
Abstract
Long-term right ventricular (RV) function, functional capacity, exercise capacity, and quality of life following pulmonary embolism (PE), and the impact of thrombolysis, are unclear. A systematic review of studies that evaluated these outcomes with ⩾ 3-month mean follow-up after PE diagnosis was performed. For each outcome, random effects meta-analyses were performed. Twenty-six studies (3671 patients) with 18-month median follow-up were included. The pooled prevalence of RV dysfunction was 18.1%. Patients treated with thrombolysis had a lower, but not statistically significant, risk of RV dysfunction versus those treated with anticoagulation (odds ratio: 0.51, 95% CI: 0.24 to 1.13, p=0.10). Pooled prevalence of at least mild functional impairment (NYHA II–IV) was 33.2%, and at least moderate functional impairment (NYHA III–IV) was 11.3%. Patients treated with thrombolysis had a lower, but not statistically significant, risk of at least moderate functional impairment versus those treated with anticoagulation (odds ratio: 0.48, 95% CI: 0.15 to 1.49, p=0.20). Pooled 6-minute walk distance was 415 m (95% CI: 372 to 458 m), SF-36 Physical Component Score was 44.8 (95% CI: 43 to 46), and Pulmonary Embolism Quality of Life (QoL) Questionnaire total score was 9.1. Main limitations included heterogeneity among studies for many outcomes, variation in the completeness of data reported, and inclusion of data from non-randomized, non-controlled, and retrospective studies. Persistent RV dysfunction, impaired functional status, diminished exercise capacity, and reduced QoL are common in PE survivors. The effect of thrombolysis on RV function and functional status remains unclear.
Introduction
Chronic thromboembolic pulmonary hypertension, diagnosed when a patient has residual pulmonary artery obstruction and a mean pulmonary artery pressure greater than 25 mmHg with a normal wedge pressure, is thought to occur in 4% of survivors of a first-time symptomatic pulmonary embolism (PE). 1 However, there is evidence that many more have some combination of poor quality of life (QoL) and exercise intolerance following PE, a constellation that some have termed the ‘post-PE syndrome’, analogous to the post-thrombotic syndrome following deep vein thrombosis (DVT).2,3 These symptoms appear to occur in spite of systemic anticoagulation, and may be attributed to unresolved thrombus and right ventricular (RV) damage causing abnormal right heart pressures, either at rest or during exercise in the months to years following PE.
Given that PE is the third leading cause of cardiovascular death in the United States, 4 most clinical research has focused on preventing short-term mortality and clinical deterioration in at-risk subgroups, and numerous meta-analyses have characterized these short-term outcomes. A smaller number of studies have examined long-term outcomes following PE, and, to date, no systematic review or meta-analysis has analyzed this literature. The purpose of this systematic review and meta-analysis was to characterize the persistent effects of PE on RV function, functional capacity, exercise tolerance, and quality of life (QoL), and to assess whether thrombolytic drugs affect these outcomes.
Methods
References
The study was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 5 MEDLINE and EMBASE databases were searched for randomized or non-randomized controlled studies and prospective or retrospective case series published in English-language journals between January 2000 and March 2016 that reported on RV function, functional capacity, or QoL at least 3 months after PE diagnosis. The details of the MEDLINE search strategy are listed in Supplementary Table 1. The syntax for EMBASE was similar, but adapted as necessary. Additionally, manual searches were conducted using the Directory of Open Access Journals, Google Scholar, and the reference lists of included papers and relevant meta-analyses.
Study selection
Study selection was performed by two independent reviewers. Study selection discrepancies between the reviewers were resolved by consensus. Titles and abstracts were initially screened to exclude non-English manuscripts, review articles, commentaries, letters, case reports, and obvious irrelevant studies. Full-texts of the remaining articles were retrieved and reviewed. Studies were excluded if the sample size was less than 20, patients were treated exclusively by pulmonary embolectomy, outcomes of interest were not reported or were not calculable, mean patient follow-up was less than 3 months, or a kin relationship was identified (multiple publications reporting identical outcomes in the same or overlapping series of patients). In these instances, only the manuscript with the largest sample size was included.
Data extraction
An initial database was developed, pilot-tested, and refined to ensure consistency with outcomes reported in the literature. Data were independently extracted from eligible articles by two reviewers. Data extraction discrepancies between the reviewers were resolved by consensus. The types of data recorded in the standardized data extraction forms included general manuscript information, study design, risk of bias using the Newcastle-Ottawa scale, patient characteristics, study characteristics, and intermediate- to long-term (⩾ 3 months) main outcomes.
Definitions and outcomes
Main outcomes of interest for this review included RV dysfunction, New York Heart Association (NYHA) functional classification, 6-minute walk test distance, and QoL. RV dysfunction was typically defined by echocardiographic evidence of RV hypokinesis and/or dilatation. In studies that did not explicitly report RV dysfunction, the highest reported prevalence of RV hypokinesis, RV dilatation, or abnormal tricuspid annular plane systolic excursion were extracted. Functional capacity was assessed with the NYHA functional classification, comprised of four categories of increasing functional impairment: no limitation of physical activity by shortness of breath (class I, no symptoms); dyspnea with ordinary physical activity (class II, mild symptoms); dyspnea with less than ordinary activity but none at rest (class III, moderate symptoms); and symptoms of cardiac insufficiency at rest and inability to carry out any physical activity without discomfort (class IV, severe symptoms). The 6-minute walk test measures the distance walked over a 6-minute period and serves as an indicator of submaximal aerobic capacity. 6 For each outcome, data were extracted at the latest follow-up period in each study. Health-related QoL was assessed with the Physical Component Summary (PCS) from the SF-12 or SF-36 questionnaire and the Pulmonary Embolism Quality of Life (PEmb-QoL) questionnaire. Scores for PCS range from 0 to 100 (mean: 50, standard deviation: 10), with higher values representing better health-related QoL. The total score for the PEmb-QoL ranges from 6 to 27, with lower values representing better QoL. In studies that reported at least one outcome of interest, we also extracted data on all-cause mortality, recurrent DVT, and PE recurrence.
Data synthesis
Random effects meta-analysis models were developed based on the a priori assumption that treatment effects would be heterogeneous given differences in patient characteristics and PE treatments among studies. For each outcome, the pooled estimate and 95% confidence interval were calculated. Meta-analysis of proportions was performed using the Freeman-Tukey double arcsine transformation to calculate the weighted summary proportion under the random effects model. A continuity correction of 0.5 was applied to the numerator for zero-event outcomes. Total scores for the PEmb-QoL were reported descriptively since the original studies exclusively reported medians and interquartile ranges. Pooled median PEmb-QoL was calculated using weighted averages where sample size was the weighting factor. Forest plots were used to illustrate individual study findings and pooled meta-analysis results, when applicable. We used the I2 statistic to estimate heterogeneity of effects across studies with values of ⩽ 25%, 50%, and ⩾ 75% representing low, moderate, and high inconsistency, respectively. 7 When sufficient data allowed, post hoc subgroup analyses were performed to explore potential sources of heterogeneity. When possible, analysis and reporting of the outcomes of interest were stratified by treatment for acute PE, namely anticoagulation alone or anticoagulation plus thrombolysis. The risk of a given outcome with thrombolysis versus anticoagulation was reported with a pooled odds ratio (OR) where an OR > 1 favors anticoagulation and an OR < 1 favors thrombolysis. Statistical analyses were performed using MedCalc version 12.5 (MedCalc Software, Ostend, Belgium) and Comprehensive Meta-Analysis version 2.2 (Biostat, Englewood, NJ, USA).
Results
Our initial database search retrieved 667 titles and abstracts; hand-searching relevant bibliographies identified 12 additional records. After screening records for inclusion criteria, 87 full-text articles were reviewed for eligibility. Ultimately, 26 studies representing 3671 patients were included in the final analysis. A flow diagram of study identification and selection is shown in Figure 1.
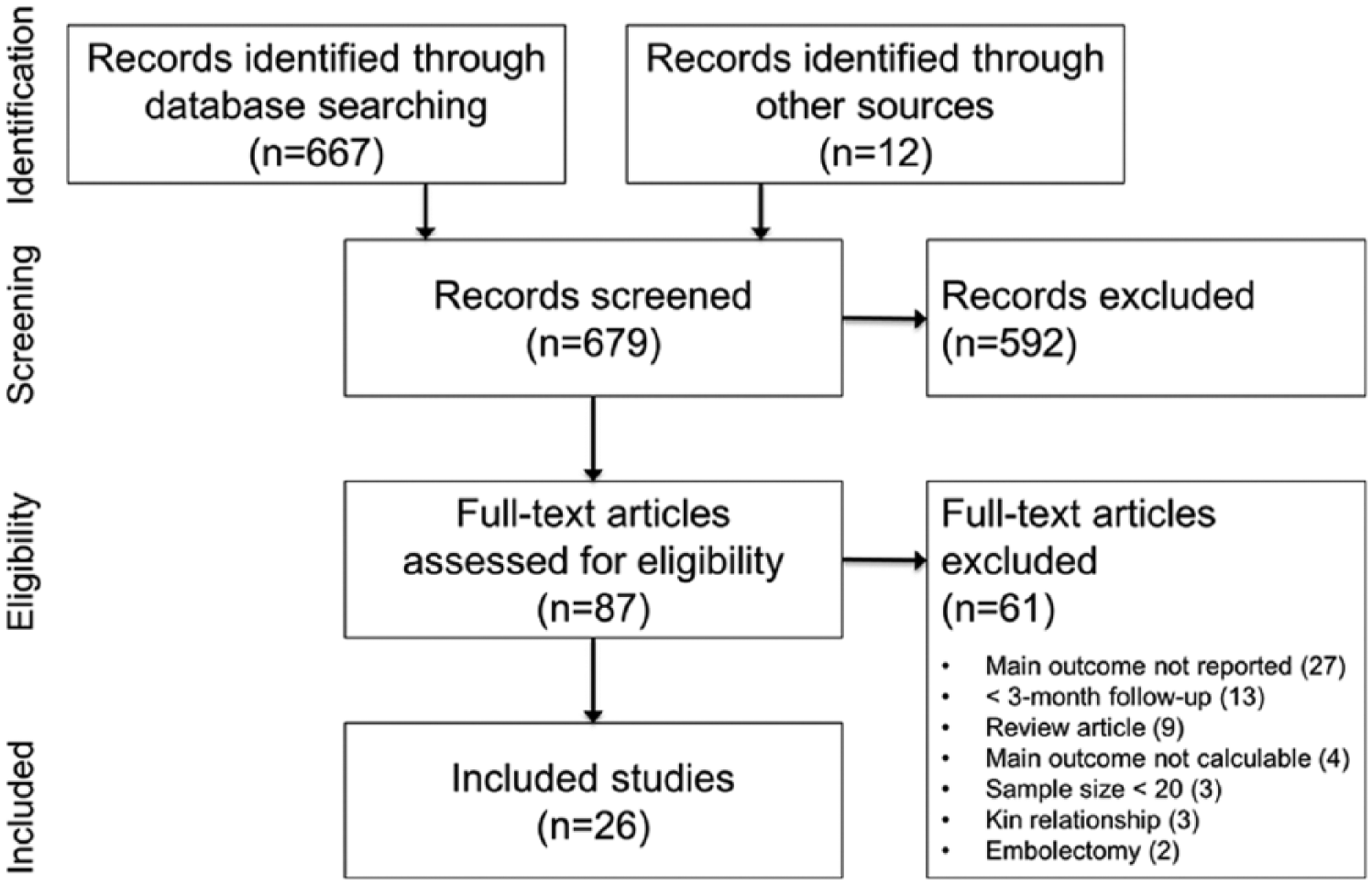
PRISMA flow diagram.
Baseline patient characteristics are reported in Table 1. Mean age was 59 years, and 50% of patients were female. Of the 26 included studies, 16 enrolled more than 100 patients and 15 were retrospective. Patients were treated with anticoagulation alone in 11 studies, thrombolysis or anticoagulation in 10 studies, thrombolysis in 1 study, and unspecified treatments in 4 studies. Median follow-up duration was 18 months (range: 3 to 92 months) (Table 2). Risk of bias was high in 10 studies, intermediate in 8 studies, and low in 8 studies (Supplementary Table 2).
Baseline patient characteristics.
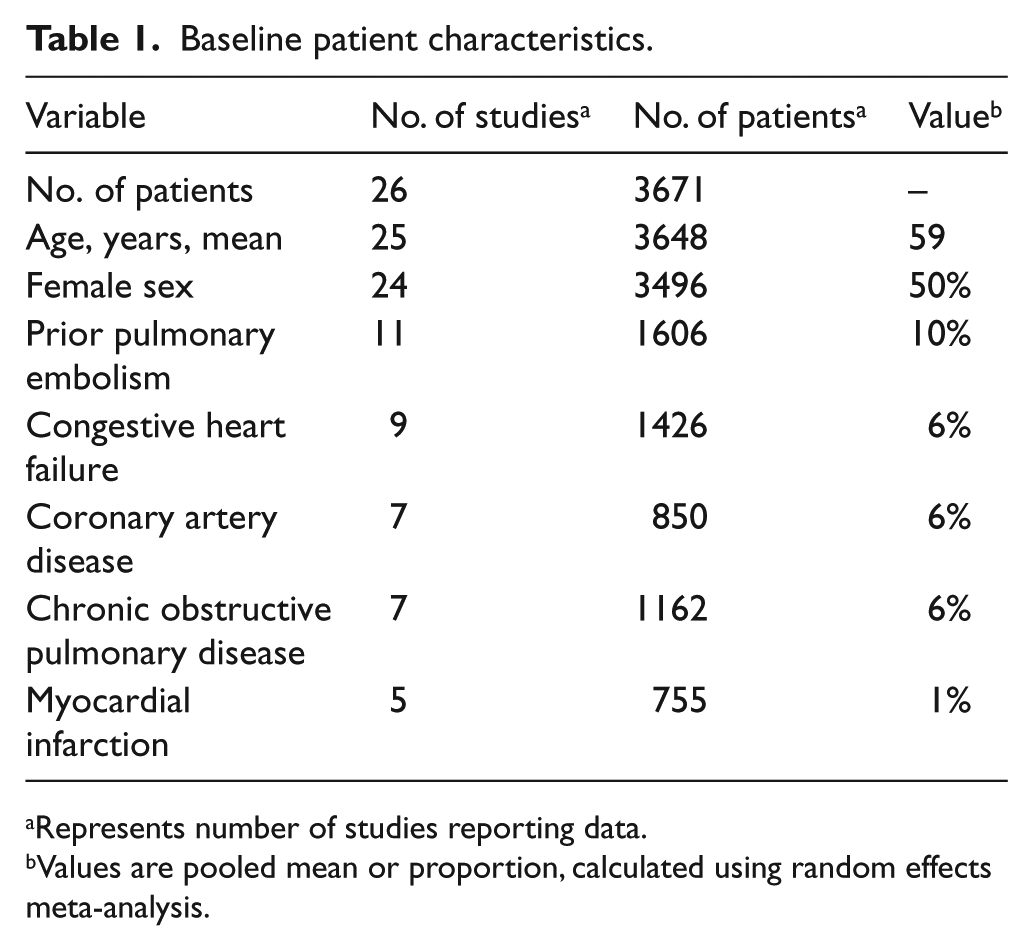
Represents number of studies reporting data.
Values are pooled mean or proportion, calculated using random effects meta-analysis.
Study characteristics.
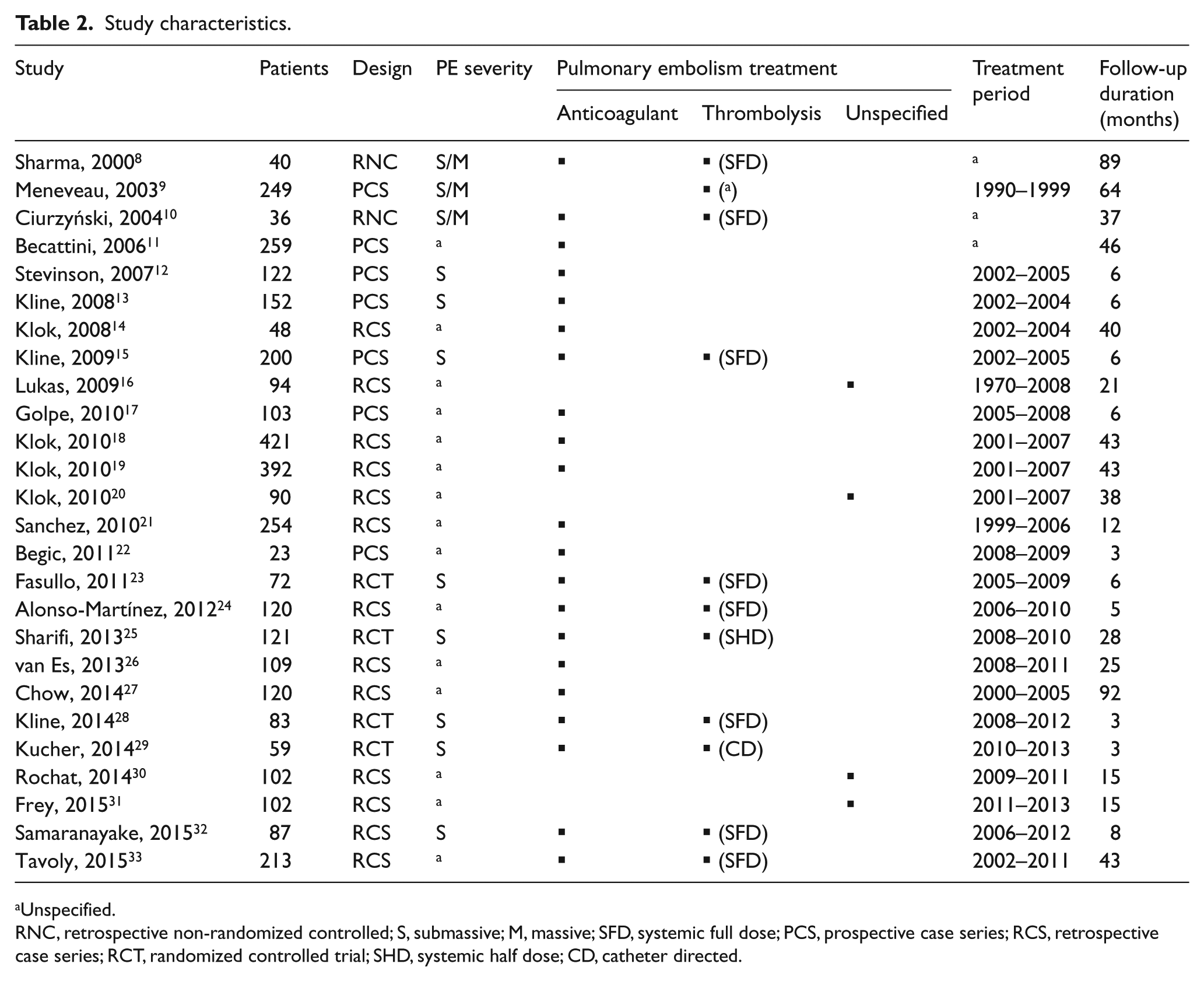
Unspecified.
RNC, retrospective non-randomized controlled; S, submassive; M, massive; SFD, systemic full dose; PCS, prospective case series; RCS, retrospective case series; RCT, randomized controlled trial; SHD, systemic half dose; CD, catheter directed.
At a median 6 months following PE diagnosis, the pooled prevalence of RV dysfunction was 18.1% (95% CI: 11.6% to 25.5%) (Supplementary Figure 1). Significant heterogeneity was identified among studies (I2=88%, p<0.001), although no patient or study characteristics explained RV dysfunction incidence in subgroup analysis (Table 3). There was no statistical difference in risk of RV dysfunction in patients treated with thrombolysis versus anticoagulation (OR: 0.51, 95% CI: 0.24 to 1.13, p=0.10) (Supplementary Figure 2).
Subgroup analysis of baseline factors on outcomes.
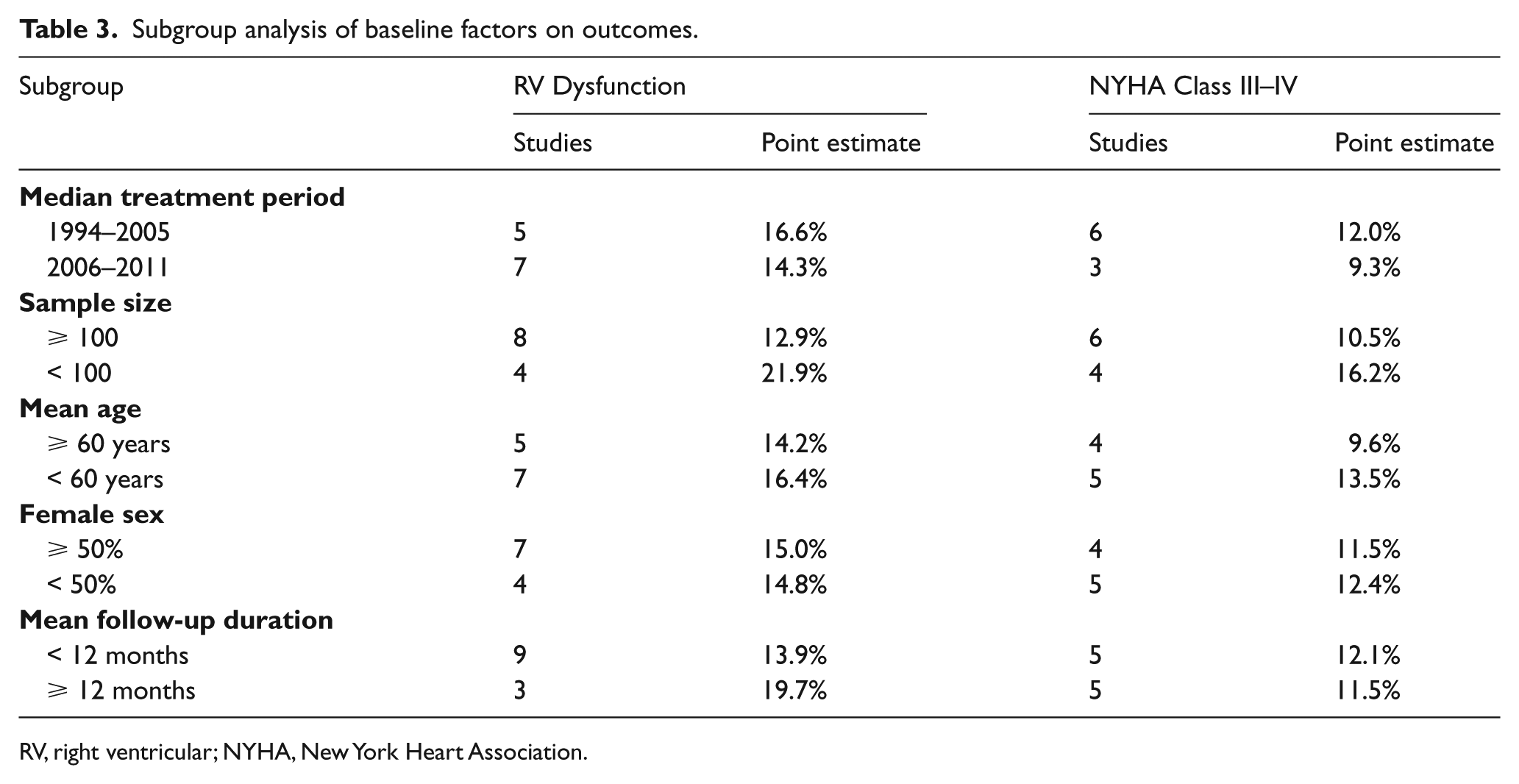
RV, right ventricular; NYHA, New York Heart Association.
At a median 40 months following PE diagnosis, the pooled prevalence of mild or greater functional impairment (NYHA II–IV) was 33.2% (95% CI: 21.3% to 46.4%) (Supplementary Figure 3). At a median 9 months following PE diagnosis, the pooled prevalence of moderate or severe functional impairment (NYHA III–IV) was 11.3% (95% CI: 8.7% to 14.1%) (Supplementary Figure 4). Significant heterogeneity among studies was identified for these outcomes, although in subgroup analysis no patient or study characteristic explained this heterogeneity (Table 3). Patients treated with thrombolysis had no significant difference in risk of moderate–severe over none or mild functional impairment compared to those treated with anticoagulation (OR: 0.48, 95% CI: 0.15 to 1.49, p=0.20) (Supplementary Figure 5).
At a median 12 months following PE diagnosis, the pooled 6-minute walk distance was 415 m (95% CI: 372 to 458 m) (Supplementary Figure 6). For reference, this value is less than the 5th percentile compared to age- and sex-matched norms. 34 Significant heterogeneity was identified among studies (I2=95%, p<0.001); however, the number of studies reporting this outcome was insufficient to perform subgroup analyses to explore reasons for heterogeneity.
The pooled SF-36 PCS score was 44.8 (95% CI: 43 to 46) at a median 25 months following PE diagnosis (Supplementary Figure 7). For reference, this value represents the 40th percentile compared to age- and sex-matched norms. 35 Significant heterogeneity was identified among studies (I2=64%, p=0.02); however, the number of studies reporting this outcome was insufficient to perform subgroup analyses. Median values for the PEmb-QoL ranged from 7.1 to 9.5 among studies (overall median: 9.1). Median and interquartile ranges are plotted for each study in Supplementary Figure 8, but PEmb-QoL data were not pooled due to highly positively skewed distributions.
The incidence of ancillary outcomes was 10.8% (95% CI: 5.9% to 16.8%) for all-cause mortality, 8.4% (95% CI: 2.1% to 18.4%) for recurrent DVT, and 5.6% (95% CI: 3.2% to 8.7%) for PE recurrence. Each of these outcomes tended to favor thrombolysis over anticoagulation, including all-cause mortality (OR: 0.49, 95% CI: 0.22 to 1.09, p=0.08), recurrent DVT (OR: 0.28, 95% CI: 0.08 to 0.90, p=0.03), and PE recurrence (OR: 0.37, 95% CI: 0.09 to 1.59, p=0.18).
Discussion
This systematic review and meta-analysis demonstrates that following PE, there is an 18% prevalence of persistent RV dysfunction and an 11% prevalence of moderate to severe dyspnea, suggesting a significantly higher rate of poor functional status after PE than the 4% rate of chronic thromboembolic pulmonary hypertension following PE. Furthermore, PE survivors walk substantially shorter distances than predicted on the 6-minute walk test and have generic QoL scores that are in the 40th percentile compared to the population norms. Additionally, patients suffered a high rate of mortality (10.8%) after PE and a 14% rate of VTE recurrence. This analysis showed lower incidences of RV dysfunction and functional impairment in patients who received thrombolysis during their acute PE, although these findings were not statistically significant. Overall, our findings support the existence of a relatively common post-PE syndrome characterized by a combination of RV dysfunction, functional limitation, exercise intolerance, and reduced QoL, in the absence of the full criteria required for chronic thromboembolic pulmonary hypertension diagnosis.
Echocardiography is routinely used for risk stratification of patients with acute PE by chronicling RV dysfunction, dilation, and elevated pulmonary pressures. 36 Acutely, RV dysfunction as detected by echocardiography is associated with worse 30-day outcomes after PE. 37 However, the long-term prognostic significance of persistent RV dysfunction with no or mild symptomatology is currently unknown. Future studies should explore the relationship between persistent RV dysfunction and long-term QoL, functional status, exercise tolerance, and mortality.
NYHA status is significantly related to mortality in patients with congestive heart failure and pulmonary hypertension. 38 While its prognostic significance in PE survivors is unclear, the relatively high prevalence of NYHA status II or greater in our study is notable. However, we acknowledge that there is subjectivity in assessment of NYHA class, and that most of the studies included in this review were not randomized or blinded, complicating interpretation of the NYHA class data.
The 6-minute walk distance is a simple method of assessing exercise capacity that correlates with disease severity and mortality in several chronic cardiopulmonary diseases. 39 It has been used in a multitude of pulmonary hypertension trials, making it particularly relevant to the post-PE population. 40 The population norm in 60-year-old patients is approximately 575 m, 34 and a distance of approximately 40 m is considered a minimal clinically important difference. 41 Our finding that PE survivors are able to walk considerably shorter distances (415 m) than the general population may be indicative of incomplete cardiopulmonary recovery following PE, although more robust studies are required to validate this finding.
The results of this review support the idea that general QoL is diminished in PE survivors, although more prospectively designed research needs to be performed to understand the true, independent impact PE has on QoL. The SF-36 is well validated, but suffers from a lack of disease specificity and the potential to be influenced by confounding conditions. The PEmb-QoL is a relatively new disease-specific measure that has been validated in several populations; however, a minimally important difference has not been established, and interpretation of the overall score of the PEmb-QOL is difficult, as most studies report scores for the various domains and not a composite score. Our finding that the PEmb-QOL composite score appears to show relatively normal QOL, especially in light of the lower QOL as measured by the SF-36, may be the result of different populations and differing lengths of follow-up.
Post-PE syndrome remains poorly characterized, and a significant amount of research is required to understand its natural history and pathophysiology. It is still unclear which baseline patient characteristics and pathologic risk factors (e.g. thrombus location, myocardial injury) correlate with long-term disability. Given that many of the symptoms are subjective and patient-reported, and that even tests such as the 6-minute walk distance can be influenced by patient motivation, there is a significant need for well-designed rigorous prospective trials with both objective and subjective endpoints. Until post-PE syndrome is characterized more clearly, routine screening with echocardiography, QoL questionnaires, or exercise testing cannot be routinely recommended following PE. While baseline patient characteristics do not suggest that overall patients were unhealthy before PE, baseline data for outcomes such as QoL or 6-minute walk distance were not possible to acquire since patients first present in the presence of PE symptoms. However, given the pooled 18% incidence of RV dysfunction, 33% incidence of NYHA functional status II or greater, and 6-minute walk distance less than the 5th percentile in PE survivors in this analysis, greater clinical attention to long-term morbidity after PE is warranted. Future research should focus on identifying subpopulations that are at higher risk for clinically significant functional and QoL impairment after PE. Such patients may require dedicated screening and may be ideal subjects of research aimed at preventing or mitigating post-PE syndrome.
Clot removal strategies such as systemic and catheter-directed thrombolysis have thus far focused on short-term outcomes such as death, deterioration, and reversal of RV dysfunction, with the exception of several studies identified in this review. 42 The possibility that active thrombus reduction may have an effect on long-term outcomes is intriguing. Mechanistically, rapid unloading of the right ventricle and increased thrombus clearance may prevent maladaptive cardiopulmonary remodeling. Future studies seeking to define the roles of these therapies in acute PE should take into account long-term clinically relevant outcomes in their design and conduct.
Limitations
This meta-analysis has certain limitations pertaining to the quality of studies available for analysis that may influence interpretation. Heterogeneity in study design, treatments, and outcomes among studies was frequently observed, which confounded data interpretation. Since the number of studies contributing to each outcome in this meta-analysis was too small to accurately detect publication bias by quantitative techniques or by funnel plot inspection, the risk of publication bias must be considered. There was also considerable variation in the completeness of data reported among studies. Inclusion of data from non-randomized, non-controlled, and retrospective studies may have introduced bias into the results. Indeed, most included studies were classified as intermediate or high risk of bias. The term ‘thrombolysis’ primarily encompassed full-dose systemic thrombolysis with few eligible studies on reduced-dose systemic thrombolysis and catheter-directed thrombolysis. Separate analyses were insufficiently powered, so relative effects of the method or dose of delivery could not be ascertained. Baseline (pre-PE) echocardiographic data were generally not reported; therefore, pre-existing RV dysfunction could not be ruled out. Finally, there was a wide range of follow-up durations in the included studies; therefore, a detailed assessment of the time to events is not possible in the current analysis.
Conclusions
Survivors of PE often manifest persistent RV dysfunction, impaired functional status, diminished exercise tolerance, and low QoL scores, suggestive of a spectrum of a clinically significant, post-PE syndrome. Whether thrombolysis during the acute event positively influences these outcomes is unclear and merits further research.
Supplemental Material
sj-pdf-1-vmj-10.1177_1358863X16670250 – Supplemental material for Persistent right ventricular dysfunction, functional capacity limitation, exercise intolerance, and quality of life impairment following pulmonary embolism: Systematic review with meta-analysis
Supplemental material, sj-pdf-1-vmj-10.1177_1358863X16670250 for Persistent right ventricular dysfunction, functional capacity limitation, exercise intolerance, and quality of life impairment following pulmonary embolism: Systematic review with meta-analysis by Akhilesh K Sista, Larry E Miller, Susan R Kahn and Jeffrey A Kline in Vascular Medicine
Supplemental Material
sj-pdf-2-vmj-10.1177_1358863X16670250 – Supplemental material for Persistent right ventricular dysfunction, functional capacity limitation, exercise intolerance, and quality of life impairment following pulmonary embolism: Systematic review with meta-analysis
Supplemental material, sj-pdf-2-vmj-10.1177_1358863X16670250 for Persistent right ventricular dysfunction, functional capacity limitation, exercise intolerance, and quality of life impairment following pulmonary embolism: Systematic review with meta-analysis by Akhilesh K Sista, Larry E Miller, Susan R Kahn and Jeffrey A Kline in Vascular Medicine
Footnotes
Acknowledgements
The authors thank Angela K Zimmermann, PhD for assistance with data extraction and verification.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AKS and SRK report no conflict of interest. JAK reports within the past 3 years receiving funding personally from Janssen Pharmaceuticals for consulting. JAK’s institution, Indiana University School of Medicine, has received grant funding from the National Institutes of Health for investigator-initiated research. JAK’s institution has received contract funding from Diagnostica Stago for industry-initiated research and has received contract funding from Roche Diagnostics and Mallinckrodt Pharmaceuticals for investigator-initiated research.
Funding
The authors disclosed receipt of the following financial support: LEM received financial support from Weill Cornell Medical College to perform the meta-analysis.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.