
Abstract
Venous thromboembolism (VTE) contributes to significant morbidity, mortality, and socioeconomic burden. There is a paucity of literature regarding sex-based sociodemographic differences in VTE presentation and short-term outcomes. We aimed to compare clinical outcomes between men and women hospitalized for VTE management. We performed a retrospective analysis using data from the National Inpatient Sample (NIS) database from 2012 to 2013. Inclusion criteria were age 18 years and older and a primary discharge diagnosis of VTE. Sociodemographic features and medical comorbidities were analyzed, as were hospital length of stay and in-hospital mortality rates. A total of 107,896 patients met the inclusion criteria; 53% were female. Median age was 65 years (interquartile range 51–77) and women were older than men (65 vs 62 years, p<0.001). There were significant differences between men and women with respect to race, primary insurance payer and medical comorbidities, and small differences with respect to VTE location. Female sex was associated with a small but significantly longer hospital length of stay (mean ratio 1.04, 95% CI 1.03–1.05, p<0.001) but no significant difference in in-hospital mortality (2.2% vs 2.1%, p=0.15). In a multivariate model, there was no significant difference between women and men with respect to hospital length of stay or in-hospital mortality. In conclusion, we used data from the NIS to study over 100,000 patients hospitalized for VTE, and identified several sex-based disparities in sociodemographic factors and location of VTE. However, in a multivariable analysis correcting for these factors, sex was not associated with significant differences in clinical outcomes.
Introduction
Venous thromboembolism (VTE), including both deep venous thrombosis (DVT) and pulmonary embolism (PE), contributes to significant morbidity and mortality both in the United States as well as worldwide.1,2 Between 300,000 and 600,000 cases of VTE are diagnosed each year. 3 Case fatality rates range from 10% to 20% or higher, and VTE-associated mortality accounts for up to 100,000 deaths each year.4–7 Additionally, VTE is associated with a substantial economic burden on hospitals and the health care system as a whole. Treatment of acute VTE and associated complications is estimated to cost up to $18,000–23,000 per incident case and cost the US health care system 7–10 billion dollars per year. 8
The substantial health care and health economic impact of VTE-related morbidity and mortality makes the identification of risk factors for VTE and disparities in VTE management and outcomes an extremely important component of health services and outcomes research. Multiple risk factors for VTE have been identified, including inherited thrombophilias and acquired risk factors including age, race, obesity, cigarette smoking, surgery and prolonged immobility, hospitalization, pregnancy, hormone therapy, malignancy, and other comorbid medical conditions.9–14
Despite the fact that sex is an essential epidemiologic characteristic and influences risk and outcomes in many health conditions, the role of sex in VTE has not been fully characterized. Male sex is associated with an increased risk of recurrent VTE, 15 but the relationship between sex and risk of incident VTE is less well defined and may vary based on whether reproductive and hormonal risk factors are taken into account during analysis.16–18 There are little data regarding how sex may influence outcomes during acute treatment episodes. We hypothesized that sex may be associated with other risk factors for VTE and that there may be sex-based disparities in outcomes, and aimed to compare clinical outcomes of patients hospitalized for VTE management in men versus women.
Methods
Data source and patient population
The National Inpatient Sample (NIS) is a component of the Healthcare Cost and Utilization Project (HCUP) sponsored by the Agency for Healthcare Research and Quality (AHRQ). The NIS database is the largest publically available all-payer inpatient database in the United States. 19 NIS data from the years 2012 and 2013 were used for this analysis. Patients were included if they were 18 years of age or older and had a primary ICD-9 discharge diagnosis code of deep venous thrombosis of the lower extremity (453.40, 453.41, 453.42), deep venous thrombosis of the upper extremity (453.82, 453.84, 453.85, 453.86), or pulmonary embolism (415.11, 415.12, 415.13, 415.19). We selected patients using the primary diagnosis code alone as a way of minimizing the inclusion of patients who developed VTE during the hospital stay rather than as a primary reason for hospital admission. Patients meeting inclusion criteria but with additional diagnosis codes of chronic deep venous thrombosis and/or pulmonary embolism or personal history of venous thromboembolism (453.71–453.79, 416.2, V12.51) were excluded, as were patients with a concurrent diagnosis of superficial venous thrombosis or venous thrombosis of an unspecified site (453.81, 453.83, 453.87, 453.89, 453.6) in an attempt to select a population specifically of those patients with DVT of the extremities or PE.
Data were collected from three categories including NIS Core Data Elements (sex, race, age, geographic location, urban versus rural setting, primary payer, median income for zip code, length of stay, and hospital mortality), NIS Hospital File Data Elements (hospital bed size, teaching or non-teaching hospital), and NIS Severity File Data Elements, which captures 29 discrete conditions labeled ‘comorbidities’ which are extracted from AHRQ co-morbidity severity files. Outcomes were defined using specific NIS Description of Data Elements coding for ‘DIED’ (inpatient mortality) and ‘LOS’ (length of stay)
Missing data
Nine percent of patients were missing at least one of the baseline characteristics, sex, or clinical outcome. No single variable was missing more than 5%. Hot deck imputation was used to create a complete data set by substituting missing values from subjects who were similar to those missing data. A similarity score between subjects was measured using all available data. Missing values were substituted from the subject who was most similar to each recipient. Of the 10 patients missing sex, five were imputed as male and five were imputed as female. Clinical outcome results were calculated using the completed data set.
Statistical analysis
Descriptive characteristics were compared between men and women using the Rao-Scott chi-squared test. Chi-squared test statistics that were significant were followed-up with residual analysis to determine which characteristics contributed to the significant difference between men and women. The residual analysis is a comparison of observed and expected counts in each cell of a contingency table; it helps describe where differences exist between row and column variables. Standardized residuals greater or less than ± 2 were considered to be significant.
In-hospital mortality was compared between men and women by odds ratio (OR), which was estimated using logistic regression. Logistic regression was also used to estimate the odds ratio for mortality between men and women, controlling for confounders. In-hospital mortality results were also stratified by thrombosis location. LOS was compared between men and women using log-gamma regression. This model provides the mean ratio (LOS for women : LOS for men), where values >1 indicate longer LOS for women compared to men. Any patient with a zero day stay was set to have a half day LOS. Results were also stratified by VTE location. All analyses accounted for the sampling design and survey weights. Descriptive statistics were calculated using SAS software, Version 9.4 (SAS Institute Inc., Cary, NC, USA). Imputation and regression models were performed using R version 3.1.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics
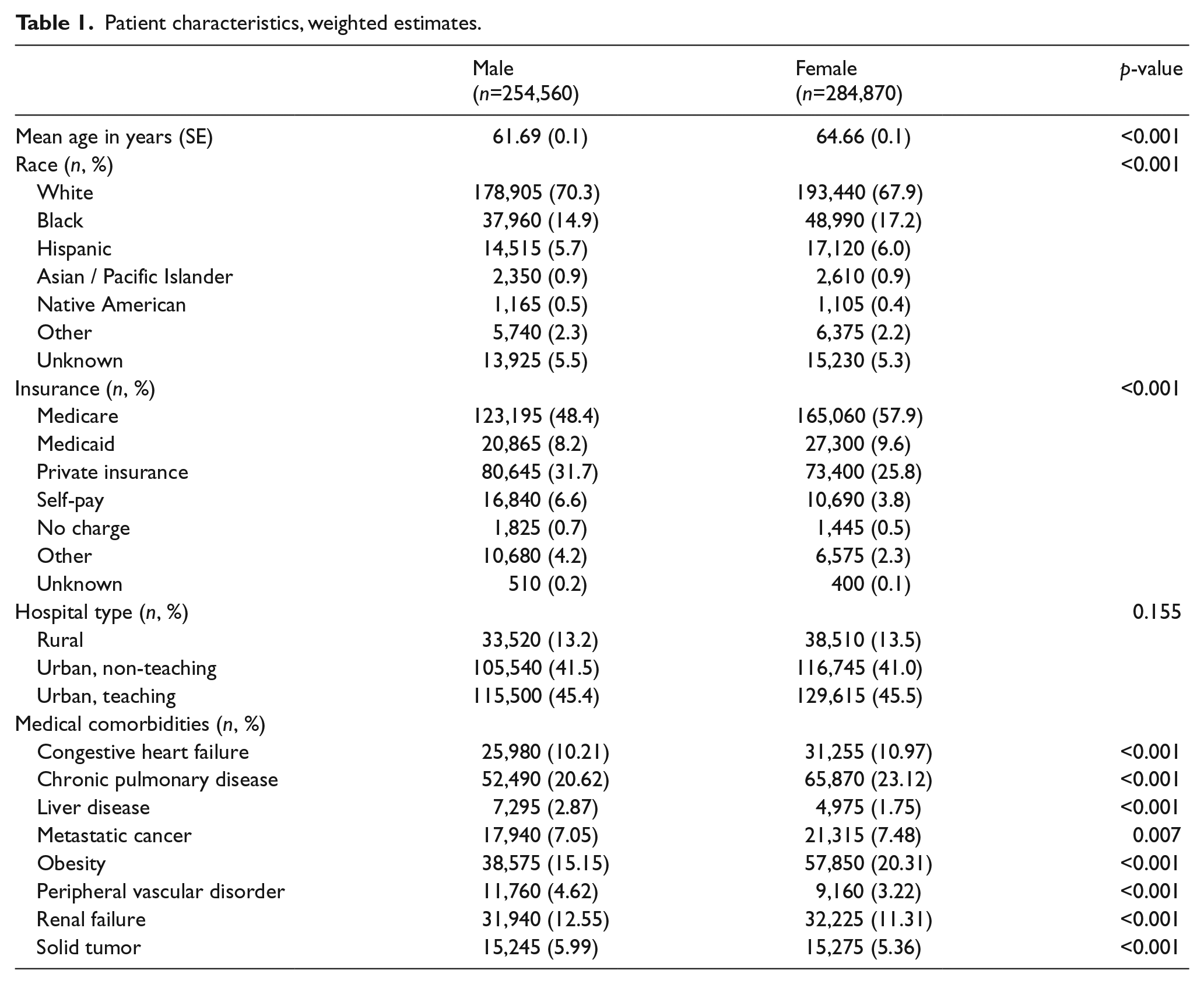
A total of 107,896 patients met the inclusion criteria for the 2-year period between 1 January 2012 and 31 December 2013 (weighted total = 539,430); 53% were female and 47% were male. Table 1 shows baseline characteristics and medical comorbidities of the original weighted sample (no imputation, missing data shown). The median age was 65 years (interquartile range 51–77) and women were significantly older than men (65 vs 62 years, p<0.001). There were significant differences between men and women with respect to race (p<0.001). The chi-squared test result was primarily driven by differences in white (more male) and black (more female) racial differences. The percentage of men versus women with each type of primary insurance payer differed significantly (p<0.001 by all types). Standardized cell residuals ranged from 3 to 15. There were also significant differences between women and men with respect to medical comorbidities including alcohol abuse, liver disease, and renal failure (more common in men) and baseline anemia, valvular heart disease, and obesity (more common in women).
Patient characteristics, weighted estimates.
We analyzed differences in women versus men with respect to VTE location and severity, and these results are presented in Table 2A. There were no sex-based differences with regards to PE with or without cor pulmonale. However, a significantly larger percentage of men had proximal DVT versus distal DVT (proximal DVT 58.1% in men and 56.7% in women, p = 0.003). The percentage of patients undergoing surgical thrombectomy as part of VTE management is presented in Table 2B. A significantly larger percentage of men underwent thrombectomy compared to women for all types of VTE (PE, lower and upper extremity DVT) and the difference was largest for upper extremity DVT (9.1% of men underwent thrombectomy compared to 5.5% of women; p<0.001).
Location of venous thrombosis.
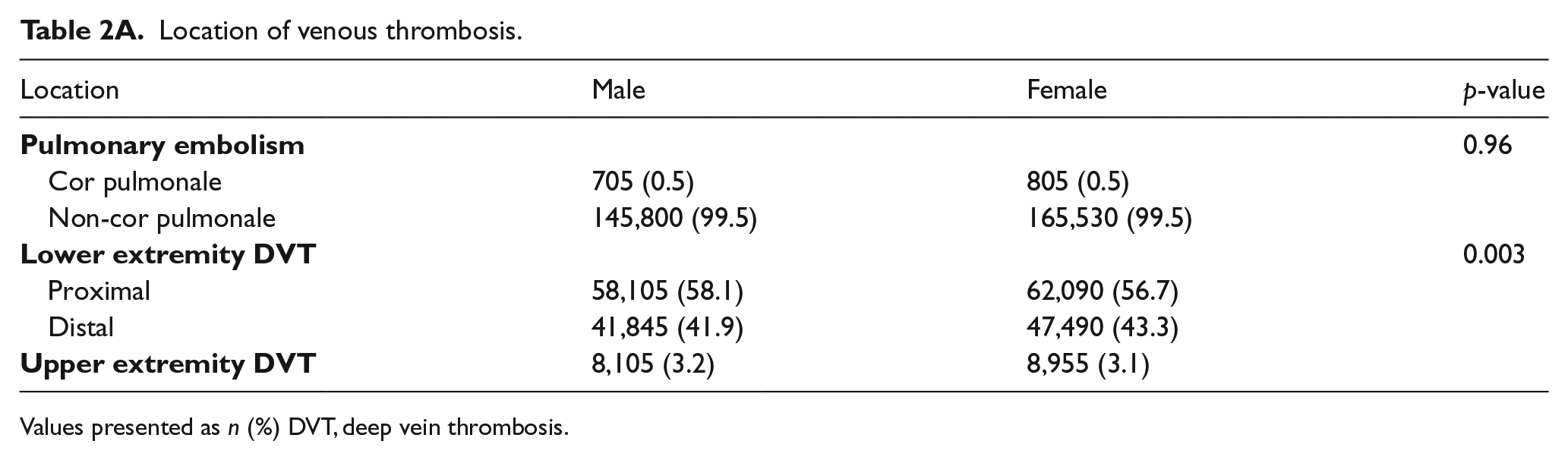
Values presented as n (%) DVT, deep vein thrombosis.
Surgical management of thrombosis.
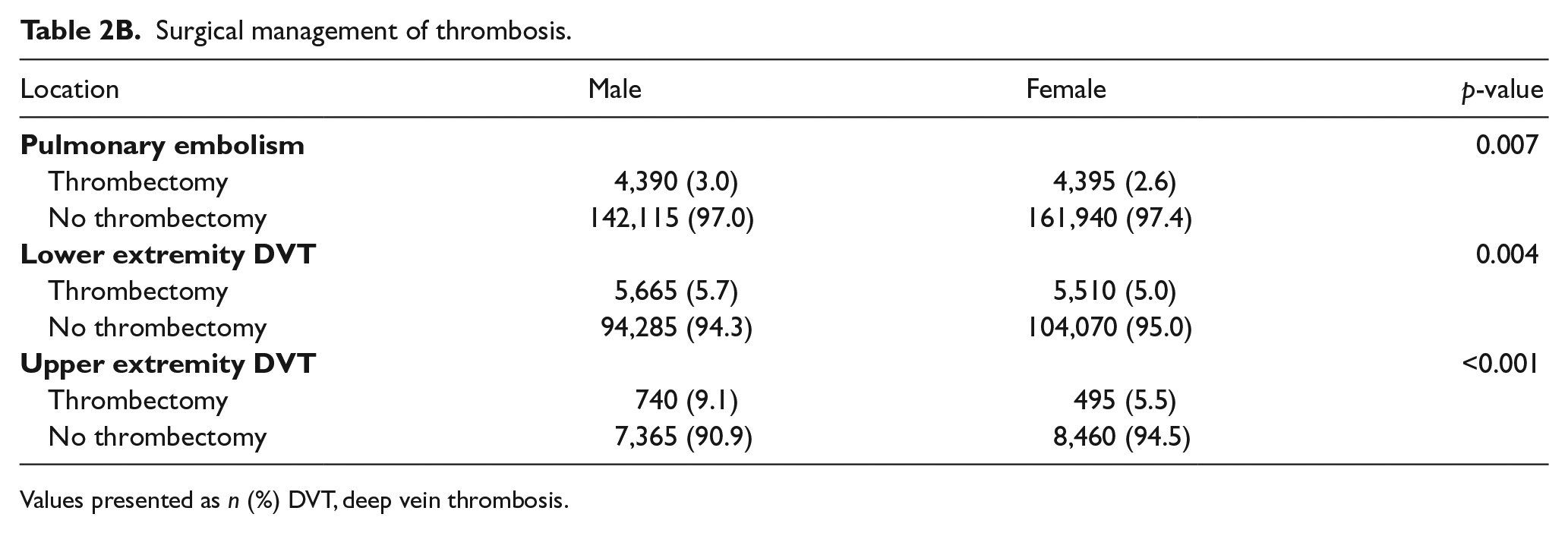
Values presented as n (%) DVT, deep vein thrombosis.
Sex-based differences in clinical outcomes
Clinical outcomes data are shown in Tables 3, 4A and 4B. The unadjusted hospital LOS differed significantly between men and women, with women having a 4% longer LOS than men (mean ratio 1.04, 95% CI 1.03–1.05, p<0.001). When stratified by type of VTE event, women with lower extremity DVT and PE had a significantly longer hospital LOS, while there was no difference in LOS between women and men among those with upper extremity VTE. The mean ratios in the unadjusted analysis were all close to 1.0; findings were no longer significant after controlling for age, race, insurance status, hospital division, and medical comorbidities. A second analysis was performed using listwise deletion and the results are almost identical; results are presented in the online supplemental Table 3. When analyzed by VTE location and severity (Table 4A), both men and women with PE complicated by cor pulmonale had a longer LOS (median of 6 days vs 4 days for PE not complicated by cor pulmonale) but there was no significant sex-based difference in this regard. There were small differences in hospital LOS with regard to sex-based proximal and distal lower extremity DVT but again the mean ratios were all close to 1.0.
Comparison of hospital length of stay and inpatient mortality by sex and VTE location.
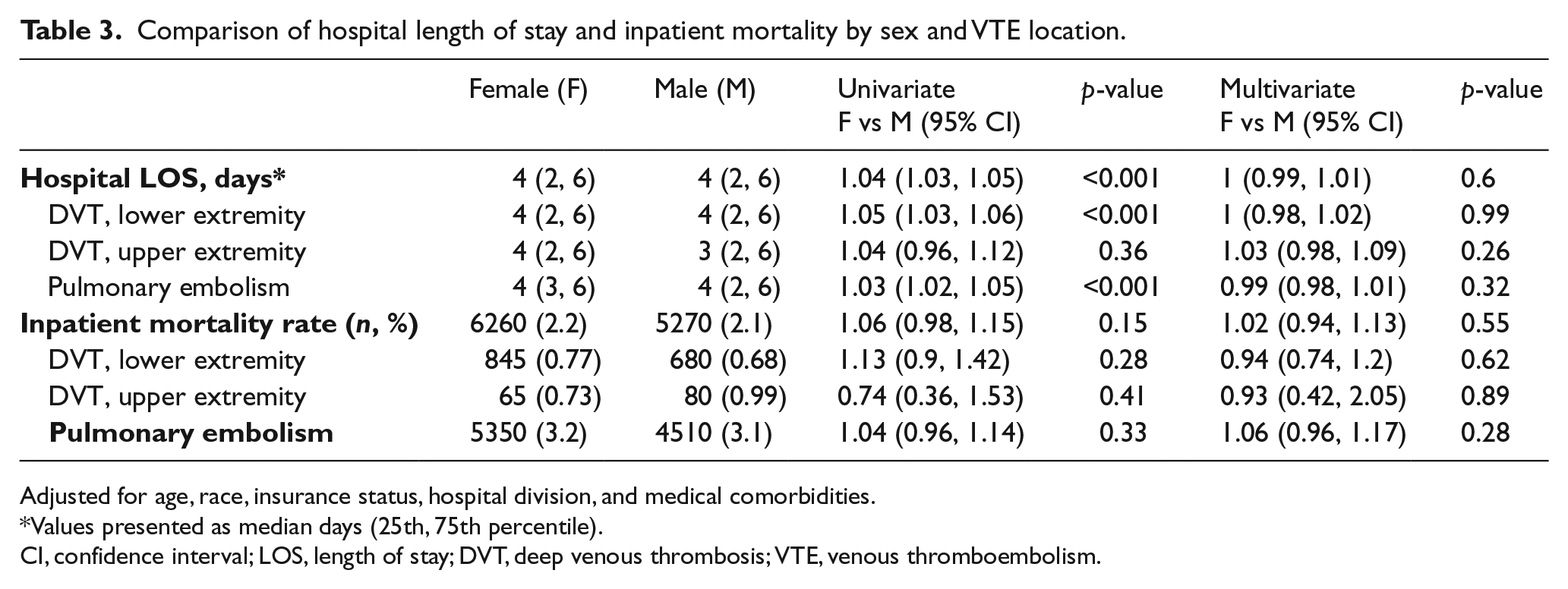
Adjusted for age, race, insurance status, hospital division, and medical comorbidities.
Values presented as median days (25th, 75th percentile).
CI, confidence interval; LOS, length of stay; DVT, deep venous thrombosis; VTE, venous thromboembolism.
Hospital length of stay by VTE location.
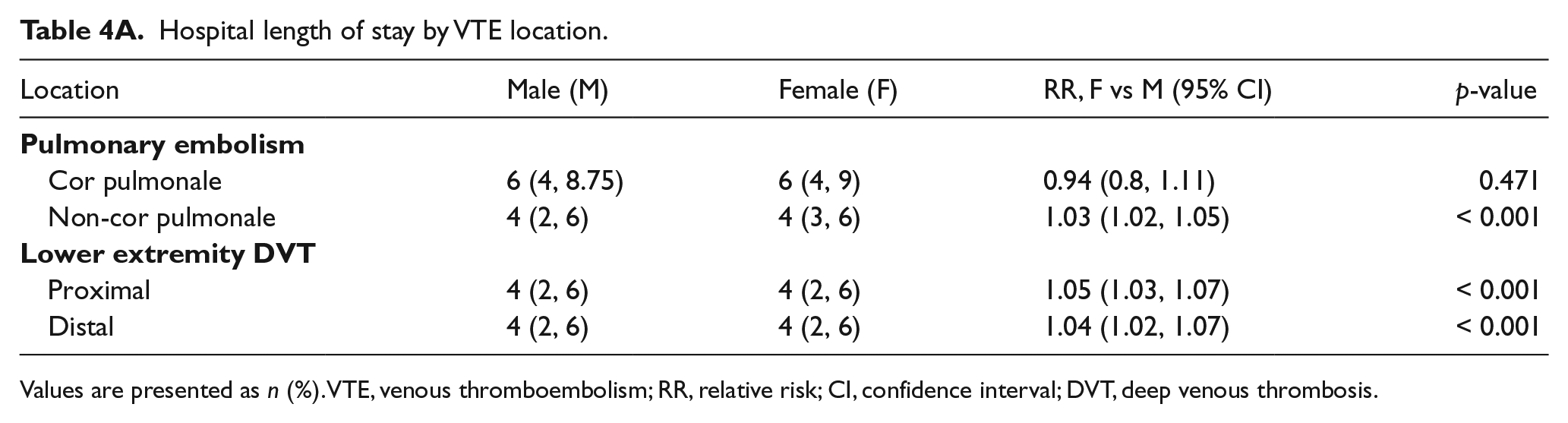
Values are presented as n (%). VTE, venous thromboembolism; RR, relative risk; CI, confidence interval; DVT, deep venous thrombosis.
Inpatient mortality by VTE location.
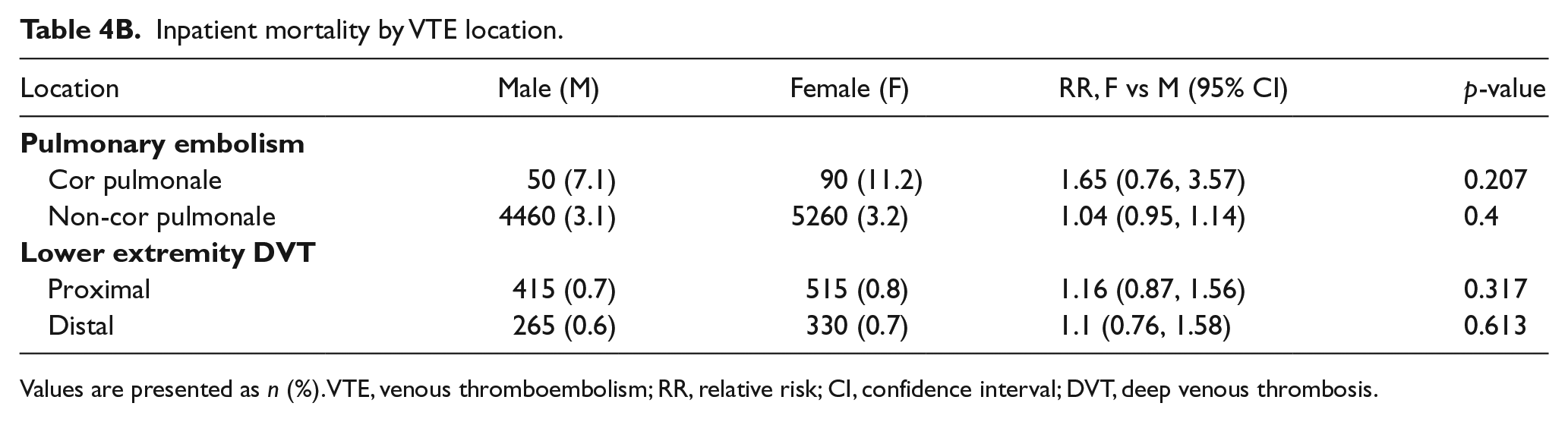
Values are presented as n (%). VTE, venous thromboembolism; RR, relative risk; CI, confidence interval; DVT, deep venous thrombosis.
A total of 2306 patients died in the hospital for a weighted total of 11,530 deaths (2.1% of discharges). Inpatient mortality was similar between the sexes (2.2% for women and 2.1% for men, OR female vs male 1.06, 95% CI 0.98–1.15, p = 0.15). There were no differences in mortality rate between men and women based on location of VTE. Multivariable logistic regression models did not find any differences between men and women after controlling for age, race, insurance status, hospital division, and medical comorbidities. A larger percentage of patients of both sexes with PE associated with cor pulmonale died in hospital compared to those with PE without cor pulmonale, but there were no significant sex-based differences in this regard (Table 4B). There were also no sex-based differences in inpatient mortality between men and women with proximal versus distal lower extremity DVT.
Discussion
We used the NIS database to explore sex-based differences in VTE comorbidities and outcomes. Patients hospitalized between 2012 and 2013 with a primary discharge diagnosis of DVT of the upper or lower extremity or PE showed significant differences between men and women with VTE in terms of baseline clinical characteristics (age, medical comorbidities, and sociodemographic factors). Such characteristics could be explored in further analyses intended to develop sex-based models of risk for VTE. However, despite the significant differences between men and women with respect to VTE presentation, there did not appear to be significant sex-based differences in clinical outcomes in terms of either hospital length of stay or inpatient mortality. While initial results showed a numerically significant increase in hospital LOS in women compared to men, the clinical significance of this finding is uncertain (given that the median hospital LOS remained 4 days in both sexes). Furthermore, after controlling for baseline clinical characteristics, the sex-based difference in hospital LOS was no longer significant. There were no differences between men and women with respect to inpatient mortality in either unadjusted or adjusted analysis.
Though it has been widely reported that male sex is associated with an increased risk of recurrent VTE, the degree of risk appears dependent on the nature of the study. VTE recurrence risk has been reported as two- to threefold higher in men compared to women in observational studies.20,21 However, the magnitude of increased risk appears less pronounced in randomized trials, with many estimating relative risk in the 1.5-fold range.22–27 A recent meta-analysis estimated that the overall risk of VTE recurrence after discontinuing anticoagulation is approximately 50% higher for men than for women. 15 The mechanism of increased recurrence risk is not entirely clear, and may be related to hormonal risk factors. 18 Given the smaller magnitude of increased recurrence risk in men in randomized trials, and the fact that many of these confidence intervals crossed 1.0 (indicating non-significance), our finding that VTE-related outcomes did not appear to differ significantly based on sex is not entirely unexpected. Pathophysiologically, the role of hormonal exposure is less likely to be relevant in the acute management and outcomes of VTE (initial hospitalization and inpatient mortality) and this provides another potential reason why sex-based disparities were not observed. However, there are little comparison data available regarding the role of sex in relation to VTE-related clinical outcomes, and further study is warranted.
Limitations
There are several limitations of this study that we have attempted to address. As with most studies using databases as a patient source, patients were included based on discharge diagnosis, which is subject to error and/or misclassification bias. Such bias may vary based on hospital geographic location and type, and as the data source is particular to the United States, the results may not be as applicable to health systems in other countries. Additionally, though we wished to analyze outcomes for patients who were hospitalized specifically for treatment of DVT or PE, inclusion of data from patients who were hospitalized for non-VTE conditions and developed VTE events while in the hospital is possible. We attempted to minimize this by including only patients with a primary (first) discharge diagnosis of DVT or PE, versus other studies which have included patients with VTE as one of the ‘top three’ discharge diagnoses or as any discharge diagnosis.28,29 The NIS database does not allow for analysis of medication administration either during hospitalization or upon discharge, so it is possible that variations in clinical outcomes may reflect, at least in part, disparities in the medical management of VTE between men and women.
Despite the limitations of the study, we believe it is an important addition to the literature both from the standpoint of thrombosis as well as outcomes research. This is one of the first clinical studies of sex-based disparities in VTE presentation and outcomes, and we believe that these findings are of interest to practitioners, health care researchers, and the public. Given the significant clinical and health care economic impact of VTE, the importance of investigating and reporting factors which both influence and also those which do not impact clinical outcomes of VTE cannot be understated. Venous thromboembolic disease contributes to significant medical morbidity and mortality and has a significant socioeconomic impact on populations throughout the world, and, as such, is it essential to identify disparities in presentation and clinical outcomes as a first step in facilitating interventions that may reduce such disparities and improve outcomes in the overall population. Work such as ours is important in terms of increasing awareness of VTE, which is essential given that global public awareness of VTE appears to be relatively low, especially in relation to other medical conditions. 30 National and international efforts to increase awareness and promote the prevention of VTE, such as the United States Surgeon General’s Call to Action to Prevent Deep Venous Thrombosis and Pulmonary Embolism, are increasingly being promoted as a way to call attention to the importance of VTE.31–33 Studies such as this one will help clinicians and researchers to choose appropriate, clinically meaningful targets for intervention and avoid those targets that may be less meaningful, less cost-effective, and of less clinical utility.
There are several potential avenues for additional investigation which could be considered based on the results of this study. Given that it was not possible to analyze the specific medical regimen used for the management of VTE in this study due to limitations of the NIS data set, sex-based differences in the medical management of VTE could be further evaluated in the context of databases which do include access to prescription-level data. This could also be an opportunity to explore sex-based disparities in the use of direct oral anticoagulants during more recent years, and whether there are sex-based differences in outcome based on the type of treatment chosen for the management of VTE. Additionally, the finding that more men than women underwent thrombectomy for VTE is of interest and may warrant further analysis, particularly with the use of a database containing information regarding thrombolytic administration.
Conclusion
Venous thromboembolic disease is a relatively common condition associated with significant morbidity and mortality. We found that sex did not impact hospital length of stay and mortality in patients hospitalized with acute VTE and therefore a high level of awareness and low threshold to pursue workup is indicated in both sexes. National and international initiatives to increase awareness of VTE and promote VTE prevention are being actively developed and disseminated. Research regarding risk factors which both impact and those which do not impact VTE-related clinical outcomes is necessary so that clinicians can define appropriate targets for intervention and avoid unnecessary or less clinically meaningful interventions.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by small-grant funding from the Mayo Clinic Hematology-Oncology Outcomes Research (HONOR) Group.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.