
Abstract
The aim of this study was to investigate the effect of cigarette smoking on peripheral and central blood pressure (BP) in a group of young stage I hypertensives. A total of 344 untreated subjects from the HARVEST study were examined (mean age 37±10 years). Patients were divided into three groups based on smoking status: non-smokers, light smokers (⩽5 cigarettes/day) and moderate-to-heavy smokers (>5 cigarettes/day); and into three groups by age: 18–29, 30–39 and ⩾40 years. Central BP measurements and augmentation index (AIx) were calculated from brachial pressure waveform, with applanation tonometry, by means of the Specaway DAT System plus a Millar tonometer. The central waveform was derived from peripheral BP using the same software system of the SphygmoCor System pulse wave analysis. In addition, two indirect measurements of arterial stiffness were calculated: pulse pressure (PP) and systolic BP amplification. Central systolic BP and PP were higher in smokers than in non-smokers (systolic BP: 121.9±13.1 mmHg in non-smokers, 127.2±16.5 mmHg in light smokers, 126.7±15.3 mmHg in those who smoked >5 cigarettes/day, p=0.009; PP: 37.7±9.8 mmHg, 41.5±13.1 mmHg, 41.9±10.5 mmHg, respectively, p=0.005). Lower systolic BP amplification (p<0.001) and PP amplification (p=0.001) were observed in smokers compared to non-smokers. In a two-way ANCOVA analysis, systolic BP amplification markedly declined across the three age groups (p=0.0002) and from non-smokers to smokers (p=0.0001), with a significant interaction between smoking and age group (p=0.05). The AIx was higher in smokers compared to non-smokers (p=0.024). In young hypertensives, smoking has a detrimental effect on central BP, accelerating the age-related decline in BP amplification.
Introduction
A number of studies have found that chronic cigarette smoking is associated with increased arterial stiffness1,2 and with a decrease of both large and medium-size artery compliance.3–5 Arterial stiffness is traditionally assessed by means of pulse wave velocity (PWV). However, other measures of arterial stiffness can provide relevant clinical information such as augmentation index (AIx), which gives an estimate of aortic wave reflection 6 and central-peripheral blood pressure (BP) amplification, which progressively decreases with aging. 7 Few data are reported regarding the effect of cigarette smoking on central BP. Central BP induces a more direct mechanical stress on the left ventricle and vital organ vasculature, 8 and its importance has been reported in large-scale intervention trials and population-based study.9,10 Central systolic BP (SBP) was also demonstrated to be more valuable than other BP variables in predicting cardiovascular mortality. 11 Some previous studies observed that central SBP was higher in smokers compared to non-smokers.2,12,13 However, these studies were performed in young healthy subjects, 2 normotensive adults, 12 or general populations. 13 Little is known about the impact of cigarette smoking on central BP in young subjects with hypertension.
The aim of the present studies was to investigate the effect of cigarette smoking on peripheral BP, central BP and pressure amplification in a group of young-to-middle age stage I hypertensive subjects from the HARVEST (Hypertension and Ambulatory Recording VEnetia STudy) study.
Material and methods
The study participants took part in HARVEST, a long-term prospective observational study, initiated in April 1990, involving 17 centres in northeastern Italy. Patients were all Caucasian and native Italian, young-to-middle age (18–45 years old), stage I hypertensives (clinic SBP: 140–159 mmHg, and/or clinic diastolic BP (DBP): 90–99 mmHg) who had never been treated for hypertension before enrolment. Patients with diabetes, renal function impairment, cardiac diseases or secondary forms of hypertension were excluded. Secondary forms of hypertension were identified on the basis of a complete history, physical examination and by standard diagnostic procedures. These included serum potassium, plasma renin activity, plasma and urinary aldosterone and urinary catecholamines. To further exclude the presence of renovascular disease, all patients underwent a Doppler examination of the renal arteries or renal scintigraphy. Recruitment of patients was obtained through collaboration with local general practitioners. Written informed consent was given by the participants. The study was approved by the HARVEST Ethics Committee and by the Ethics Committee of the University of Padova.
The baseline data included medical and family history, a questionnaire of current use of coffee, alcoholic beverages, smoking status and physical activity habits.14 –16 Participants completed questionnaires about their medical history, family history of hypertension, cigarette smoking, physical activity, coffee intake, and alcohol use. Coffee consumption was defined as the number of caffeine-containing coffees drunk per day. A positive family history of hypertension was defined as one or two parents having hypertension and/or taking antihypertensive treatment. Patients were defined smokers if they smoked at least one cigarette per day and were categorized into four groups according to the exact number of cigarettes smoked per day: non-smokers, 1–5 cigarettes/day, 6–10 cigarettes/day, 11–20 cigarettes/day. Subjects were categorized as non-exercisers if they did not regularly perform any sports activity and as exercisers if they had performed sports at least once a week during the previous 2 months. Subsequently, among the non-exercisers, the fully sedentary subjects were distinguished from those who performed light physical activities, such as walking, gardening, etc. Among the exercisers, the subjects performing competitive sports were separated from those not involved in competitions. More details about the interview, lifestyle assessment, and criteria used for subjects’ classification according to lifestyle have been reported elsewhere.14 –16 All subjects underwent physical examination, anthropometry and routine blood chemistry. After an overnight fast, a morning sample of blood was obtained to measure serum glucose and lipid profile. Office BP at entry was the mean of six measurements obtained with a mercury sphygmomanometer, during two visits, performed 2 weeks apart. After enrolment, patients also underwent 24-hour BP monitoring, using an A&D TM2420 model 7 (A&D, Tokyo, Japan) or an ICR Spacelabs 90207 monitor (Spacelabs, Redmond, WA, USA). Both of these devices were previously validated17,18 and shown to provide comparable results. 19 Twenty-four-hour urine samples were collected from all participants for catecholamine assessment. Immediately after completion, urine volume was measured and urine specimens were frozen (−20°C) and sent to the Coordinating Office at the University of Padova, where epinephrine and norepinephrine were measured by a high-performance liquid chromatography method (HPLC).
Central blood pressure assessment
Arterial distensibility assessment was performed in 344 subjects enrolled in the four HARVEST centres who agreed to participate in this substudy. Central BP was assessed from brachial pressure waveform, recorded at the radial artery with applanation tonometry. We used the DAT System (SN1002-960604-12; Specaway, Sydney, Australia) connected to a Millar tonometer (SPC-301; Millar Instruments, Huston, TX, USA). After acquiring 30 sequential waveforms at the radial artery, the same software system of the SphygmoCor® System pulse wave analysis, which incorporated a validated transfer function, was used to generate an average peripheral and corresponding ascending aortic pressure waveform. 20 From the radial pulse wave analysis, using a generalized transfer function, derived from the invasive measurements, we obtained central BP values.20 –23 The device also returned the radial AIx as the ratio of the difference between the pressure at the second systolic shoulder and diastolic BP to that between the diastolic BP and pressure at the first inflection point: AIx = 100*(P2 – DBP)/(P1 – DBP). 24
Statistical analysis
Pulse pressure (PP) was calculated as the difference between SBP and DBP. Mean BP was calculated as diastolic BP+PP/3. The central-peripheral SBP and PP amplification was calculated by subtracting the central from peripheral BP measurement. Patients were divided into three smoking groups according to how many cigarettes they smoked per day: non-smokers, light smokers (⩽5 cigarettes/day; n=43 subjects) and moderate-to-heavy smokers (>5 cigarettes/day; n=33 subjects); and into three age groups: 18–29 years (n=83), 30–39 years (n=131) and ⩾40 years (n=130).
Data are presented as mean ± standard deviation. Differences between means were assessed by one-way ANCOVA, adjusting for age and sex. One-way ANCOVA analysis was performed to examine differences between smoking groups for central SBP and PP, and for SBP and PP amplification, adjusting for several clinical variables (age, sex, body mass index (BMI), lifestyle habits (smoking habit, coffee and alcohol use, physical activity habit), parental hypertension, mean BP and heart rate (HR)). Pairwise comparisons between smoking groups were assessed by post hoc analysis (Tukey’s test). Two-way ANCOVA analysis was performed to investigate the interactive effect of smoking with age on central BP data, adjusting for the clinical variables reported above. The same analyses were repeated to test the interaction between smoking habits and coffee and alcohol consumption. A two-tailed probability value <0.05 was considered significant. All analyses were performed using SYSTAT version 12 (SPAA Inc., Evanston, IL, USA).
Results
Baseline characteristics and peripheral blood pressure
The baseline characteristics of the study participants, by smoking group, are presented in Table 1. Smokers constituted 22.1% (n=76) of the study participants. Among these, 10.8% smoked 1–5 cigarettes/day, 5.3% smoked 6–10 cigarettes/day, and 6% smoked 11–20 cigarettes/day; subjects who smoked more than 20 cigarettes/day were excluded according to the HARVEST study protocol. Smokers were less active than non-smokers and drank more alcohol and coffee; all differences were statistically significant when patients were divided into three groups (non-smokers, ⩽5 cigarettes, >5 cigarettes). When patients were divided into two groups, non-smokers and smokers, the difference for frequencies of alcohol users was no longer significant. When the study population was divided into three smoking groups, no smoking-related differences were found for peripheral BP, PP, HR, metabolic data and catecholamine levels; however, triglyceride levels were higher in the two smoking groups (borderline significance, p=0.06). When patients were divided into two groups, smokers presented lower peripheral DBP (borderline significant, p=0.058) and higher triglyceride levels that reached a level of statistical significance (p=0.019).
Baseline characteristics of study participants according to smoking group.
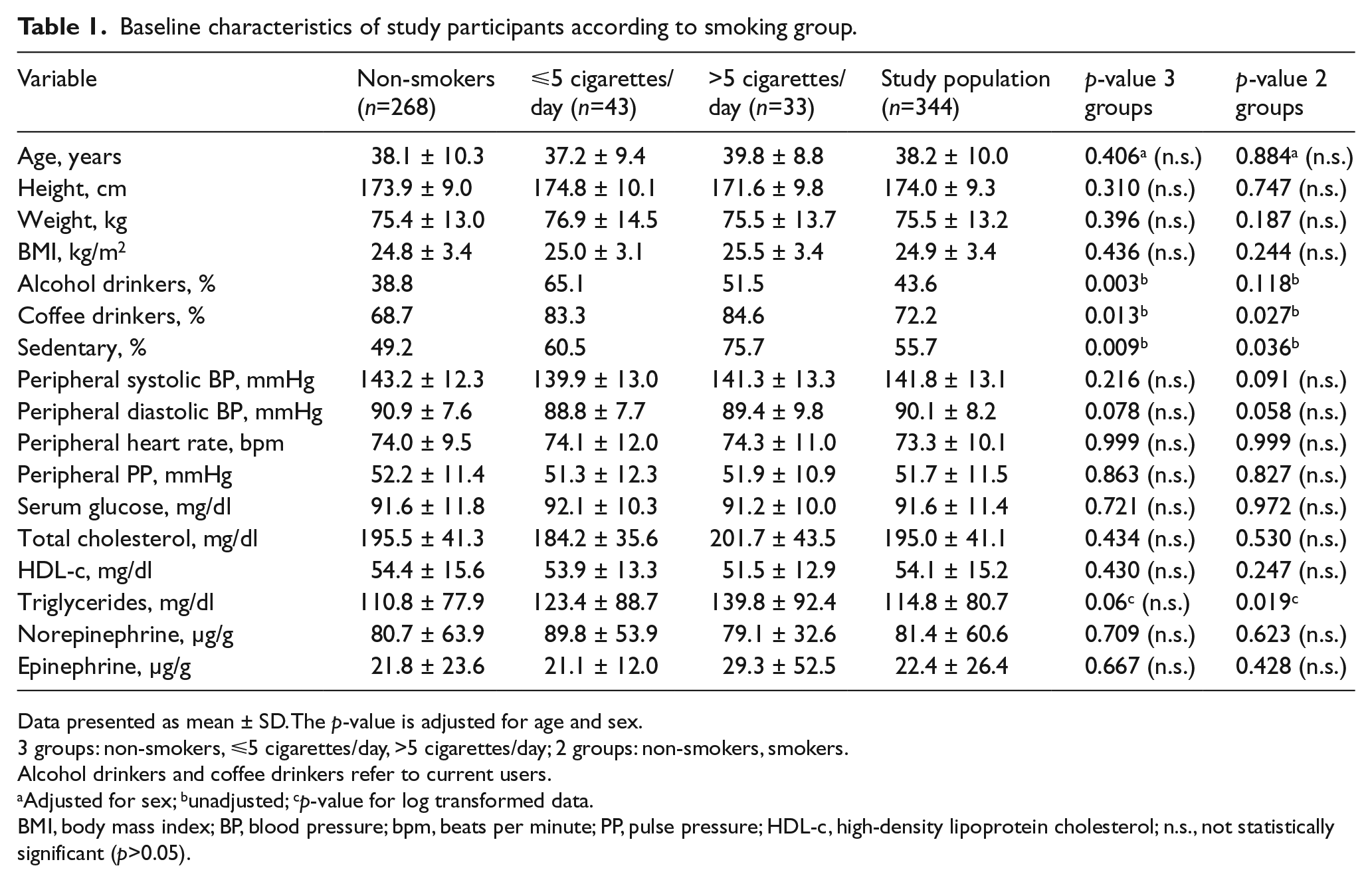
Data presented as mean ± SD. The p-value is adjusted for age and sex.
3 groups: non-smokers, ⩽5 cigarettes/day, >5 cigarettes/day; 2 groups: non-smokers, smokers.
Alcohol drinkers and coffee drinkers refer to current users.
Adjusted for sex; bunadjusted; cp-value for log transformed data.
BMI, body mass index; BP, blood pressure; bpm, beats per minute; PP, pulse pressure; HDL-c, high-density lipoprotein cholesterol; n.s., not statistically significant (p>0.05).
Central haemodynamic measurements
Central haemodynamic measurements are reported in Table 2. Both light smokers and those who smoked more than 5 cigarettes per day had significantly higher central SBP than non-smokers (F-ratio 6.41, p=0.0019 for fully adjusted model without mean BP; F-ratio 7.84, p=0.0005 for fully adjusted model including mean BP) (Figure 1a). Post hoc analysis showed that the difference was significant for both light smokers and those who smoked more than 5 cigarettes per day compared to non-smokers (p=0.020 and 0.018, respectively, for the model without inclusion of mean BP; p=0.004 and 0.016, respectively, after inclusion of mean BP). When patients were divided into two smoking groups, smokers and non-smokers, the difference remained highly significant: F-ratio 12.99, p=0.0004 without inclusion of mean BP; F-ratio 15.34, p=0.0001 after inclusion of mean BP). Smokers also had higher central PP (F-ratio 4.09, p=0.018) than non-smokers (Figure 1b). Post hoc analysis showed near significant differences for both light smokers and those who smoked more than 5 cigarettes per day compared to non-smokers (p=0.08 and 0.07, respectively). The inclusion in the model of mean BP increased the significance of the differences (F-ratio 4.91, p=0.008; p=0.03 for light smokers compared to non-smokers, p for those who smoked >5 cigarettes/day remained unchanged). Again, when patients were divided into two smoking groups, the difference was highly significant (F-ratio 8.48, p=0.0039; F-ratio 9.5114, p=0.0022 after inclusion of mean BP in the model). There was no statistically significant difference in central DBP between smokers and non-smokers (84.2±8.0 mmHg in non-smokers, 85.7±8.9 mmHg in light smokers, 84.7±10.3 mmHg in those who smoked more than 5 cigarettes per day; p value was not statistically significant comparing either two or three smoking groups). Smokers also had significantly lower SBP amplification (Figure 2a) (F-ratio 7.97, p=0.0004 without inclusion of BP in the model; F-ratio 7.19, p=0.0009 after inclusion of mean BP) and PP amplification (Figure 2b) (F-ratio 3.72, p=0.025; F-ratio 3.31, p=0.038 after inclusion of mean BP) compared to non-smokers. Post hoc analysis showed a significant difference between both groups of smokers and non-smokers (p=0.002 and 0.030, respectively; p=0.007 and p=0.020, respectively, after inclusion in the model of mean BP) for SBP amplification, while the post hoc analysis for PP amplification identified no statistically significant difference. When the analysis was repeated in patients divided into two groups, non-smokers and smokers, the difference was significantly higher between the two groups (F-ratio 15.04, p=0.0001 for SBP amplification; F-ratio 14.06, p=0.0002 for PP amplification). AIx was higher in smokers (23.8±0.34% in light smokers and 19.8±0.41% in those who smoked >5 cigarettes per day) than in non-smokers (15.3±0.13%) (data presented as mean±SE), although the difference was of borderline significance (p=0.068, adjusted for age, sex, lifestyle habits, parental hypertension and baseline HR; p=0.059 after inclusion of mean BP). When patients were divided into two groups, smokers and non-smokers, the difference for AIx reached the level of statistical significance (p=0.024).
Central haemodynamics of study participants according to smoking group.
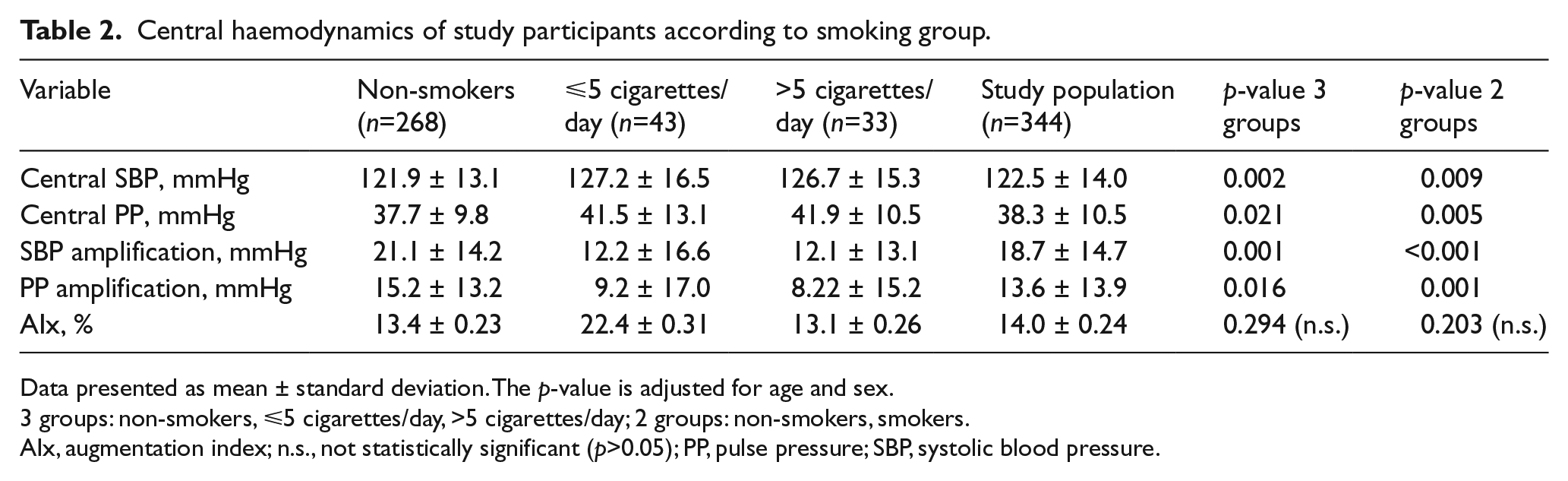
Data presented as mean ± standard deviation. The p-value is adjusted for age and sex.
3 groups: non-smokers, ⩽5 cigarettes/day, >5 cigarettes/day; 2 groups: non-smokers, smokers.
AIx, augmentation index; n.s., not statistically significant (p>0.05); PP, pulse pressure; SBP, systolic blood pressure.
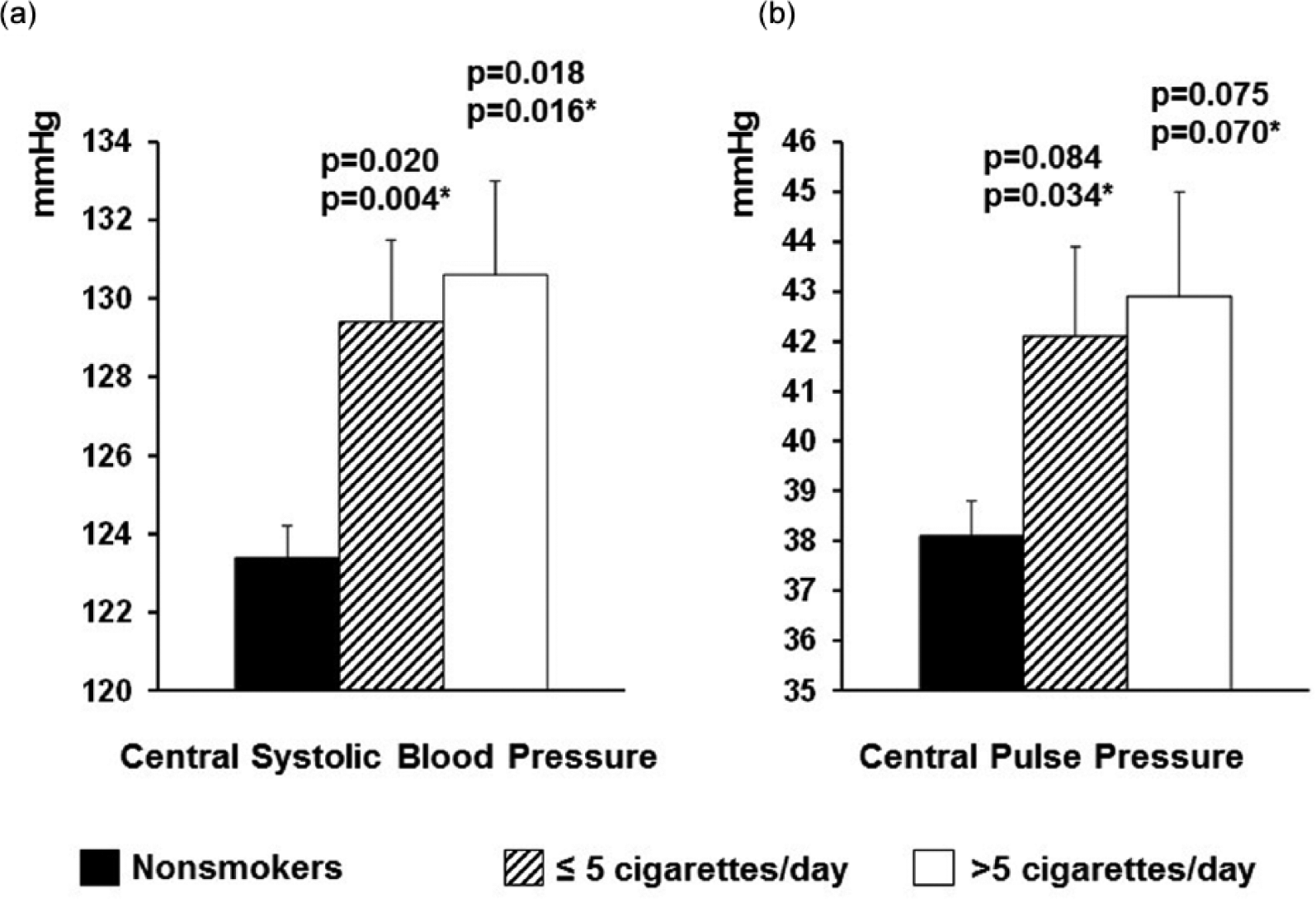
(a) Central systolic blood pressure according to smoking group. (b) Central pulse pressure according to smoking group. The p-value versus non-smokers is adjusted for age, sex, BMI, heart rate (HR), lifestyle habits and parental hypertension. *The p-value is adjusted for age, sex, BMI, HR, lifestyle habits, parental hypertension and mean arterial pressure. Post hoc analysis, Tukey’ s test.
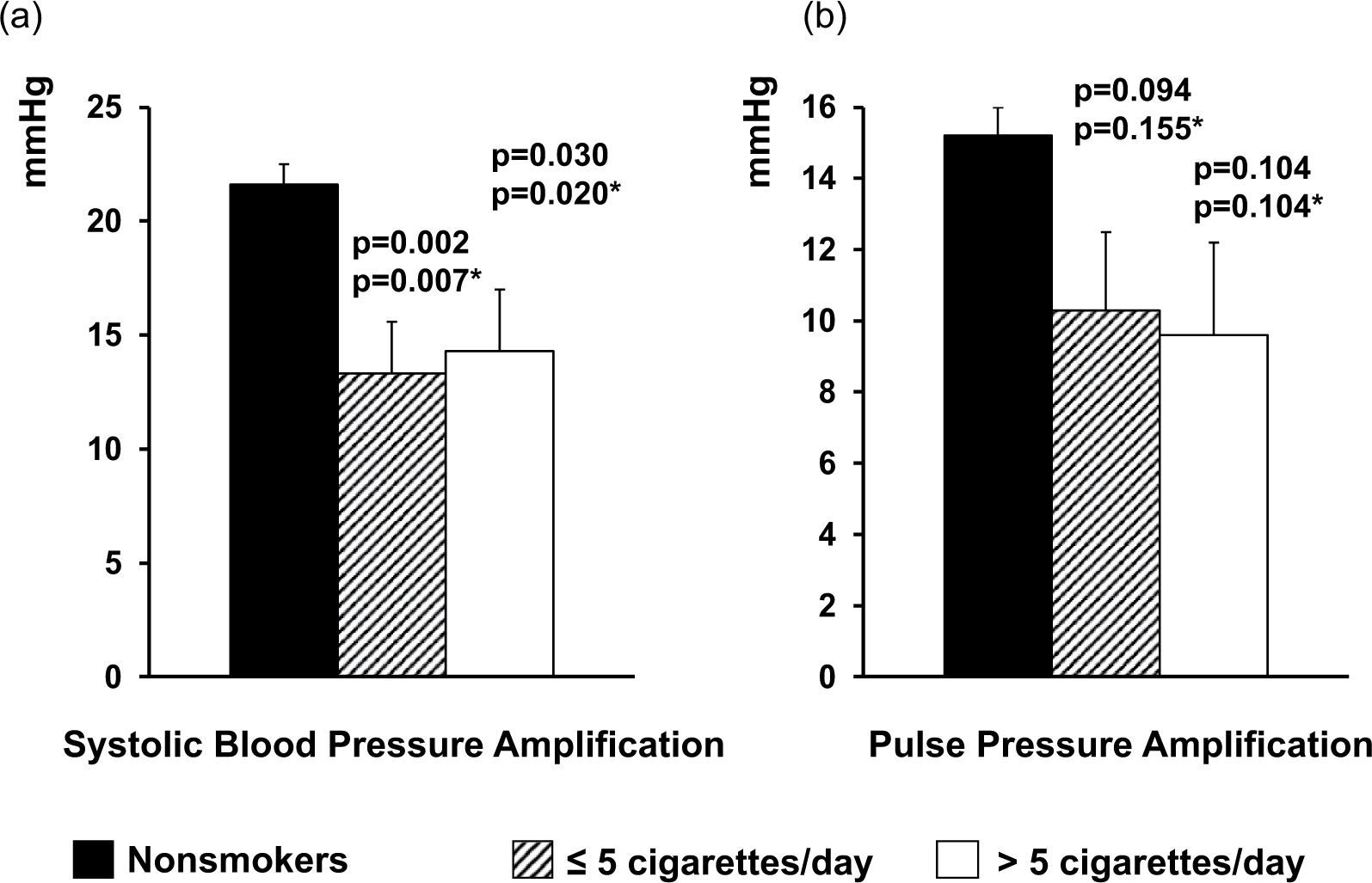
(a) Systolic blood pressure amplification according to smoking group. (b) Pulse pressure amplification according to smoking group. The p-value versus non-smokers is adjusted for age, sex, BMI, heart rate (HR) lifestyle habits and parental hypertension. *The p-value is adjusted for age, sex, BMI, HR, lifestyle habits, parental hypertension and mean arterial pressure. Post hoc analysis, Tukey’ s test.
Age–smoking correlation on arterial stiffness
In a fully adjusted two-way ANCOVA analysis we observed a progressive decline in SBP amplification across the age groups (p=0.0002), with a significant difference between smokers and non-smokers (p=0.0001) and a borderline significant interaction between smoking and age group (p=0.07) (Figure 3). The age–smoking interaction reached the level of statistical significance after inclusion of mean BP in the fully adjusted model (p=0.05). Smokers in the first and second age groups presented similar SBP amplification to that observed among non-smokers in the second and third age groups, respectively (Figure 3). Similar results were observed for PP amplification: it declined across the age groups (p<0.0001) and from non-smokers to smokers (p=0.005) with a borderline significant interaction between smoking and age group (p=0.073); the inclusion in the model of mean BP did not change the level of statistical significance. No interactive effect was observed between smoking group and coffee or alcohol consumption (data not shown).
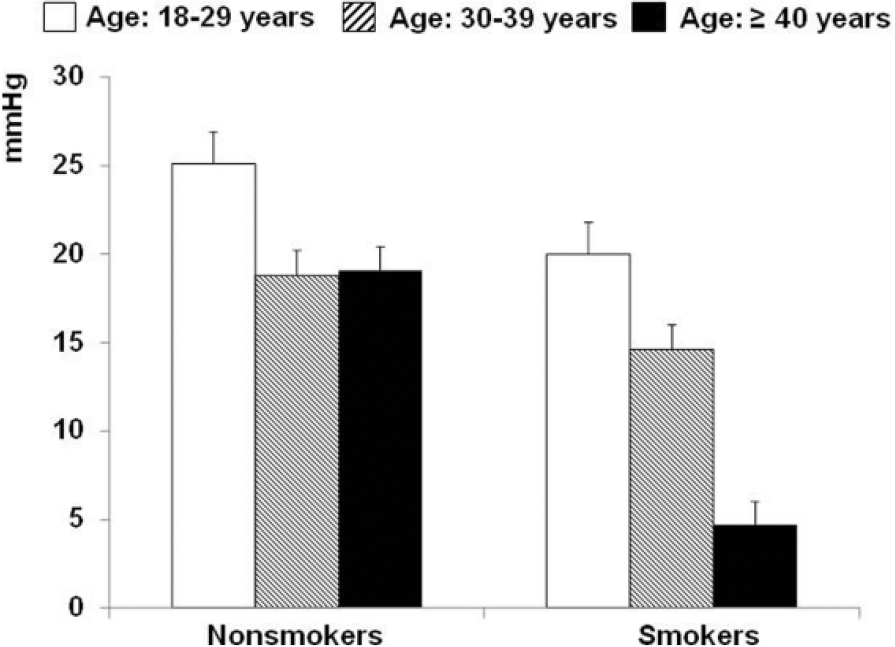
Systolic blood pressure amplification according to age and smoking groups (yes/no). Two-way ANCOVA analysis. The p-value is adjusted for sex, BMI, heart rate (HR), lifestyle habits and parental hypertension. According to age group p=0.0001, smoking group (non-smokers vs smokers) p=0.0002, interaction (smoking*age group) p=0.069. After inclusion of mean arterial pressure in the model, p<0.0001 for age group, p=0.0002 for smoking group, p=0.05 for interaction (smoking*age groups).
Discussion
We found that smoking increased central BP in young-to-middle age stage I hypertensives and accelerated the age-related decline in BP amplification. The effect of smoking on BP amplification was comparable to that of being 10 years older. This suggests that smoking contributes to accelerating the age-related stiffening of the arterial wall in hypertension. The higher central BP and the lower BP amplification found in our hypertensive smokers indicates an earlier reflected wave return to the aorta during the cardiac cycle in smokers, in agreement with previous results obtained in different populations. 24 Mahmud et al., 2 examining the acute and chronic effect of smoking in young healthy subjects, observed that smokers had higher central SBP and AIx, and lower PP amplification. The same results were observed by Tabara et al. examining patients from a general population. 25 Several mechanisms can account for the increased arterial stiffness in smokers. Nicotine stimulates epinephrine release and sympathetic nervous system activity. 26 However, this effect was not apparent in our smokers in whom urinary epinephrine was increased only marginally. This may be because young hypertensive subjects already have a chronically activated simpatho-adrenergic system.27,28 The increased arterial stiffness in smokers may be due to other humoral factors not measured in the present study. In the literature, increased release of thromboxane A2, which has a powerful vasoconstrictive effect, 29 and inhibition of nitric oxide release with impairment of endothelial vasodilation have been described in smokers. 30 The accumulation of active oxygen and free radicals during smoking, which results in chronic oxidative stress, is another possible mechanism leading to endothelial dysfunction, 31 vasoconstriction and vascular inflammation. 32 In addition, the carbon monoxide contained in cigarette smoke binds to blood haemoglobin and stimulates cholesterol degeneration, which impairs endothelial function and stimulates of atherosclerosis. 33
Of note, in our study there were more coffee drinkers among the smokers than the non-smokers. Previous studies have shown an interaction of caffeine and smoking on BP and on cardiovascular risk.34 –37 Vlachopoulos et al. observed that smoking and coffee intake combined had unfavourable effects on aortic stiffness and wave reflections. 38 In the present study, results were adjusted for coffee consumption but we cannot exclude that coffee potentiated the detrimental effects of smoking on arterial elasticity, especially in low caffeine metabolizers. 39
Study limitations
In this analysis, central SBP was not directly measured but was estimated from non-invasive pressure waveforms with applanation tonometry. A potential pitfall of this technique is that the values for central BP depend on the validity and applicability of the generalized transfer function used to generate the central aortic waveforms. In addition, the calibration of central aortic pressures depends on the accuracy of the brachial BP measurements. However, the transfer function used by the DAT system to derive central BP has been validated in several studies which showed a good correspondence between calculated and directly recorded central aortic BP. 23
The second limitation is the higher prevalence of male subjects in our population, due to the effect of the natural selection in this age range. Because of the small number of female hypertensives, we must be cautious about conclusions in this gender.
The third limitation regards suboptimal smoking exposure data. Unfortunately, we did not have data regarding how long patients have been exposed to smoke, changes on smoking habits during follow-up or second-hand smoking. However, a previous paper by Winnicki et al. demonstrated that during 6 years of follow-up the changes in smoking status were −0.5% in the HARVEST participants. 40
Finally, because this is a cross-sectional analysis our findings should be confirmed in a prospective longitudinal study.
Conclusion
Smoking has many negative effects on human health. The present results suggest that in young-to-middle age subjects, in the initial stage of hypertension, cigarette smoking accelerates the age-related decline of BP amplification leading to increased arterial stiffness. Young hypertensive patients should be vigorously and persistently encouraged to stop smoking, to avoid the acceleration of arterial stiffening and prevent vascular dysfunction.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the study was funded by the University of Padova, Padova, Italy and by the ‘Associazione 18 maggio 1370’, San Daniele del Friuli, Italy.