
Abstract

Introduction
Leg swelling, known as edema, is a common problem, representing more than half of new referrals to a large vascular medicine practice. Edema occurs when fluid builds up in the tissues, and it may happen suddenly or develop slowly and last for months or years. Most frequently edema is a result of harmless conditions, but occasionally it is caused by more serious underlying health problems.
When thinking about the causes of leg edema, it is helpful to divide them into causes involving both legs versus involving just one leg, as some conditions may cause swelling in one or both legs. Often, the most important clues to the cause of leg edema are in the patient’s reported history and in the physical examination, and a doctor may not need blood work or any other tests to make a diagnosis.
Edema of both legs
Dependent edema is probably the most common form of swelling in both legs referred to vascular doctors. This type of swelling develops when a patient sits or stands for prolonged periods. The veins are the blood vessels that drain blood from the arms and legs back to the heart, and they are thin-walled and stretchy. Whereas the blood in the arteries is propelled by the pumping heart, the veins in the legs must work against gravity. Thus, blood can pool in the leg veins and lead to swelling.
One way the body assists the veins is with calf muscle contraction with walking, known as the ‘calf muscle pump’. Patients who are inactive (sedentary) for long periods may have leg edema because the calf muscle pump is underused or ineffective. Elevating the ankles above the level of the heart can help relieve this type of swelling. Most patients with dependent edema notice that their swelling is vastly improved first thing in the morning, unless they sleep in a recliner or other furniture that keeps their legs below the level of the heart. Patients with dependent edema are often prescribed elastic compression stockings to help prevent the swelling from reaccumulating when they are seated or standing during the day.
Similarly, obesity can cause or contribute to dependent edema, as the veins do not drain as effectively because of added weight pressing on them in the belly. Pregnancy may also lead to dependent edema, both because of added weight in the belly and because of hormonal changes. Swelling of the legs during pregnancy generally goes away after childbirth. Hormonal changes related to the menstrual cycle can also cause mild edema in both legs.
Disorders of the endocrine (hormone or gland) system can occasionally cause edema. A severely over- or underactive thyroid gland may cause swelling or thickening of the skin on the lower legs (shins) that is often hard and waxy-appearing. Cushing’s syndrome, a disorder in which the adrenal gland produces too much steroid hormone, may also cause swelling in both legs. In addition to swelling, patients with Cushing’s syndrome usually have other features of the condition such as skin changes, roundness of the face, and development of a hump of tissue at the back of the neck.
Patients with congestive heart failure may have swelling of both legs when a weakened heart cannot pump enough blood forward. When this happens, blood backs up in the veins and leads to an increase in pressure that pushes fluid into the tissues. Patients with heart failure have other symptoms in addition to swelling, most commonly shortness of breath with physical exertion or when lying flat. Conditions of the kidneys and liver sometimes cause swelling as well, so patients who come to their doctor with new swelling in both legs usually have evaluation of these organs with simple blood and/or urine tests.
Medications are a common cause of swelling in both legs. Swelling can be seen with calcium-channel blockers (such as amlodipine or nifedipine), non-steroidal anti-inflammatory drugs (NSAIDs, such as ibuprofen or naproxen), gabapentin, hormones (such as oral contraceptives), prednisone, diabetes medications called the thiazolidinediones (such as pioglitazone or rosiglitazone), and many others.
Occasionally, patients may have swelling of both legs because of severe malnutrition. These patients do not have enough protein in the bloodstream, which allows fluid to leak into the tissues. Patients who are extremely ill in the hospital often develop swelling in the legs and sometimes in the arms because of changes that occur with severe illness. This type of diffuse swelling, which is called anasarca, will resolve over time as the patient’s general condition improves.
Edema of one leg
Deep vein thrombosis (DVT), or a blood clot in the large veins in the thigh or calf, usually results in swelling of just one leg (Figure 1). Rarely, when the large vein that goes from the pelvis to the heart is blocked (known as the inferior vena cava or IVC), both legs can swell. Swelling develops over hours to days, and the patient usually also has pain and redness of the leg. DVT is caused by a combination of stagnant blood flow, injury to veins, and conditions that cause clotting. DVT is most often seen in patients who have had major surgery, have had trauma (especially leg trauma), have been hospitalized for more than 3 days, or have cancer. Diagnosis of DVT is made using ultrasound, a non-invasive test performed in radiology or the vascular laboratory. Anticoagulant medications, or blood thinners, are used to treat the DVT. As the body slowly dissolves the blood clot, the leg swelling improves.

This patient has a deep vein thrombosis (DVT or blood clot) in the right leg, which is swollen and darkened compared with the more normal-appearing left leg.
Superficial thrombophlebitis or superficial vein thrombosis (blood clots in the surface veins) may also cause swelling of one leg. With a superficial blood clot, patients usually have pain, redness, and tenderness to touch at the affected vein, which sometimes can be felt as a hard knot or cord in the leg. The diagnosis is often clear from the patient’s history and physical examination, though usually the doctor will order an ultrasound. Treatment consists of anti-inflammatory medications and warm compresses applied to the affected area, unless the clot extends through a long portion of the vein or close to a deep vein, when blood thinners may be prescribed.
Several conditions that mimic blood clots can cause swelling, pain, and redness in one leg. Cellulitis is an infection of the soft tissues of the leg, seen more frequently in patients with diabetes and other chronic medical conditions, though it can also occur in healthy people if a cut or abrasion allows bacteria to enter the tissue. Cellulitis is treated with antibiotics. Ruptured Baker’s cysts and calf muscle tears can also cause swelling, pain, and redness of one leg. A Baker’s (or popliteal) cyst occurs when the lining of the knee joint pouches out behind the knee; it can cause a feeling of fullness or pain in the crease behind the knee, with or without leg swelling. Sometimes these cysts, which are harmless, can burst with physical activity and cause extensive swelling throughout the calf and ankle. Calf muscle tears can occur with strenuous activity, especially jumping. In both Baker’s cyst rupture and calf muscle tear, a crescent-shaped bruise may be seen at the inner or outer ankle, tracking into the side of the foot. Ruptured Baker’s cysts are treated with rest, elevation, and icing the affected leg. Calf muscle tears may be treated with immobilization of the leg in a walking boot or a cast.
Edema of one or both legs
Several vascular disorders can result in swelling of one or both legs. Chronic vein problems may lead to a phenomenon called venous hypertension. Venous hypertension occurs when veins become enlarged and the valves that prevent the backward flow of blood can no longer close properly, allowing blood to fall backward in the leg. The excess blood leads to high pressure in the veins, which in turn causes fluid to leak into the tissues. This problem is also known as chronic venous insufficiency. Patients with venous hypertension may have varicose veins, which are enlarged, bulging, twisted, rope-like veins; or spider veins, small bluish-purple veins that sprout on the ankles, calves, or thighs (Figure 2).

Small spider veins on the ankle and calf are signs of underlying venous hypertension and chronic venous insufficiency. This patient also had ‘dependent edema’ from standing for long periods during the day. The ridged appearance on the legs is from compression bandages, which have squeezed much of the excess fluid out of the leg.
Venous hypertension can also occur when a patient has had a past blood clot (DVT) in the leg veins, damaging the valves or causing persistent blockage of blood flow back toward the heart, a condition known as the post-thrombotic syndrome (PTS). In both varicose veins and the PTS, the legs may be achy or painful, especially with prolonged sitting or standing, and patients may have night-time symptoms like leg muscle cramps or restless legs. In severe cases of venous hypertension, patients have skin changes that include brown or purple darkening or staining (hyperpigmentation) around the lower parts of the legs, hardening or thinning of the skin on the legs, or painful sores that occur with minor injury or sometimes even with no injury.
Varicose veins and the PTS are usually treated with compression stockings to control swelling, and for certain patients there are outpatient procedures that are aimed at destroying or removing damaged veins or reopening persistently blocked veins. Patients who develop sores in the setting of venous hypertension need advanced wound care, as these sores are slow to heal.
Lymphedema is another vascular cause of swelling that can affect one or both legs (Figure 3). The lymphatic vessels are tiny channels in the skin that sweep up excess fluid that gets trapped in the tissues, and that are involved in the body’s infection-fighting functions. The lymphatic vessels drain to the lymph nodes, tiny (less than half an inch) organs that filter the fluid and where some infection-fighting white blood cells are formed. When lymphatic vessels are injured, or when lymph nodes are removed surgically (as with some cancer surgeries), patients may develop lymphedema, a painless, rubbery swelling of the legs that also involves the top of the foot and the toes. Some patients are born with incomplete or underdeveloped lymphatic vessels, and they may develop lymphedema with no explanation, usually in the teenage years or in the mid-30s. Other common causes of lymphedema include severe obesity and chronic venous insufficiency. Lymphedema is almost always diagnosed by taking the patient’s history and on physical examination. If the diagnosis is not clear, specialized imaging tests in a hospital’s nuclear medicine laboratory may be performed. Lymphedema is treated with a special kind of physical therapy (called manual lymphatic drainage) that involves light-pressure massage and wrapping with elastic bandages to shrink the leg before fitting for a compression stocking or garment. Lymphedema is incurable, and patients will reaccumulate fluid in the legs if they do not always wear a compression garment or bandages.

(A) Leg swelling due to mild lymphedema. This patient also has redness and pain due to cellulitis, a soft tissue infection. (B) Severe lymphedema. This patient has a severely swollen leg, puffiness of the foot, squaring of the toes, and creases at the bases of the toes. This patient also has wart-like overgrowth of the tissues on the inner aspect of the leg and at the toes, which can occur with severe lymphedema.
Conclusion
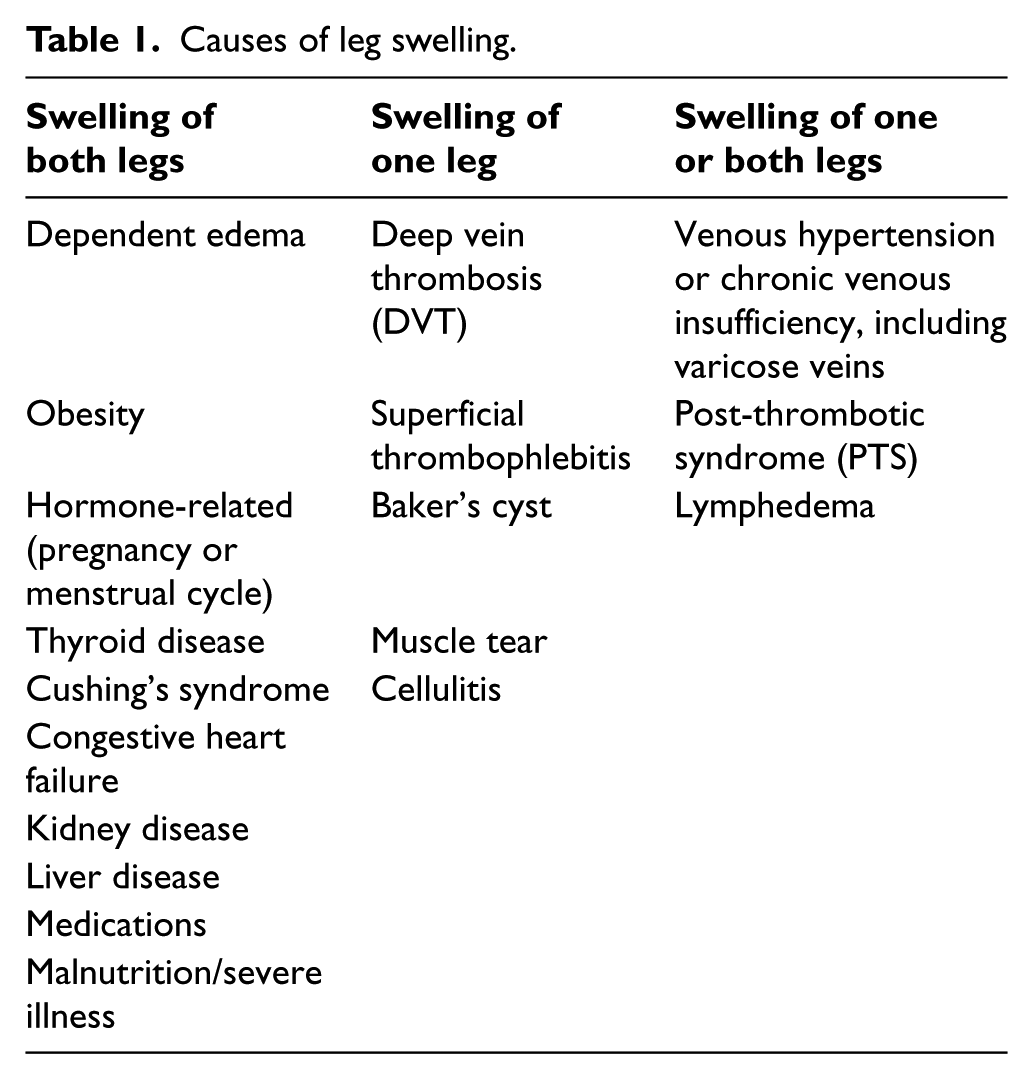
Leg swelling (edema) is common and may be caused by a wide variety of disorders, some harmless, some more serious. Diagnosis of the underlying condition is often made by history and physical examination, although sometimes blood work and imaging tests may be done. Treatment of leg swelling depends on the underlying cause. A summary of the causes of leg swelling is given in Table 1.
Causes of leg swelling.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.