection bias and confounding may have impacted the observed relationships between identified predictors and our outcome of interest, although it is not possible to randomize patients to having different sociodemographic and clinical characteristics. Our study’s external validity may also be limited by the small number of participating centers, although we were able to include three countries in this study. Similarly, we were unable to examine the impact of race/ethnicity on PAD-specific health status in this cohort due to the homogeneity of the population studied. Finally, most patients in our study cohort reported typical, rather than atypical, intermittent claudication symptoms. This contrasts with the PARTNER study, where only 5.5% of those newly diagnosed with PAD had classic symptoms of intermittent claudication. 7 That ours was a population largely comprised of patients with typical symptoms may suggest that only patients with the most ‘typical’ symptoms are recognized and subsequently referred for vascular specialty care while those with atypical symptoms (the majority) remain undetected or undertreated.
Conclusion
Disparities in sociodemographic, clinical and treatment characteristics were associated with poorer PAD-specific health status at the time of presentation, with new or worsened claudication for advanced vascular care. Better awareness of such disparities may permit a more proactive and tailored response, and in doing so improve upon disease diagnosis and management moving forward.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Soukas is an unpaid consultant to WL Gore, Spectranetics, Cordis, and Bard; he receives research/grant support from WL Gore, Spectranetics, Intact Vascular, Juventas Therapeutics, Medtronic, and Biotronik. Dr Spertus owns the copyright to the Peripheral Artery Questionnaire. Dr Smolderen is supported by an unrestricted research grant from Boston Scientific and Merck. Drs Noyes, Abbott, Gosch, Hyder, Shishehbor and Aronow have no disclosures.
Funding/Role of Sponsor
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: a Patient-Centered Outcomes Research Institute (PCORI) Award (IP2 PI000753-01; CE-1304-6677); a VENI Grant from The Netherlands Organisation for Scientific Research (No. 916.11.179); and an unrestricted grant from WL Gore & Associates, Inc. (Flagstaff, AZ, USA).
The statements in this manuscript are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI), its Board of Governors or Methodology Committee
All manuscripts for the PORTRAIT study are prepared by independent authors who are not governed by the funding sponsors and are reviewed by an academic publications committee before submission.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.