
Abstract
The prognostic significance of acute pulmonary events in people with lower extremity peripheral artery disease (PAD) is unknown. We hypothesized that an acute pulmonary event (hospitalization for pneumonia and/or chronic lower respiratory disease (CLRD) exacerbation) would be associated with a higher rate of subsequent ischemic heart disease (IHD) events in PAD. A total of 569 PAD participants were systematically identified from among patients in Chicago medical practices and followed longitudinally. Hospitalizations after enrollment were evaluated and adjudicated for pulmonary events. The primary outcome was adjudicated myocardial infarctions, unstable angina, and IHD death. Of 569 PAD participants, 34 (6.0%) were hospitalized for a pulmonary event (11 CLRD exacerbation and 23 pneumonia) during a mean follow-up of 1.52 years±0.80. Participants hospitalized for a pulmonary event had a higher rate of subsequent IHD events than those not hospitalized for a pulmonary event (10/34 (29%) vs 38/535 (7.1%), p<0.001). After adjusting for age, sex, race, comorbidities, and other confounders, a pulmonary hospitalization was associated with an increased risk of a subsequent IHD event (hazard ratio (HR) = 12.42, 95% confidence interval (CI) = 5.35 to 28.86, p<0.001). Non-pulmonary hospitalizations were also associated with IHD events (HR = 3.39, 95% CI = 1.78 to 6.44, p<0.001), but this association was less strong compared to pulmonary hospitalizations and IHD events (p = 0.011 for difference in the strength of association). In conclusion, hospitalization for an acute pulmonary event was associated with higher risk for subsequent IHD events in PAD. Future study should examine whether hospitalization for pulmonary events warrants increased surveillance or potential intervention to prevent IHD events in PAD.
Introduction
Lower extremity peripheral artery disease (PAD) affects eight million people in the United States and nearly 200 million worldwide.1,2 People with PAD have an increased risk of ischemic heart disease (IHD) events compared to people without PAD, even after adjusting for confounders.3,4 Pneumonia and chronic lower respiratory disease (CLRD), prevalent in people with PAD, are associated with an increased risk of IHD or other cardiovascular events in people without PAD.5–9
To our knowledge, the association of either pneumonia or CLRD exacerbation with IHD events has not been studied in people with PAD. Because people with PAD have both a high prevalence of pulmonary disease and high rates of IHD events, they are likely to be vulnerable to complications from pulmonary hospitalizations. We studied the associations of hospitalizations for pulmonary events (CLRD exacerbation or pneumonia) with subsequent IHD event rates among people with PAD identified from outpatient medical centers.
Methods
This study was conducted in the Biomarker Risk Assessment in Vulnerable Outpatients (BRAVO) cohort study. BRAVO was designed to determine whether inflammatory and hemostatic biomarkers increase acutely before an IHD event.10,11 Methods of the BRAVO study have been reported. 10 In the BRAVO study, participants with PAD were enrolled between September 2009 and September 2012 and followed prospectively to identify new IHD events. Participants returned to the medical center every 2 months. At these visits they were interviewed to identify new hospitalizations. Medical records for all hospitalizations after enrollment were obtained and adjudicated by physicians to identify new IHD events and new hospitalizations for pneumonia or CLRD exacerbation. Participants were followed through January 2013.
The Institutional Review Board at Northwestern University and all participating sites approved the protocol. Participants provided written informed consent.
Participants were identified from lists of consecutive men and women diagnosed with PAD in non-invasive vascular laboratories, vascular surgery practices, and other relevant medical practices from six medical centers in Chicago.
The inclusion criterion was presence of PAD – measured by an ankle–brachial index (ABI) < 0.90 at the study visit, evidence of PAD from a medical center-associated non-invasive vascular laboratory, or medical record documented lower extremity revascularization. Exclusion criteria included potential participants with an IHD or cerebrovascular event within the past 6 months, history of inflammatory arthritis, recent cancer diagnosis, or unintentional weight loss. 10 Potential participants who were unable to return for follow-up, with significant communication difficulty or cognitive impairment, or living > 40 miles from the medical center and refusing regular follow-up visits were excluded. Potential participants with recent major surgery and those enrolled in clinical trials were also excluded.
Baseline measures included the ABI, medical history questionnaires, a resting 12-lead electrocardiogram (ECG), and height and weight for calculating body mass index (BMI). Baseline comorbidities were ascertained and confirmed using patient-report, medical record review, medication use, and results of a primary care physician questionnaire. These data were used to verify and adjudicate comorbidities, using comorbidity algorithms developed and validated by the Women’s Health and Aging Study. 12
A hand-held Doppler (Pocket-Dop II; Nicolet Vascular Inc., Golden, CO, USA) was used to measure systolic blood pressures for the ABI measurement after a 5-minute rest. Measured pressures included the brachial, dorsalis pedis, and posterior tibial arteries. Each pressure was measured twice. The ABI was calculated by dividing average systolic pressures in each leg by the average of the brachial pressures.13,14
At baseline and each follow-up visit, ECGs were performed to identify new silent myocardial infarctions.15,16 We used methods and equipment (MAC 1200 portable ECG units; General Electric, Louisville, KY) from the Atherosclerosis Risk in Communities and the Multi-Ethnic Study of Atherosclerosis studies.17,18 Methods from the Cardiovascular Health Study were used to diagnose new silent myocardial infarctions. 19
Participants returned every 2 months for follow-up. At each follow-up, participants underwent an ECG and questionnaire administration. Participants unwilling or unable to attend a follow-up visit received a home visit or follow-up telephone call to obtain information about hospitalizations. Medical records were obtained for new hospitalizations reported after baseline.
The primary outcome was combined fatal and non-fatal IHD events. Non-fatal IHD events were defined as acute myocardial infarction, hospitalizations for unstable angina, and new silent myocardial infarction detected by ECG. Two physician investigators reviewed medical records and independently adjudicated each event. When two primary adjudicators disagreed, a third adjudicator reviewed the case and the outcome was determined by discussion and consensus.
Criteria for myocardial infarction were derived from the Atherosclerosis Risk in Communities and the Multi-Ethnic Study of Atherosclerosis studies.17,18 An acute myocardial infarction required at least two of the following three criteria: (a) chest pain; (b) abnormal ECG consistent with a myocardial infarction (ST segment elevation, new left bundle branch block, new Q waves); and (c) abnormal cardiac enzymes (troponin more than two times the upper limit of normal).
We used criteria from the Multi-Ethnic Study of Atherosclerosis and the Lifestyle Interventions and Independence for Elders (LIFE) Study18,20 to adjudicate unstable angina. Unstable angina was defined as non-elective hospital admission for symptoms of acute angina that is not definite or probable myocardial infarction. Participants were required to have chest pain symptoms attributable to coronary ischemia requiring hospital admission, absence of acute myocardial infarction during the hospital stay, and one or more of the following additional criteria: (a) treatment with nitrates, heparin, or beta-blockers; (b) coronary artery bypass graft surgery or other coronary revascularization during the hospital stay; (c) ⩾70% obstruction of any coronary artery by angiography during the hospital stay; and (d) an ECG showing horizontal or down-sloping ST depression or abnormal ST elevation > 1 mm and these findings were present only during chest pain.
IHD death consisted of definite fatal myocardial infarction, definite coronary heart disease death, and possible coronary heart disease death. 18
Participants with new Q waves on their ECG during follow-up, consistent with a new myocardial infarction, were also classified as having a new IHD event. Two board-certified cardiologists reviewed each ECG to identify new Q waves. Discrepancies were resolved by discussion.
We used methods from the LIFE Study to adjudicate pulmonary events. 20 Criteria for hospitalization for acute CLRD required all three of the following criteria: (a) history of CLRD at the time of hospital admission; (b) hospitalization for dyspnea, increased cough, or sputum production; and (c) treatment with inhalers or steroids for respiratory symptoms. Criteria for hospitalization for pneumonia required all of the following criteria: (a) hospitalization with cough or fever; (b) a new infiltrate or effusion on chest X-ray; and (c) treatment with an antibiotic.
Hospitalizations for reasons that did not meet criteria for a pulmonary event were classified as non-pulmonary hospitalizations. Non-pulmonary hospitalizations excluded hospitalizations for the primary outcome of IHD events. Hospitalizations primarily for infections that did not meet criteria for hospitalization for pneumonia were classified as hospitalizations for infections other than pneumonia.
The six-minute walk test was performed at baseline using a standardized and well-validated protocol.21,22 Participants walked up and down a 100-foot (30.48 m) hallway for 6 minutes after instructions to cover as much distance as possible.
Participants brought their medications to their baseline visit. A study investigator (MMM) classified medications according to whether they were statins, anti-platelet drugs, or inhaled pulmonary drugs (inhaled corticosteroids, inhaled anti-cholinergic drugs, and inhaled bronchodilators).
Statistical analyses
Baseline characteristics were compared between those with and without pulmonary hospitalizations using t-tests for continuous measures and chi-squared tests for discrete measures.
Cox regression analyses with the hospitalization status as a time-dependent binary covariate were used to evaluate the association of hospitalization for pulmonary events with subsequent IHD events, adjusting for age, sex, race, comorbidities (baseline prevalence of myocardial infarction, angina, heart failure, stroke, CLRD, cancer, and diabetes), BMI, medications, and smoking. Analyses were repeated separately for pneumonia and CLRD exacerbation, respectively. Eleven hospitalizations that were adjudicated as both acute CLRD and acute pneumonia were classified as pneumonia when CLRD and pneumonia were analyzed separately.
Similar Cox regression analyses with the hospitalization status as a time-dependent binary covariate were used to evaluate the associations of non-pulmonary hospitalizations and hospitalizations due to infections other than pneumonia, respectively, with subsequent IHD events, adjusting for age, sex, race, comorbidities, BMI, smoking, and relevant cardiovascular and pulmonary medications. Analyses were repeated with additional adjustment for the six-minute walk test, to determine whether six-minute walk performance attenuated the association of hospitalization for acute pulmonary events with subsequent IHD events.
Some PAD participants were eligible based on medical record documented prior lower extremity revascularization and had a normal ABI at their study visit. Therefore, to determine whether the association of pulmonary hospitalizations with IHD events was independent of the ABI, analyses were repeated in the subset of participants with an ABI < 0.90, adjusting for age, sex, race, BMI, comorbidities, ABI, smoking, and pulmonary and cardiovascular medications.
Time-dependent Cox modeling was used to determine whether hospitalization for an acute pulmonary event was a stronger predictor than a hospitalization for a non-pulmonary event and hospitalization for an infection other than pneumonia, respectively, in predicting subsequent IHD events. These analyses adjusted for age, sex, race, BMI, comorbidities, smoking, and cardiovascular and pulmonary medications.
Results
A baseline visit was scheduled for 950 participants, but 131 met exclusion criteria and 224 did not attend their appointments or refused participation. Of the 595 participants enrolled, 15 were lost to follow-up and 11 participants were excluded due to missing covariates, leaving 569 participants for analysis. Mean follow-up was 1.52 years ± 0.80. Forty-eight participants (8.4%) had one or more IHD events during follow-up. Among participants who had a pulmonary event followed by an IHD, the median time between hospitalization for the pulmonary event and the IHD event was 59.5 days. The first IHD events experienced by these 48 participants were eight cardiac deaths, 22 hospitalizations for acute myocardial infarction, 15 hospitalizations for unstable angina, one hospitalization for a resuscitated cardiac arrest and two silent myocardial infarctions. Two hospitalizations were adjudicated as attributable to both IHD events and pulmonary events. These hospitalizations were counted as IHD events preceded by pulmonary events. Results were not meaningfully changed when these two hospitalizations were excluded from analyses (data not shown).
Thirty-four participants (6%) were hospitalized for one or more acute pulmonary events during follow-up. Of these, 23 (68%) were hospitalized for pneumonia and 11 (32%) for CLRD. PAD participants hospitalized for pulmonary disease were older and had a higher baseline prevalence of CLRD compared to those not hospitalized for pulmonary events (Table 1). A total of 198 PAD participants (34.8%) experienced a non-pulmonary hospitalization. Fifty-seven PAD participants (10%) were hospitalized for an infection other than pneumonia.
Baseline characteristics of peripheral artery disease participants with and without hospitalization for an acute pulmonary event during follow-up.
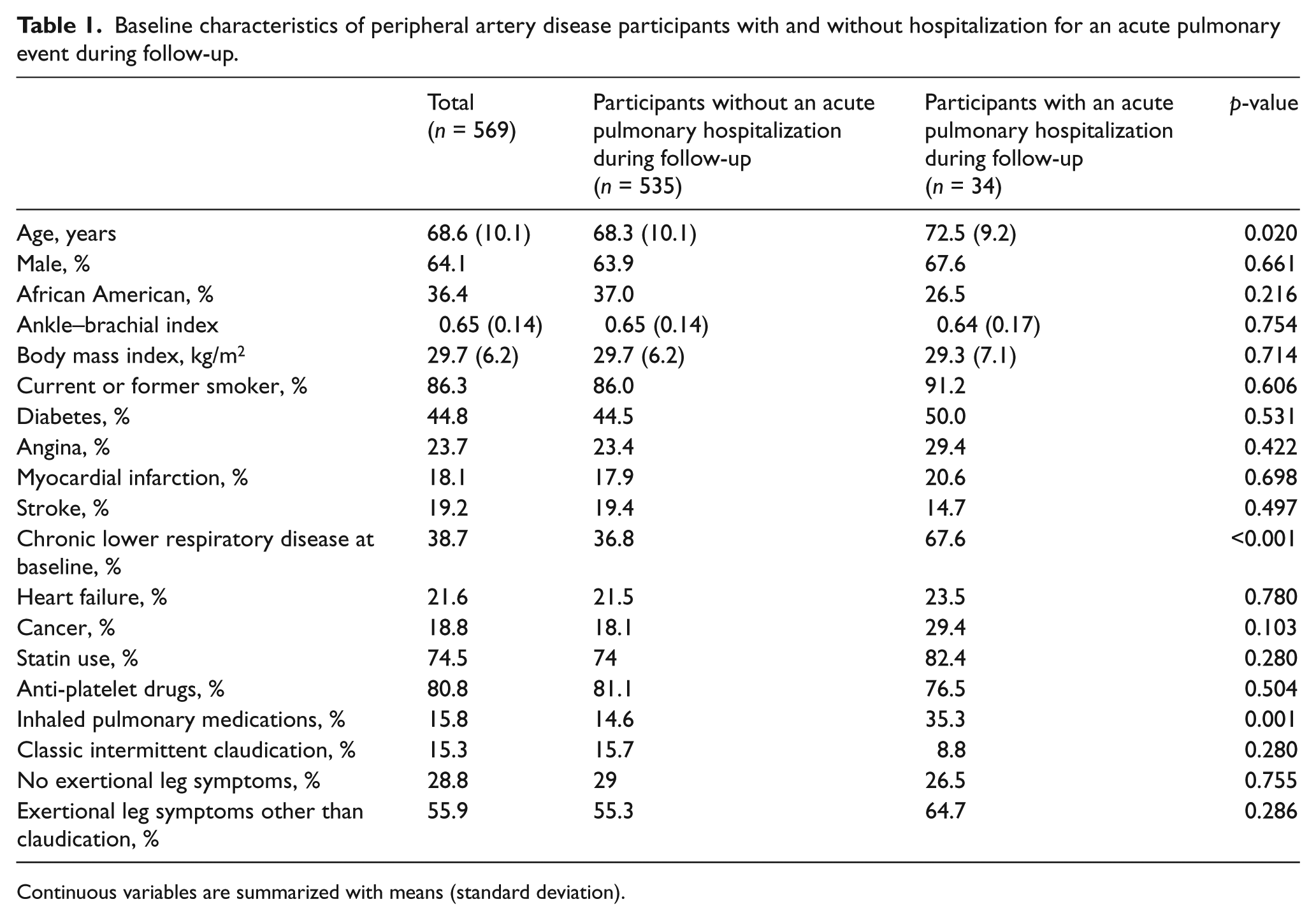
Continuous variables are summarized with means (standard deviation).
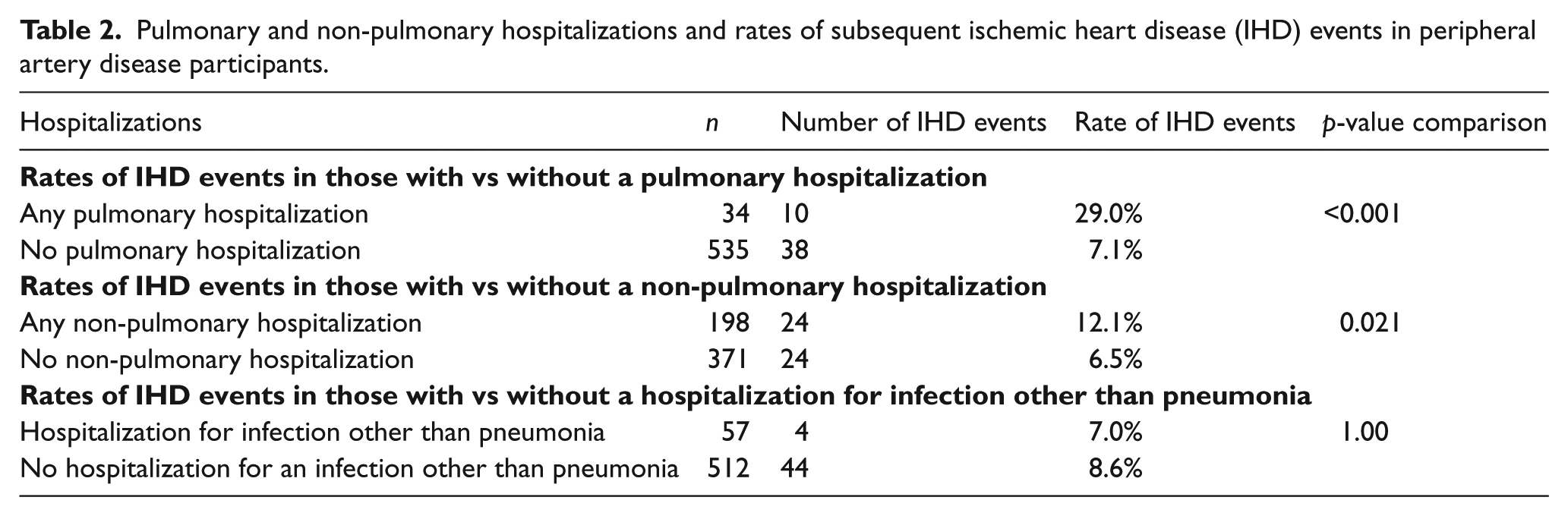
IHD events were more common in PAD participants hospitalized for a pulmonary event, compared to those not hospitalized for a pulmonary event: 10/34 (29%) of PAD participants hospitalized for an acute pulmonary event experienced a subsequent IHD event versus 38/535 (7.1%) of PAD participants not hospitalized for an acute pulmonary event (p<0.001) (Table 2). IHD events were also more common in PAD participants hospitalized for a non-pulmonary reason compared to those not hospitalized for a non-pulmonary reason (p=0.021) (Table 2). However, there were no differences in rates of IHD events among PAD participants hospitalized for an infection other than pneumonia compared to those not hospitalized for a pneumonia infection (p=1.00) (Table 2).
Pulmonary and non-pulmonary hospitalizations and rates of subsequent ischemic heart disease (IHD) events in peripheral artery disease participants.
Adjusting for age, sex, race, smoking, BMI, comorbidities, and medications, participants hospitalized for an acute pulmonary event had higher rates of a subsequent IHD event than those not hospitalized for an acute pulmonary event (hazard ratio (HR)=12.42, 95% confidence interval (CI)=5.35 to 28.86, p<0.0001). Adjusted HRs for associations of hospitalization for pneumonia or an acute CLRD exacerbation, respectively, with an acute IHD were similar to the adjusted HRs for associations of all pulmonary hospitalizations with subsequent IHD events (HR=10.84, 95% CI=3.93 to 29.9, p<0.001 and HR=10.82, 95% CI=3.01 to 38.9, p<0.001, respectively). Acute pulmonary hospitalizations were associated independently with both unstable angina (HR=5.99, 95% CI=1.10 to 32.51, p=0.038) and myocardial infarction (HR=20.68, 95% CI=6.24 to 68.56, p<0.001) in adjusted analyses. Adjusting for age, sex, race, smoking, BMI, comorbidities, and medications, non-pulmonary hospitalizations (HR=3.39, 95% CI=1.78 to 6.44) but not hospitalizations for infections other than pneumonia (HR=1.15, 95% CI=0.39 to 3.38) were associated with an increased risk of subsequent IHD events (Table 3).
Clinical characteristics associated with ischemic heart disease (IHD) events in people with peripheral artery disease (n=569).
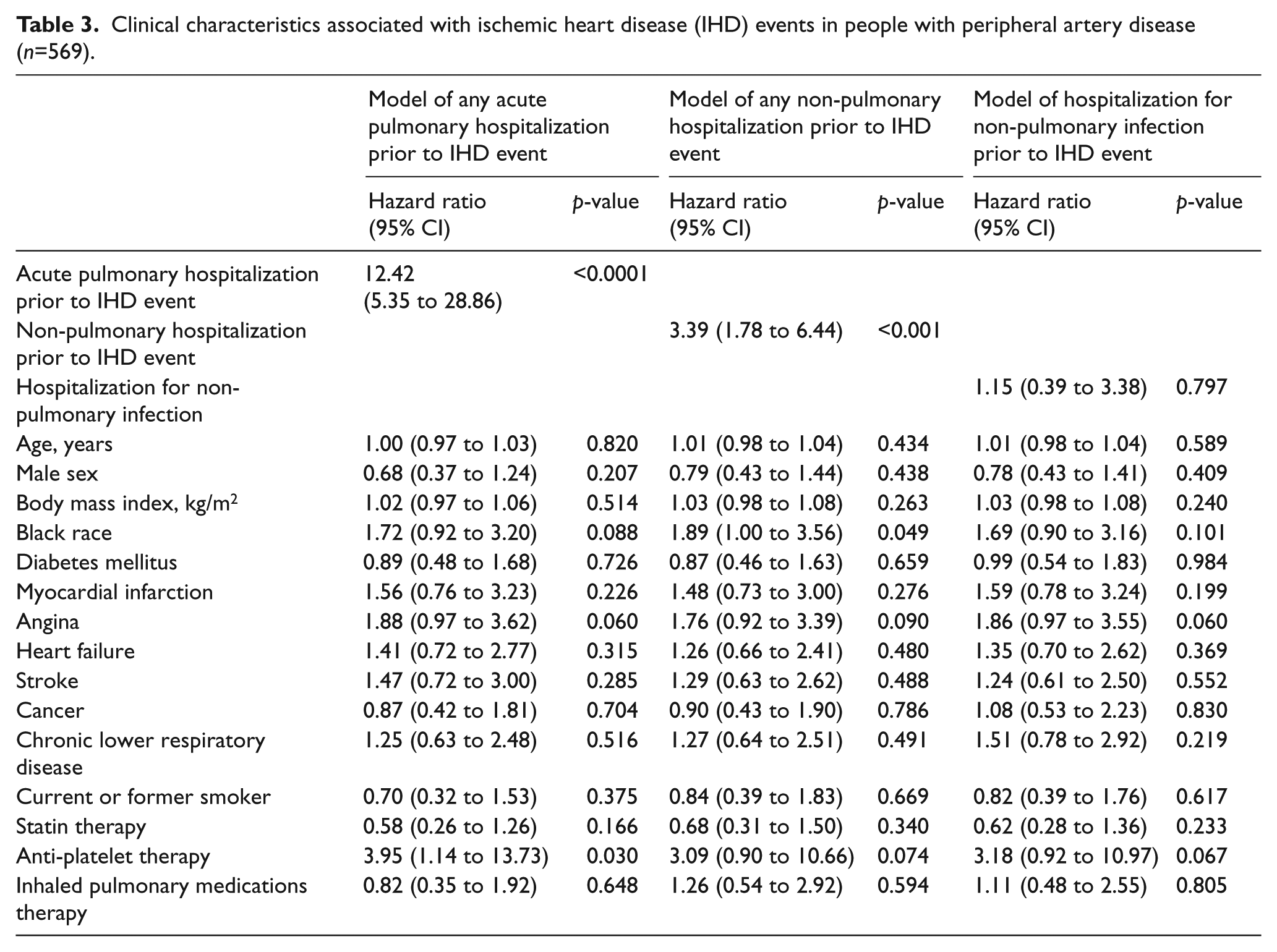
Table 3 shows hazard ratios for all covariates in the Cox proportional hazards analyses relating pulmonary hospitalizations, non-pulmonary hospitalizations, and hospitalizations for non-pulmonary infections, respectively, to IHD events. For the model evaluating the independent association of pulmonary hospitalizations with subsequent IHD events, use of anti-platelet therapy was also associated independently with subsequent IHD events. For the model evaluating all non-pulmonary hospitalizations, black race was associated with an increased risk of IHD events (Table 3).
In sensitivity analyses, we repeated analyses among the 406 PAD participants with an ABI < 0.90 at baseline, excluding those who were eligible based on prior lower extremity revascularization or non-invasive vascular laboratory evidence of PAD. Among participants with an ABI < 0.90 at baseline, the HR for the association of acute pulmonary hospitalizations with subsequent IHD events was 24.79 (95% CI=8.75 to 70.22, p <0.001), adjusting for age, sex, race, BMI, smoking, comorbidities, and relevant pulmonary and cardiovascular medications. This HR was not substantially changed after additional adjustment for the ABI (HR=24.16 (95% CI= 8.63 to 67.59, p<0.001)). We also repeated analyses among the 510 PAD participants with baseline six-minute walk data. In these participants, the HR for the association of acute pulmonary hospitalizations with subsequent IHD events was 11.30 (95% CI=14.48 to 28.55, p <0.001), adjusting for age, sex, race, BMI, smoking, comorbidities, and relevant pulmonary and cardiovascular medications. This HR was not substantially changed after additional adjustment for the six-minute walk (HR=9.28 (95% CI=3.64 to 23.63, p<0.001)).
In Cox proportional hazards analyses, the HR for the association of acute pulmonary hospitalizations with subsequent risk of IHD events was significantly higher than the HR for the association of non-pulmonary hospitalizations and hospitalizations for infections other than pneumonia with subsequent IHD events, adjusting for age, sex, race, BMI, comorbidities, smoking, and cardiovascular and pulmonary medications (Table 4).
Relative associations of pulmonary hospitalizations, non-pulmonary hospitalizations, and hospitalizations for infections with ischemic heart disease (IHD) events in people with peripheral artery disease (n=569).
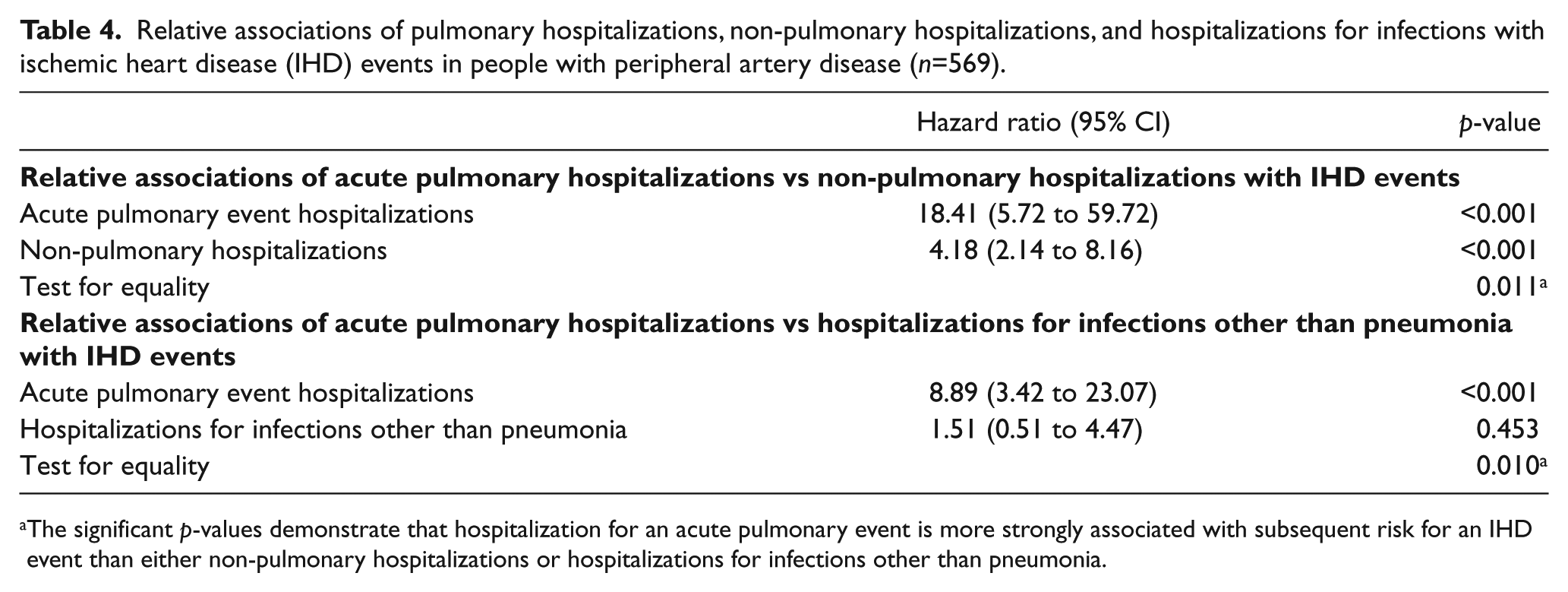
The significant p-values demonstrate that hospitalization for an acute pulmonary event is more strongly associated with subsequent risk for an IHD event than either non-pulmonary hospitalizations or hospitalizations for infections other than pneumonia.
Discussion
Among 569 PAD participants, hospitalization for an acute pulmonary event was associated with more than a 10-fold increased risk of a subsequent IHD event, even after adjusting for potential confounders. The strength of the association of pulmonary event hospitalization with subsequent IHD events was comparable for pneumonia and acute exacerbation of CLRD, when each was considered individually. Pulmonary hospitalization was associated significantly with both unstable angina and myocardial infarction, respectively.
Although PAD participants with a history of CLRD at baseline did not have higher rates of IHD events than PAD participants without CLRD at baseline, PAD participants with a pulmonary hospitalization during their study participation had a markedly higher rate of IHD events during follow-up compared to those without a pulmonary hospitalization. The distinction between the prognostic significance of a baseline medical history of CLRD versus hospitalization for an acute pulmonary event may help elucidate mechanisms for the findings reported here. It is possible that hypoxia, tachycardia and acute inflammation associated with acute hospitalizations for pulmonary disease may serve as a trigger for subsequent IHD events. The relatively short period of follow-up supports the hypothesis that acute hypoxia, tachycardia, and inflammation may be short-term triggers for IHD events. In contrast, patients with CLRD who are not hospitalized for acute pulmonary events may be at lower risk because of the absence of these potentially contributing factors.
Among PAD participants, we also observed that hospitalization for any reason other than an acute pulmonary event was associated with increased risk of subsequent IHD events, compared to PAD participants without hospitalization. However, the association of hospitalization for an acute pulmonary event was significantly stronger than the association of hospitalization for non-pulmonary reasons with subsequent IHD events. Furthermore, hospitalization for an infection other than pneumonia was not associated with a higher rate of subsequent IHD events. Together, these results support the hypothesis that hospitalization for an acute pulmonary event identifies PAD patients at particularly high risk for a subsequent IHD event.
A study of 5888 community dwelling men and women from the Cardiovascular Health Study and 15,792 participants in the Atherosclerosis Risk in Communities Study reported that participants hospitalized for pneumonia had a higher rate of subsequent cardiovascular events. 5 Associations of hospitalization for pneumonia with subsequent cardiovascular events were highest during the first 30 days after pneumonia hospitalization and decreased with increasing time. For example, in the Cardiovascular Health Study, the HR=4.07 (95% CI=2.86 to 5.27) during the first 30 days of follow-up and decreased to HR=2.10 (95% CI=1.59 to 2.60) between 91 and 365 days of follow-up. 5 In the Rotterdam study of community dwelling people, a history of CLRD was associated with an increased risk of sudden cardiac death (age and sex-adjusted HR=1.34, 95% CI=1.06 to 1.70). Participants with frequent chronic obstructive pulmonary disease (COPD) exacerbations had a 3.58 HR (95% CI=2.35 to 5.44) for the association with sudden cardiac death, suggesting that more severe COPD is associated with greater risk of cardiac death. 9 Among participants with PAD, we observed hazard ratios that were substantially higher than those observed in these community dwelling populations. This may be related to illness acuity, including the severity of pulmonary disease, among PAD patients and the higher risk of cardiovascular events in people with PAD.
Mechanisms of associations of pulmonary disease with subsequent cardiovascular disease events are unclear. However, among people with pneumonia, elevated levels of inflammatory and hemostatic biomarkers can persist after pneumonia and may contribute to subsequent cardiovascular risk.23–25 Among people with chronic airway disease, inflammation, hypoxemia, and autonomic dysfunction, including tachycardia, might all be potential mechanisms explaining the association of COPD with subsequent IHD events. Increased arterial stiffness in patients hospitalized for a pulmonary event may denote patients at increased risk for subsequent IHD events. Importantly, the magnitude of associations of hospitalization for pneumonia and acute CLRD were comparable, suggesting that biologic pathways unique to both types of acute pulmonary events may contribute to the higher rate of IHD event.
Limitations
Our study has limitations. First, we adjudicated pneumonia and acute CLRD outcomes only among those who were hospitalized. Our study design did not allow us to evaluate associations of pneumonia or CLRD exacerbations treated in the outpatient setting with subsequent risk of IHD events. Second, the follow-up of our study was relatively short. Third, the numbers of pulmonary hospitalizations and IHD events were relatively small. Fourth, our study design does not allow us to assess potential mechanisms by which pulmonary hospitalizations are associated with subsequent IHD events. Fifth, the BRAVO study is an observational study. We cannot discern from our data whether the associations reported here are causal. Sixth, we did not collect data on chronic renal insufficiency or anemia.
Conclusion
In conclusion, acute pulmonary hospitalizations were associated with a higher rate of subsequent IHD events in people with PAD. This association was stronger than the association of non-pulmonary hospitalizations with subsequent IHD events. Identifying mechanisms of the associations reported here could lead to new therapeutic targets for preventing IHD events in people with PAD. Future studies should consider whether close monitoring for and early treatment of pulmonary events may prevent IHD events in people with PAD. Future studies should also consider whether vaccinating with the protein conjugate pneumococcal vaccine and maximizing the influenza vaccination may prevent IHD events in people with PAD.26,27
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: funded by the National Heart, Lung, and Blood Institute (NHLBI), R01-HL089619 and R01-HL109244. The funding agency played no role in carrying out the study, data analyses, data interpretation, or manuscript writing.