
Abstract

Increased carotid intima–media thickness (cIMT) serves as an indicator of early atherosclerosis, 1 but it may stem from increased intima layer thickness (cIT), a more precise atherosclerosis marker, or media layer thickness (cMT), predominantly comprising vascular smooth muscle cells (VSMC).2 –4 Elevated blood pressure (BP) is strongly related to greater cIMT, 5 but whether BP-related cIMT remodeling is mediated by cIT, cMT, or both is not established.2,3 Pulse pressure amplification leads to higher systolic peripheral BP (PBP) values when compared to central BP (CBP). This may explain why studies indirectly assessing CBP reported a stronger accuracy to detect high cIMT than PBP. 6 Currently, it remains uncertain whether this association’s strength is attributed to increased cIT or cMT. To address these questions, our study aimed to validate whether invasively measured CBP exhibits greater accuracy in detecting increased cIMT compared to PBP and to identify the primary carotid wall layers responsible for driving this association.
This study evaluated cIMT, cMT, cIT, PBP, and CBP in a convenience sample of 97 consecutive individuals aged ⩾ 18 years referred for elective coronary angiography in the Clinics Hospital of the State University of Campinas. CBP was measured directly in the ascending aorta with the patient in a supine position using a low-compliance fluid-filled catheter. PBP was calculated as the average of two brachial BP readings performed with a 1-minute interval using a HEM-7113 device (Omron, Kyoto, Japan) with appropriate cuff sizes, concomitantly to CBP measurement. High-resolution images of both common carotid arteries 2 cm proximal to the carotid bifurcation were obtained immediately before cardiac catheterization by a physician (DSSM) using a Vivid q ultrasound device (General Electric, Milwaukee, WI, USA) equipped with a linear transducer (12L-RS; 6–13 MHz) set at 10 MHz, as previously described. 2 Five measurements of cIT, cMT, and cIMT in plaque-free areas were manually performed using ImageJ software (NIH, Bethesda, MD, USA) for each image and the thickness of the layers corresponded to the average of left and right carotid measurements (online supplemental Figure 1). 2 The protocol was approved by the State University of Campinas Ethics Committee and all participants provided written consent. Significance was considered for p < 0.05.
The sample (n = 97; 61% men, age = 61.4 ± 10.5 years) had mean values of systolic PBP and CBP and diastolic PBP and CBP of 144.5 ± 28.3, 140.5 ± 29.3, 83.5 ± 14.7, and 78.7 ± 16.0 mmHg, and average values of cIT, cMT, and cIMT of 0.222 ± 0.048, 0.511 ± 0.137, and 0.733 ± 0.159 mm, respectively (online supplemental Table 1). Univariate linear regression analysis only showed a direct association of age with cMT and cIMT (both p = 0.001) and between cIT and hypertension (p = 0.010). Multivariable linear regression analysis adjusted for age and sex showed no association between any BP measurement and carotid layers. Conversely, restricted cubic spline analysis adjusted for age and sex showed an inverted U-shaped relationship of systolic CBP and cMT (overall p = 0.047; p for nonlinearity = 0.020) and cIMT (overall p = 0.025; p for nonlinearity = 0.008) with a peak at CBP values of 150–160 mmHg (Figure 1). Additionally, adjusted restricted cubic spline analysis showed no association of any carotid layer with systolic PBP (Figure 1), diastolic CBP, or PBP, and pulse pressure derived from CBP or PBP measurements (all p > 0.05).
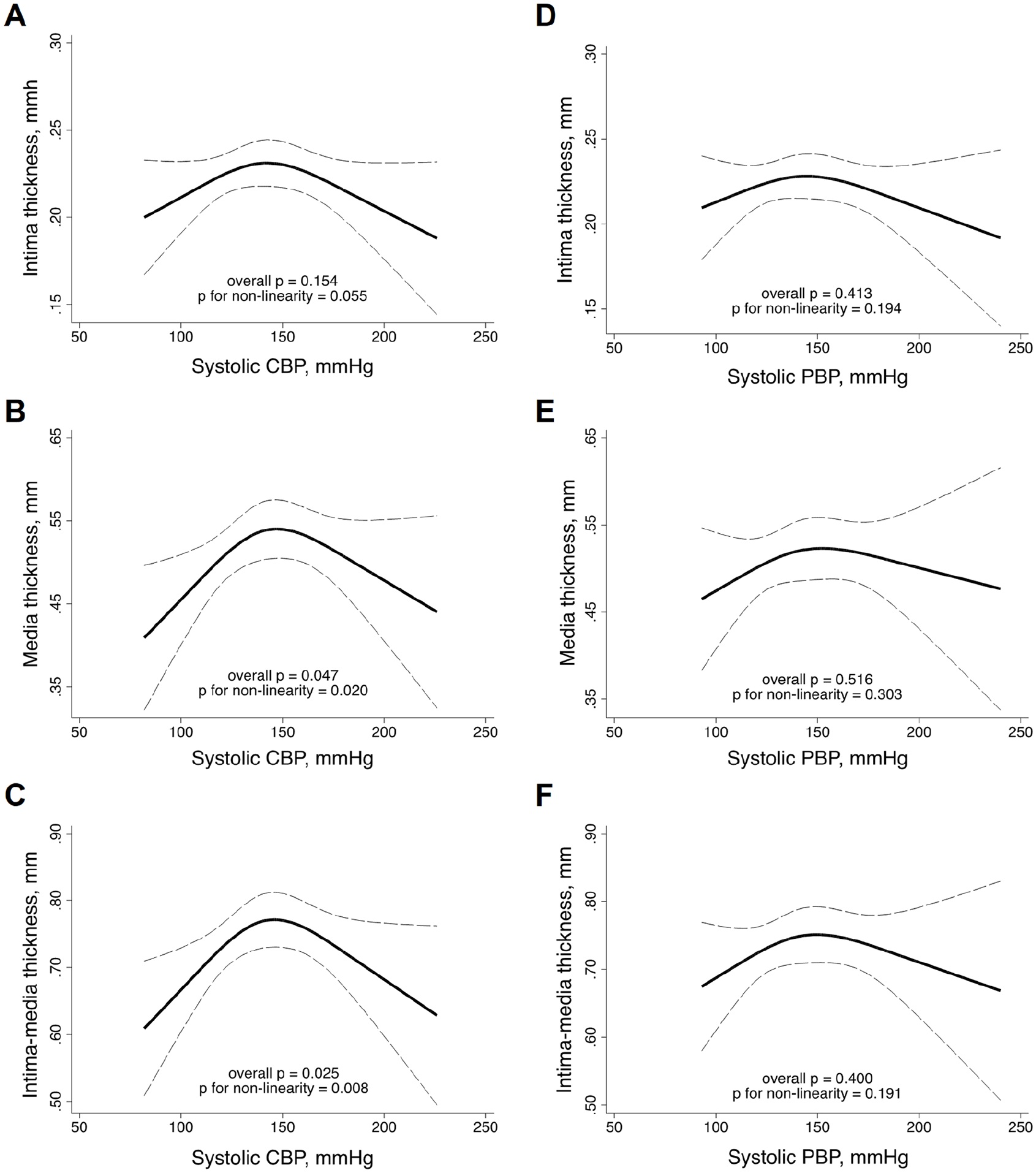
Relationship between carotid wall layers and systolic blood pressure measurements evaluated by restricted cubic splines with three knots adjusted for age and sex.
This study provided novel evidence that the relationship between cIMT and CBP was mediated by variation in cMT and that cIMT and CBP had an inverted U-shaped relationship, with a peak at systolic CBP values of 150–160 mmHg. These findings might have clinical implications. First, they indicate that cMT, which is majorly comprised by VSMC, is more sensitive to pressure load than cIT, 4 and supports the notion that BP-induced variation of cIMT may not reflect atherosclerosis burden. Second, they suggest that cIMT might not be an accurate marker of vascular remodeling under high aortic pressures. In agreement with this assumption, a former longitudinal study demonstrated that cIMT progression tends to decrease at systolic CBP levels > 150 mmHg. 7 Potential explanations for such nonlinear association could be that, at high CBP values, the cIMT may become more compacted and thinner, as previously suggested by studies evaluating cIMT variation during the cardiac cycle, 8 or could exhibit a saturating hypertrophic response to mechanical stress. 9 Furthermore, the nonlinear relationship may also help explain the lack of independent association between CBP and cIMT when assessed by conventional linear or logistic regression analysis in some studies. 6
Our study has limitations. Owing to the cross-sectional design, a causal relationship between BP and carotid remodeling cannot be inferred. Furthermore, BP was measured only at a single time point. Conversely, data on lean mass were not available, limiting our ability to assess the reported association of muscle mass with cIMT and cMT. 10
In conclusion, we demonstrated that CBP has an inverted U-shaped relation with cIMT and cMT, but is not related to cIT, suggesting that cIMT may not be an accurate marker of pressure overload-induced carotid atherosclerosis. Further studies are necessary to evaluate the value of cMT and cIT in predicting cardiovascular events.
Supplemental Material
sj-docx-1-vmj-10.1177_1358863X241238708 – Supplemental material for Association between carotid wall layers and invasively measured central blood pressure
Supplemental material, sj-docx-1-vmj-10.1177_1358863X241238708 for Association between carotid wall layers and invasively measured central blood pressure by Daniel SS Mello, Silvio Gioppato, Diego Q Antoniassi, Demétrio CS Vieira, Pedro HA Matos, Silvério A Fernandes, Otavio R Coelho-Filho, Roberto Schreiber, Rogério TP Okawa, Andrei C Sposito, José R Matos-Souza and Wilson Nadruz in Vascular Medicine
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by CNPq (grant 310869/2021-8) for Dr Nadruz.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.