
Abstract

Introduction
Fibromuscular dysplasia (FMD) is an uncommon vascular disease that affects the arteries of the body and is more commonly seen in women. Though FMD was first described in 1938, only in the past decade have there been major advances in the understanding of this condition. In 2017, FMD remains poorly understood by many medical professionals, and arriving at the right diagnosis can be difficult, even for patients who have symptoms of this disease.
What is FMD?
Arteries are the blood vessels that carry oxygenated blood to the brain, the organs of the body, and the arms and legs. FMD affects medium-sized arteries, and it is different than atherosclerosis or plaque build-up within the arteries. In FMD, instead of plaque, fibrous tissue and webs develop in the artery wall and can lead to narrowing of the arteries. Patients with FMD can also develop bulging of the artery wall (aneurysms) or tears (dissections) of arteries and can have very twisty (tortuous) arteries. In most cases, it is possible to distinguish the artery blockages of FMD from those of atherosclerosis or plaque based on the appearance of the blockage or its location in an artery. Artery blockages due to atherosclerosis or plaque build-up tend to develop at a branch point in an artery, whereas blockages due to FMD tend to develop further along in the vessel. Sometimes patients can have both FMD and atherosclerosis within arteries, especially in older patients.
Types of FMD: Multifocal and focal
Experts in the field of FMD have proposed an updated naming system for FMD. 1 According to this terminology, there are two types of FMD: multifocal and focal. These two types differ in how the arteries appear on imaging studies and what layer of the artery wall is affected by the build-up of fibrous tissue. Multifocal FMD is by far the more common type of FMD, affecting 90% or more of FMD patients. The hallmark of this type of FMD is the ‘string of beads’ appearance of the artery (Figure 1A). This appearance occurs when areas of artery narrowing due to fibrous tissue and webs alternate with areas of artery enlargement or dilation. This ‘string of beads’ is widely recognized as a sign of FMD. Meanwhile, focal FMD, which is much less common, usually consists of a single, smoother narrowing in an artery (Figure 1B). The focal type is more common among children and teenagers diagnosed with FMD.
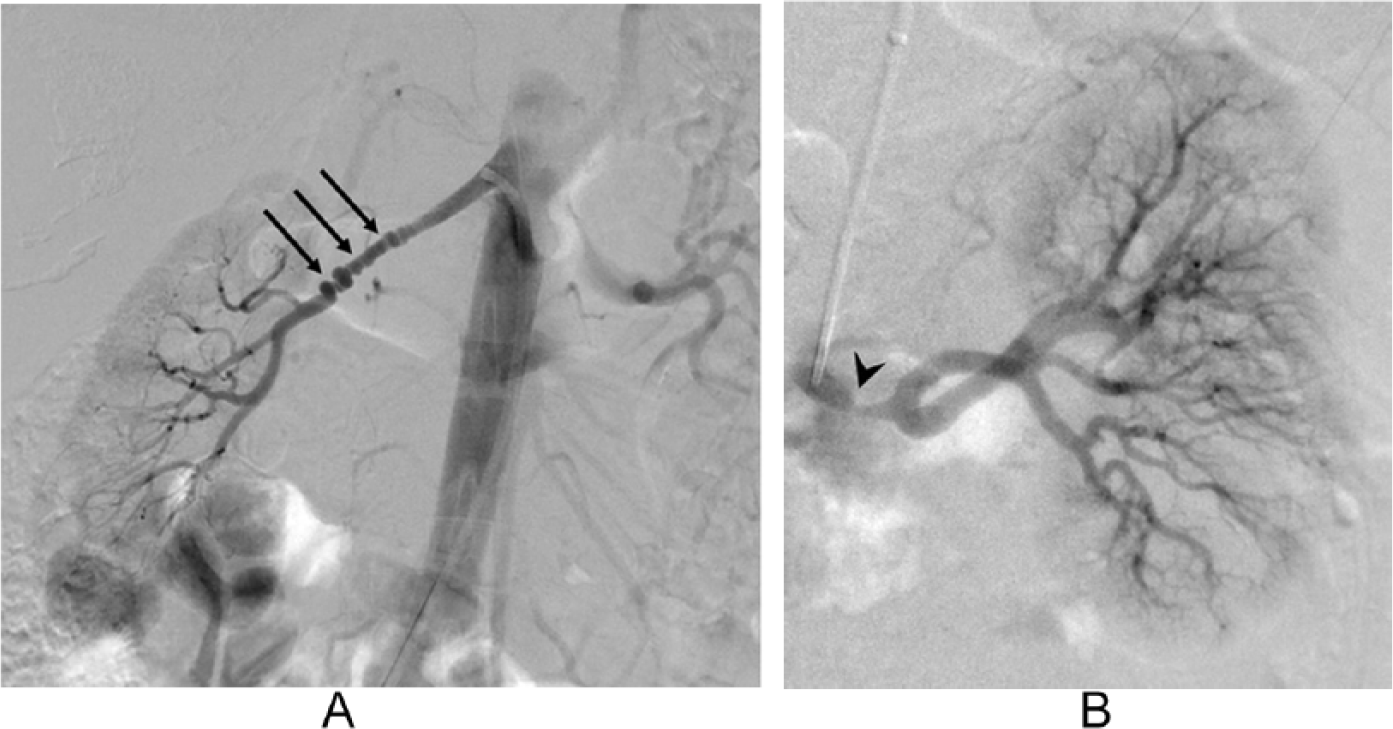
Catheter-based angiography of renal arteries showing (A) ‘string of beads’ (arrows) in multifocal fibromuscular dysplasia (FMD) and (B) a single narrowing of focal FMD (arrow head).
What arteries are involved in FMD?
As mentioned above, FMD affects the medium-sized arteries of the body. The most commonly affected areas are the arteries leading to the kidney (renal arteries) and the arteries that supply blood flow to the brain (carotid and vertebral arteries). Other arteries in the body that can develop FMD include arteries supplying the intestines (mesenteric arteries) and those to the legs (external iliac arteries) and arms (brachial arteries). Rarely, other arteries can be affected by FMD.
What causes FMD?
The short answer: we still don’t know. There is likely a genetic component to the development of FMD, but, despite some promising recent advancements, no single genetic cause has been identified. Research is still underway to identify genetic causes of FMD. According to data from the United States FMD Registry, fewer than 8% of patients with FMD also have a family member with the disease, but other vascular conditions may be more common among family members of FMD patients, such as aortic or brain aneurysms. 2 Environmental factors probably interact with genetic factors, such as female sex, in the development of FMD.
Although FMD has traditionally been considered ‘rare’, in reality FMD may be more common than previously thought. Still, the exact number of people affected by FMD (known as the prevalence) is unknown. 3 FMD is far more common in women than in men, with over 90% of those affected being female. 2 Because the overwhelming majority of FMD patients are women, hormonal factors may contribute to FMD development. While a small minority of FMD patients are men, men with FMD seem to have a more aggressive form, with a twofold greater risk of artery aneurysms or dissections compared to women. 4 Additionally, FMD is not restricted to adults. Children can also develop FMD, usually with the focal type causing high blood pressure.
Although the cause of FMD remains elusive, certain risk factors exacerbate it, the main one being smoking. A recent study from the United States FMD Registry found that FMD patients who smoke are more likely to have aneurysms, more likely to experience leg pain with exertion (claudication), more likely to require some type of vascular intervention, and as a whole are more likely to experience major vascular events such as stroke or heart attack compared to patients who have never smoked. 5
What are the common symptoms of FMD?
Symptoms of FMD are quite variable and depend on the location, severity, and type of FMD. Some patients with FMD may have no symptoms at all. According to data from the United States FMD Registry, common signs and symptoms are high blood pressure (hypertension), headache (especially migraine type), and pulsatile tinnitus, which patients describe as hearing a ‘swishing’ or ‘whooshing’ sound in their ears that matches the timing of their own heartbeat. 2 Hypertension is the most common sign of kidney artery FMD. Patients with carotid or vertebral artery FMD more commonly complain of headaches and pulsatile tinnitus and can have other symptoms such as neck pain or dizziness.
Unfortunately, more severe symptoms can develop in some patients with FMD. Stroke, or a ‘mini-stroke’ (transient ischemic attack or TIA), ruptured brain aneurysm, or a carotid or vertebral artery dissection can develop in patients with cerebrovascular FMD. Patients with FMD can also develop dissections in other arteries of the body, such as the kidney (renal) arteries, leading to blockage of blood flow to the kidneys, which can cause lower back and side (flank) pain and may cause blood in the urine. Recently, studies have found that patients with FMD can develop a heart attack (myocardial infarction) due to spontaneous coronary artery dissection (SCAD). 6 SCAD is a blood clot of the coronary artery wall due to a tear in the artery or a bleed into the vessel wall that can lead to compromised blood flow to the heart muscle, causing a myocardial infarction.
Although FMD can manifest very dramatically in some patients with a stroke or heart attack, fortunately, the majority of FMD patients do not experience such dangerous vascular events.
What is a bruit?
Another common sign of FMD is a bruit on physical examination. A bruit is an abnormal sound heard over an artery using a stethoscope, and it indicates turbulent blood flow. This turbulent flow of blood is usually a sign of a narrowed artery and is commonly heard in the setting of a ‘string of beads’ in an artery due to FMD, but also can be heard with other artery abnormalities. Bruits heard in FMD patients provide clues as to which arteries are affected. Bruits are most commonly heard over the abdomen or flanks, in the neck, or in the upper legs (groin area). Since renal and carotid arteries are the most common locations with FMD, abdominal and neck bruits are most often heard.
How is FMD diagnosed?
The diagnosis of FMD is made by imaging studies; there is no blood test for FMD and biopsies are not performed. Diagnosing FMD can sometimes be a difficult task since other conditions that cause artery abnormalities may look like FMD (such as atherosclerosis or an artery dissection).
Catheter-based (invasive) angiography remains the gold standard test for diagnosing FMD. This test involves creating high quality X-ray-type pictures of the arteries by injecting dye through catheters that are most commonly inserted through the groin (Figures 1 and 2A). This method is not used to diagnose FMD in routine clinical practice given its invasive nature, expense, and use of both radiation and iodine-based contrast dye. Instead, angiography is used to diagnose FMD only if other imaging studies have been unclear or if a procedure is needed (such as angioplasty).
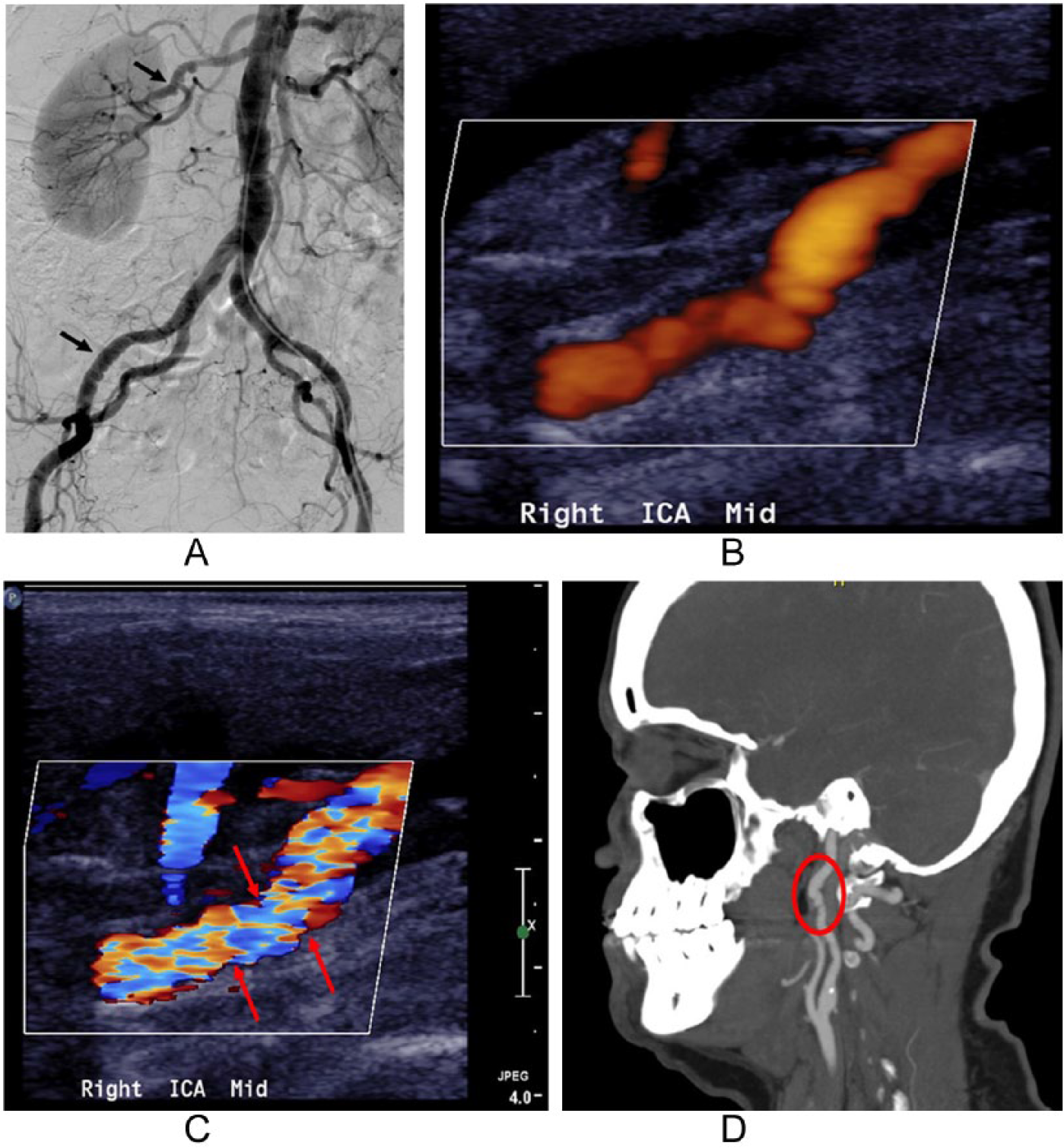
Different imaging tools to visualize multifocal fibromuscular dysplasia (FMD). (A) Catheter-based angiogram (CTA) showing ‘string of beads’ of the renal (upper arrow) and external iliac (lower arrow) arteries. Ultrasound showing (B) beading and (C) turbulent flow (indicated by red arrows pointing to mosaic of colors) in the right internal carotid artery. (D) CTA demonstrating beading of the internal carotid artery (red oval).
Fortunately, other imaging techniques have been proven to be very successful in diagnosing FMD and have the added benefit of being non-invasive and widely accessible. These non-invasive imaging tools include vascular duplex (or Doppler) ultrasound, magnetic resonance angiography (MRA), and computed tomography angiography (CTA).
Duplex (or Doppler) ultrasound uses sound waves to visualize the blood vessels and assess the speed and character of blood flow in vessels. Features of FMD that can be identified with duplex ultrasound include beading (Figure 2B), turbulent blood flow and abnormally high speed (velocity) blood flow (Figure 2C), and tortuosity or ‘S’-shaped arteries. In some cases, although beading can be seen with duplex ultrasound, it is better appreciated by other types of imaging studies such as catheter angiography, CTA, or MRA. CTA and MRA are non-invasive imaging tests that use different techniques to create detailed vascular images. Both CTA (Figure 2D) and MRA can be used to create detailed reconstructions of the anatomy of the arteries and are accurate in visualizing aneurysms, dissections, and areas of beading. Recently, Lau and colleagues published a detailed Patient Information Page on these imaging modalities. 7
Deciding which type of imaging to use for diagnosis or follow-up of FMD depends upon the vessels that need to be imaged, patient factors (such as allergy to contrast dye or kidney problems), and local availability and expertise. Once FMD is diagnosed, it is often recommended that patients undergo comprehensive one-time imaging of the arteries from head to pelvis to determine which areas are affected and to check for any aneurysms or dissections of arteries. Subsequent follow-up may be limited to imaging of the areas of the body that are involved with FMD, and in some cases may be as simple as periodic duplex ultrasound studies. The frequency of repeating surveillance imaging studies is customized for each patient.
How is FMD treated?
Unfortunately, there is no cure for FMD. It is a chronic medical condition, but one that can be treated and managed with good outcomes with an individualized plan of care. The treatment plan for each patient includes consideration of symptoms, the location of the arteries involved, the severity, and whether or not the patient has any aneurysms or dissections. Care for patients with FMD is a combination of education, monitoring with imaging, lifestyle modification, and medication (Table 1). Some patients with FMD will also undergo vascular procedures. It is important to work with a physician or a team of physicians who are familiar with FMD and who will work collaboratively with other specialists in providing patient care. Physicians who may have expertise in the care of patients with FMD can include vascular medicine specialists, vascular surgeons, cardiologists, interventional radiologists, nephrologists, and neurologists, among others. We hope that greater awareness and progress in researching this disease will result in more physicians who have significant experience in caring for patients with FMD.
Components of care for patients with FMD.
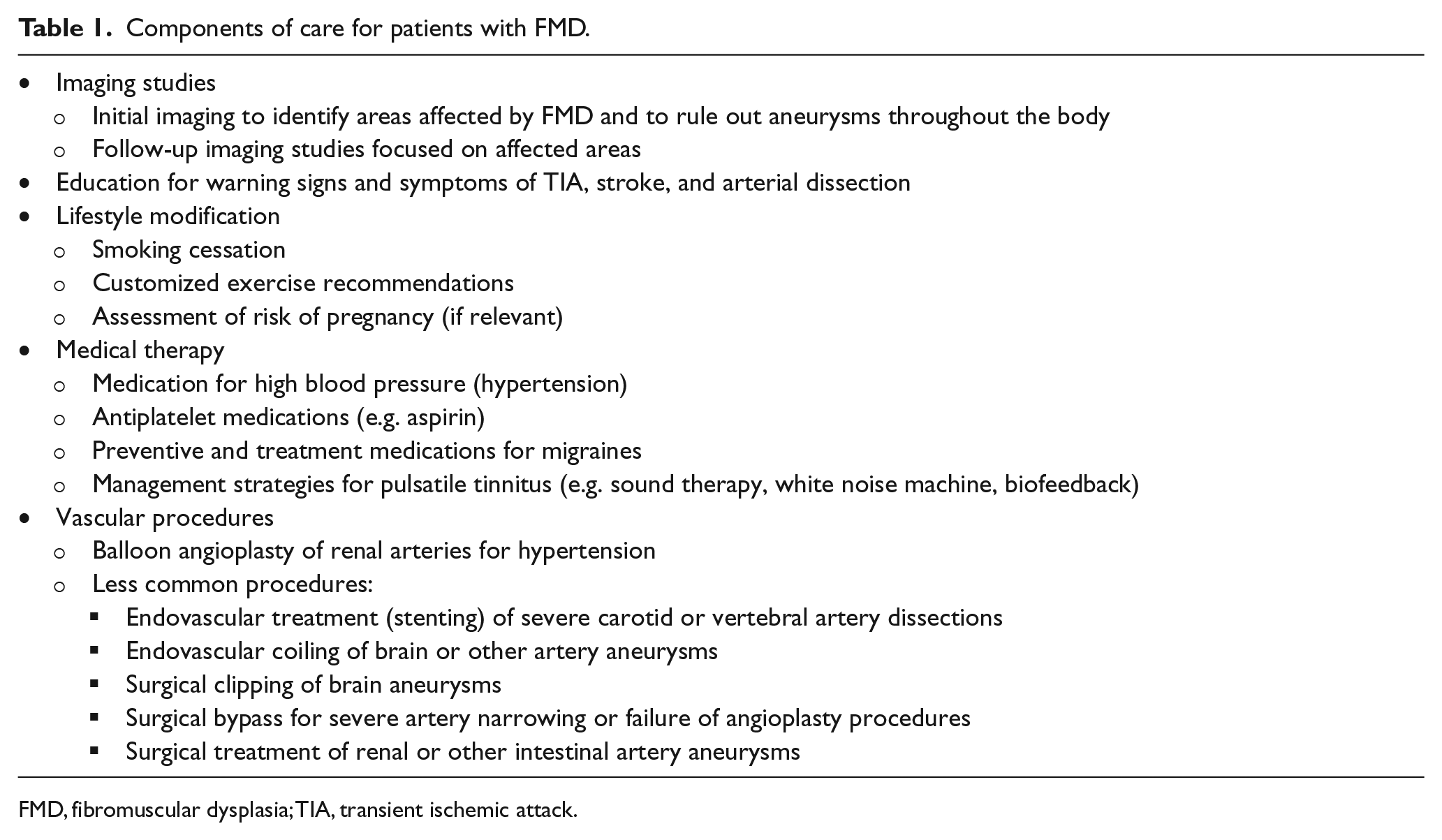
FMD, fibromuscular dysplasia; TIA, transient ischemic attack.
Medical therapy plays a large role in the care of FMD patients. Since high blood pressure is common among patients with FMD, blood pressure-lowering medications and blood pressure monitoring are important components of the treatment plan. Blood-thinners (antiplatelet agents), such as aspirin, are often used to reduce the risk of vascular events in patients with FMD, especially those with carotid or vertebral FMD. Since many patients with FMD suffer from headaches or migraines, medications to prevent and treat migraine may be prescribed. For FMD patients who have severe or frequent headaches, a headache specialist can be helpful to explore treatment options to improve and manage the associated pain and discomfort. For patients with bothersome pulsatile tinnitus, sound therapy and consultation with an ENT physician or audiologist may be helpful.
Patients with FMD may need to undergo vascular procedures, such as endovascular procedures or vascular surgery, depending on the severity of their symptoms. Vascular procedures may also be required to treat aneurysms, even if the patient has no symptoms. Percutaneous transluminal angioplasty (PTA) of the renal arteries, also called balloon angioplasty, is the most common procedure performed on patients with FMD. The goal of renal artery angioplasty is to improve high blood pressure, particularly blood pressure that has been resistant to aggressive medical treatment. Renal artery angioplasty may also be recommended in the setting of a new diagnosis of high blood pressure due to FMD, particularly in younger patients, with a goal of curing this high blood pressure. Other vascular procedures for FMD may be necessary in cases causing severe symptoms. Patients with FMD who have sizable brain aneurysms may require endovascular coiling or surgical clipping to prevent stroke due to aneurysm rupture. However, many patients with FMD are managed with medication and follow-up alone.
Living with FMD
In addition to medical therapy and monitoring with imaging, patients with FMD should be educated about warning signs of severe complications, such as artery dissection, TIA, stroke, and heart attack. Hopefully none of these events will occur with good medical care and monitoring, but if any of these complications do occur, prompt medical attention is key, and emergency health care providers should be informed that the patient has FMD. Some FMD patients wear medical alert jewelry for this reason.
The diagnosis of FMD may come with recommended lifestyle modifications. Patients with FMD who smoke must quit smoking to decrease the risk of major vascular events. 5 Maintaining a healthy body weight and nutritious diet are recommended, and this is particularly important for FMD patients with high blood pressure. Depending on the location and severity of the FMD, patients may be advised to refrain from certain activities, such as lifting heavy objects, extreme or contact sports, roller coaster rides, and undergoing chiropractic neck manipulations. These restrictions are related to the potential risk of arterial dissection. That being said, exercise is important for overall cardiovascular health and well-being for all patients, including those with FMD, and there is generally no limitation on moderate aerobic exercise. As always, recommendations for exercise should be customized to the individual patient by his or her physician.
Though FMD tends to be diagnosed later in life, FMD patients of childbearing age should discuss the risk of pregnancy with their doctors, and this discussion should occur long before pregnancy is contemplated.
Research and resources
Sponsored by the Fibromuscular Dysplasia Society of America (FMDSA), which is located in Rocky River, Ohio, the United States FMD Registry began enrolling patients in 2009. The United States Registry has collected data that have advanced the understanding of the symptoms, diagnosis, epidemiology, natural history, and outcomes of FMD and have helped to raise awareness about FMD in the medical community. Fourteen centers are currently enrolling in the US Registry, and more than 1600 patients have been enrolled to date. In addition to sponsoring the US Registry, the FMDSA provides resources and support for patients and health care providers interested in FMD, including an online support network and regional FMD patient support communities. The FMDSA hosts an FMD patient meeting in Cleveland, Ohio each May that includes clinical and research updates and opportunities for fellowship and support among FMD patients. Further details regarding the FMDSA are available at www.fmdsa.org or by phone at +1 216-834-2410.
The movement to understand FMD and thus to improve care for patients with this disease is not restricted to the United States. A European FMD registry initiative is well under way involving a network of clinical centers in Europe. Presently, the main coordinating countries for the European registry include Belgium, France, and The Netherlands, and the European initiative intends to expand to other European countries with time. 8
Summary
FMD is an uncommon vascular disease of unknown cause that affects medium-sized arteries and can lead to narrowing and beading of the arteries as well as artery dissections or aneurysms. More than 90% of patients with FMD are women. The location of artery involvement, type of FMD (multifocal or focal), and severity of symptoms are highly variable among patients. Common signs and symptoms of FMD are high blood pressure, headaches (especially migraines), and pulsatile tinnitus. Recently, FMD has been recognized among some patients who suffer a heart attack due to coronary artery dissection. Patients with FMD should have an individualized management plan that incorporates periodic clinical assessment and follow-up imaging, patient education, medical therapy, and lifestyle modification. Vascular procedures may be needed for some patients to treat high blood pressure or other severe symptoms, or for treatment of aneurysms. Research and resources are constantly evolving to provide better understanding of this disease and thus to improve the quality of care for affected patients.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Heather L Gornik is a member of the Medical Advisory Board of the FMD Society of America, a non-profit organization.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.