
Abstract
Fibromuscular dysplasia (FMD) is a non-atherosclerotic, non-inflammatory disease of medium sized arteries that has been described in multiple anatomic territories with a wide variety of manifestations (e.g. beading, stenosis, occlusion, aneurysm, or dissection). While the first case of FMD is thought to have been described over 75 years ago, the causes, natural history, and epidemiology of FMD in the general population remain incompletely understood. This article reviews important historical and contemporary contributions to the FMD literature that inform our current understanding of the prevalence and epidemiology of this important disorder. A particular focus is given to studies which form the basis for FMD prevalence estimates. Prevalence estimates for renal FMD are derived from renal transplant donor studies and sub-studies of clinical trials of renal artery stenting; however, it is unclear how well these estimates generalize to the overall population as a whole. Newer data are emerging examining the genetic associations and environmental interactions with FMD. Significant contributions to the understanding of FMD have come from the United States Registry for Fibromuscular Dysplasia; however, many unanswered questions remain, and future studies are required to further characterize FMD epidemiology in general populations and advance our understanding of this important disorder.
Introduction
Fibromuscular dysplasia (FMD) is an arteriopathy which can affect arteries of all sizes that has been described in multiple anatomic territories with a wide variety of radiographic manifestations (e.g. beading, stenosis, tortuosity, occlusion, aneurysm, or dissection).1,2 It is most commonly found in the renal and extracranial carotid and vertebral arteries, 1 and while the first case of FMD is thought to have been described over 75 years ago, 3 the causes, natural history, and epidemiology of FMD in the general population remain incompletely understood. In the recent Scientific Statement from the American Heart Association on FMD, determination of the prevalence of FMD in the general population is at the top of the list of research priorities for FMD. 4 This present article reviews important historical and contemporary contributions to the FMD literature that inform our current understanding of the prevalence and epidemiology of this important disorder.
The basis for FMD prevalence estimates come from four principal sources: (1) studies of candidates for renal transplant donation, (2) sub-studies of renal stent/intervention trials, (3) cerebral angiography studies which evaluated consecutive patients, and (4) autopsy series. More recent understanding has also come from the United States Registry for Fibromuscular Dysplasia, which in 2012 published results from the first 447 enrolled patients. 1
Renal transplant donor studies
Catheter-based angiography
The largest available literature to estimate the prevalence of FMD comes from studies focused on the incidental detection of FMD in living kidney donor candidates. Key features from eight published studies are summarized in Table 1.
Renal transplant donor studies examining fibromuscular dysplasia (FMD) prevalence.
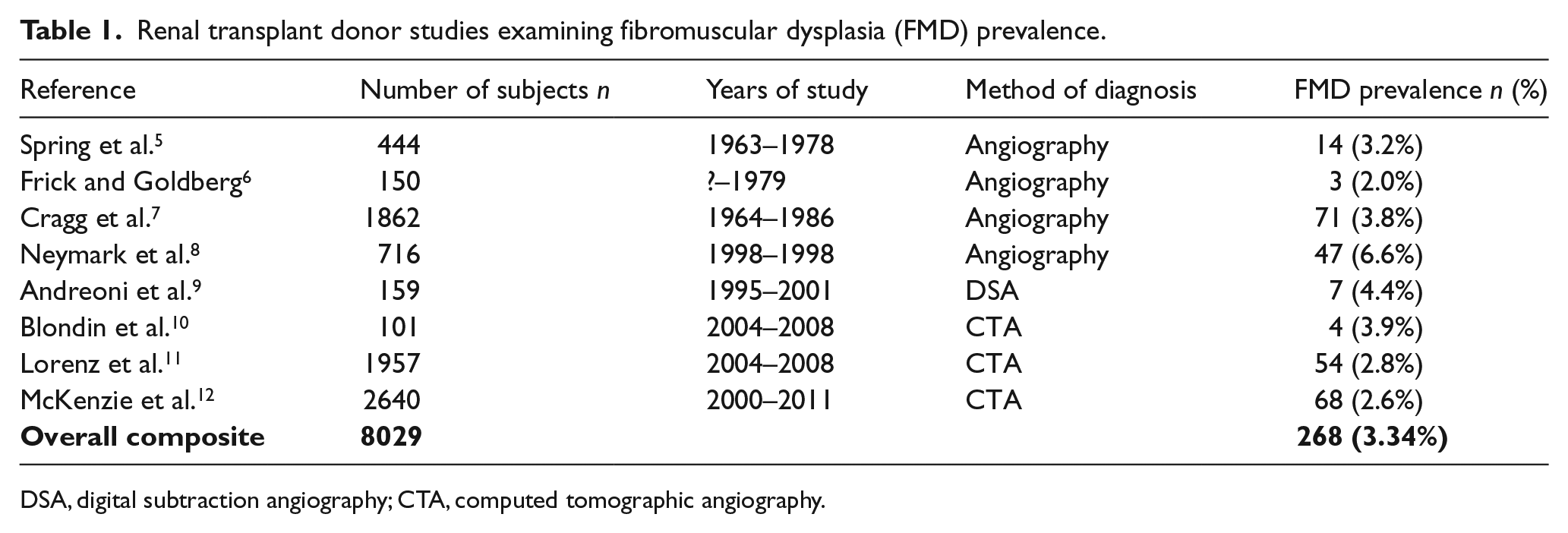
DSA, digital subtraction angiography; CTA, computed tomographic angiography.
The first major study to report FMD rates among prospective kidney donors was published in 1979. Spring and colleagues evaluated the aorto-renal angiograms of all prospective related donors at the University of California – San Francisco (UCSF) from December 1963 to March 1978. Out of the 444 reviewed studies, FMD was present in 14 for a prevalence of 3.2%. 5 Similarly, the Mayo Clinic experience of consecutive renal arteriograms from living related renal donor candidates was published in 1980. All patients in this cohort had no history of prior renal disease, normal physical examinations, normal blood pressure, and normal basic laboratory studies (e.g. normal blood urea nitrogen, creatinine, 24-hour urine creatinine clearance, and urinalysis). Out of 151 consecutive donor candidates, 150 underwent semi-selective renal angiography and three cases of ‘mild fibromuscular dysplasia’ were identified for a prevalence of 2.0%. 6
The first multicenter FMD prevalence data from potential living renal donor candidates were reported in 1989 along with long-term clinical follow-up. Data from 1862 subjects with renal angiograms performed at the Universities of Iowa, Minnesota, California – San Francisco, California – Los Angeles, and the Mayo Clinic from 1964 to 1986 were pooled. Of the 1862 studies, 1854 were available for panel review and were graded for ‘severity’ of FMD using degrees of angiographic stenosis. They identified 71 cases of FMD among their pool of potential renal donors, for a prevalence of 3.8%. 7 Of note, this cohort included the angiograms from UCSF and Mayo Clinic previously published in the articles described above.5,6
The most contemporary study cohort of healthy renal donor candidates undergoing traditional invasive renal angiography includes 716 subjects from April 1988 to March 1998. Forty-seven of these subjects were found to have renal FMD (6.6%). This rate is notably higher than all other previously and subsequently published reports. An important distinction in the methodology of this study compared with the publications described above is that only angiograms previously reported as abnormal were reviewed. Further, of the 78 angiograms whose dictated reports identified an abnormality, only 64 of the films were available to be retrospectively reviewed. It is noted that the retrospective interpretation agreed with the original dictated report in 61 of the 64 available cases; however, it is not reported what percentage of the cases identified as FMD were available for review or whether any FMD cases were among those of disagreement in interpretation. 8
In 2002, Andreoni and colleagues published the only large cohort of healthy renal donor candidates evaluated with digital subtraction angiography (DSA). From July 1995 to June 2001, 159 donor candidates who underwent selective bilateral renal artery DSA studies were reviewed. Seven cases of renal FMD were identified, for a prevalence of 4.4%. 9
Non-invasive angiography
More recent evaluations of potential renal donor candidates employ non-invasive computed tomographic angiography (CTA) in place of invasive angiography. In a sample of 101 healthy living kidney donors between July 2004 and September 2008, Blondin et al. identified four cases of FMD (3.9%) which were confirmed by histopathology following transplant. This is a notable contribution as it is one of the only studies to compare non-invasive imaging against surgical pathology. The authors note that three cases were detected by their 64-detector-row CTA protocol, while one case of a ‘mild form of FMD’ could not be detected even upon retrospective review (75% sensitivity in their small sample). 10
The first large contemporary report of the prevalence of FMD from CTA evaluation of healthy prospective kidney donors included 1957 potential donors from March 2000 to July 2008 at Mayo Clinic. Among this cohort, 54 cases of FMD were identified (2.8%) from review of scan reports (retrospective review of images was not performed in this study). The authors do note that the CTA scanning technology and protocols at their institution evolved during the 9-year study period, but that there were no significant differences in prevalence estimates across the two periods (2000–2005 and 2005–2008). 11
In 2013, additional data from this same kidney donor population at Mayo Clinic was published, expanding the scope of the retrospective review from January 2000 to December 2011. The updated report included 2640 potential renal donors and, in contrast to the prior publication, independent readers reviewed all of the scans whose initial dictated reports cited FMD or one of a number of search terms they associated with the condition (e.g. ‘bead’, ‘string’, ‘pearls’, etc). They confirmed 68 cases for a prevalence of 2.6% in their renal donor population. Notable limitations of this work include that the only CTA images retrospectively reviewed were those cases originally reported as FMD and that none of the cases were subsequently evaluated with DSA or traditional angiography. 12
Taking all of these studies together, FMD is present in approximately 3–4% of the overall kidney donor population. An important limitation of this data is that it may not generalize to the population as a whole. Some have suggested that many kidney donors likely have a family member with severe renal disease, which may enrich for a familial FMD population and lead to overestimates of prevalence. Conversely, others have suggested that healthy renal donor candidates often have few comorbid health conditions (and by definition often lack pre-existing hypertension or renal disease), and therefore may underrepresent FMD prevalence in a general population.
Sub-studies of clinical trials
Another methodology used to gain insight into the prevalence of FMD is retrospective evaluation of large clinical trial populations. The Cardiovascular Outcomes in Renal Atherosclerotic Lesions (CORAL) trial13,14 was a randomized, multicenter clinical trial comparing optimal medical therapy versus renal artery stenting plus optimal medical therapy in patients with atherosclerotic renal artery stenosis. Inclusion criteria consisted of patients aged 18 years or older with either documented hypertension (systolic > 155 mmHg) on greater than two antihypertensive medications or with chronic kidney disease. Trial patients underwent conventional renal angiography which was later reviewed by a blinded angiographic core lab (ACL). Of note, an exclusion criterion for enrollment into the CORAL trial was the presence of renal artery FMD and of the 4375 patients initially screened for the trial, 87 were not enrolled due to the presence of FMD. Of those who were enrolled and underwent angiography, the presence or absence of FMD for each catheter-based angiogram was adjudicated by two interventional radiologists and recorded in the ACL database. Of 995 CORAL participants who underwent renal angiogram, 58 were noted to have incidental renal FMD (5.8% overall prevalence). Of the 58 found to have FMD, 44 were female and 14 were male; thus, the prevalence of FMD in the female population was 8.6% while it was only 2.8% among males. The CORAL population had notable differences from the healthy renal donor populations previously described in that it consisted of older subjects with a higher prevalence of hypertension, atherosclerotic disease, and/or kidney disease. 14
Cerebral angiography studies
Recent publications have demonstrated that cerebrovascular FMD occurs nearly as frequently as renal FMD; 1 however, there are even fewer published primary data available examining its prevalence in the general population. There are multiple factors for this: (1) pathologic specimens from the cerebral arteries are infrequently obtained in the course of routine clinical care and (2) conventional invasive cerebral angiography is rarely performed, even in patients with symptoms or known cerebrovascular diseases. A study by Mettinger and Ericson reviewed 4000 consecutive cerebral angiograms performed at Karolinska Hospital in Stockholm, Sweden from 1970 to 1978 and identified 37 patients with cerebral FMD (0.9% prevalence). 15 Other smaller studies reviewed by Touze and colleagues demonstrated that the prevalence of cerebrovascular FMD in patients undergoing cerebral angiography ranges from 0.3% to 3.2%. 16 It is notable that in each of these studies, patients were undergoing invasive cerebral imaging for symptomatic disease and/or major risk factors and therefore likely do not accurately represent the general population.
Autopsy series
The methodology which may offer the most insight into the prevalence of FMD in the general population is autopsy studies of consecutive patients. The first such study to report FMD findings was from the Mayo Clinic and identified nine patients with renal FMD out of a cohort of 819 consecutive autopsies at their institution. These data were only ever published in abstract form in 1970, and further details (such as rates of cerebrovascular FMD) were not included. 17 The largest autopsy series to date was later published by the Mayo Clinic in 1996. Schievink and colleagues reviewed 20,244 consecutive autopsies and found histopathologic FMD in only four patients (0.02%). Interestingly, all were cases of internal carotid FMD. 18 A notable limitation of these autopsy studies is that standard autopsies rarely sample distal internal carotid artery (ICA) segments and FMD usually spares the more commonly sampled proximal segments; therefore the true prevalence of cerebrovascular FMD is likely underestimated in these series.
Key findings from the US FMD Registry
In 2008, the United States Registry for Fibromuscular Dysplasia (US FMD Registry) was established. In 2012, Olin and colleagues published a report of the first 447 patients enrolled from the nine participating sites. 1 This represents the largest published cohort of FMD patients and offers unique insights into the contemporary epidemiology of FMD in the US. The vascular imaging obtained for Registry participants was guided by clinical presentation and local/institutional practices.
The anatomic distribution of vascular involvement in the US FMD Registry was one of its most interesting findings and did not follow smaller, previously published reports that had suggested that renal FMD was much more common than cerebrovascular FMD. Of the 447 patients enrolled, 342 had cerebrovascular imaging and 374 had renal and abdominal vascular imaging. There were 294 out of 369 Registry patients with renal artery FMD (79.7%) and 251 out of 338 with extracranial carotid artery FMD (74.3%). The authors suggest that improved non-invasive imaging techniques and more thorough screening for the extent of disease involvement in FMD patients may account for the higher rates of cerebrovascular FMD in Registry patients than in previously published cohorts. Because not all vascular territories were imaged in all patients, it was not possible to determine the prevalence of FMD in multiple sites for the whole cohort. The vast majority of imaging in both groups was non-invasive (ultrasound or CTA), and histopathologic confirmation of FMD was only available in 14 patients (3.3%).
The US Registry also offered important insights regarding the contemporary demographics of FMD in the US. Consistent with prior published cohorts, the mean age at diagnosis was 55.7 years (range 5–83 years) with a strong female predominance (91% female). Of 414 patients, 395 were Caucasian (95.4%), nine were African American (2.2%), six were Hispanic (1.5%), and two were Asian (0.5%). Conclusions of FMD prevalence estimates based on race must be viewed cautiously, however, as there is likely to be a referral bias of patients who are able to be seen at FMD Registry centers. Out of 395 patients for whom data were available, 147 were current or former smokers (37.2%). Out of 293 female patients, 204 (69.6%) had either current or a history of exposure to oral contraceptives or hormone replacement therapy at the time of enrollment into the FMD Registry.
Patients in the Registry self-reported family history data for their first- and second-degree relatives. Only 26/354 (7.3%) reported a confirmed diagnosis of FMD in a family member. However, there were varying rates of other conditions reported which can be associated with or considered manifestations of FMD. Out of 303 FMD patients responding, 60 reported a family history of sudden death (19.8%), 175/327 (53.5%) reported a family history of stroke, 76/323 (23.5%) reported a family history of aneurysm, and 6/303 (2.0%) reported a history of arterial dissection.
There were 25 patients (5.6%) who were asymptomatic at the time of diagnosis, whose FMD was found either when imaging was performed for another indication or following the evaluation of a bruit on routine physical examination. These patients further support that FMD reflects a broad spectrum of disease and suggests that there is likely a substantial number of patients with undiagnosed silent FMD.
The FMD Registry reported the prevalence and vascular distribution of arterial dissections and aneurysms in patients with FMD. Dissection was present in 88/447 (19.7%) of cases, and manifested in a wide range of arterial territories. Of the 88 patients with dissections, there were 68 carotid (77%), 19 renal artery (21.6%), 15 vertebral artery (17.0%), four mesenteric (4.5%), three coronary (3.4%), two celiac (2.3%), and two iliac artery dissections (2.3%) (all vascular beds were not imaged in every patient and patients may have had dissections in more than one territory). Similarly, aneurysms were present in 76/447 patients (17%) and represented the same wide range of arterial territories (the most common examples included renal 32.9%, carotid 21.1%, aortic 19.7%, and cerebral 11.8%).
In separate reports, investigators have found high prevalence rates of FMD among those who present with a primary vascular event. In patients who present with spontaneous cervicocephalic dissection (cranial and cervical arteries), FMD is the most common association and is present in approximately 20% of cases. 4 In patients presenting with spontaneous coronary artery dissection (SCAD), two independent single-center registries from large referral centers both found an FMD prevalence of 45%,19,20 while a third cited an FMD prevalence as high as 86% among its SCAD patients. 21 Further investigation is needed to better understand the relationship between these conditions and FMD.
In a sub-study from the US Registry data, the clinical presentation and outcomes of patients stratified by gender were examined and found that men were more likely to have focal disease and were more likely to present with visceral involvement than women. Male FMD patients in the US Registry had a twofold higher prevalence of arterial aneurysm and arterial dissection when compared with female Registry patients. These findings suggest that FMD may have a more aggressive course with higher rates of renal and mesenteric artery involvement in men compared to women. 22
Genetics of FMD
The genetics underlying FMD represent an emerging area of research. To date, no causative genes have been definitively identified; however, published case reports of FMD in identical twins and sibling pairs suggest there may be underlying inheritability. 23 Early pedigree analyses performed in the 1970s and 1980s suggested FMD may follow an autosomal dominant pattern with variable penetrance.24,25 Rushton and colleagues presented a series of 20 FMD patients and classified 60% as familial. 24 An important limitation of these findings is that few family members underwent definitive confirmation of FMD by imaging, but rather were classified by interviews and reports of having clinical cardiovascular events or early-onset hypertension. Therefore, this study may have significantly overestimated the true FMD prevalence among family members. In more recent studies with imaging confirmation of FMD diagnoses, approximately 11% of FMD was classified as familial. 26 In a French study retrospectively reviewing 104 patients with imaging-confirmed FMD, all identified positive family members were siblings and no cases of vertical transmission were found. 26
There are only a few, limited studies examining molecular targets or specific genes. Sang and colleagues examined the role of autoimmunity in a case–control study of 33 patients with angiographically confirmed FMD. They found an association with human lymphocytic antigen (HLA) type DRw6 that was more common in FMD patients than in matched renal transplant donor control subjects or matched healthy ambulatory controls; however, this finding has not been subsequently replicated in other studies. 27
Case reports have described individuals with concurrent α1-antitrypsin (AAT) deficiency and FMD. In a larger series of 161 consecutive patients with angiographically confirmed FMD, three functional polymorphisms of the AAT gene were investigated using three control groups (hypertensive and normotensive patients). No differences were found in AAT genotype frequencies between the FMD and control groups, and further there was no correlation between the AAT genotypes and the clinical and angiographic characteristics of the FMD patients. 28
In 2001, Bofinger and co-investigators in Australia reported findings on several polymorphisms of the renin-angiotensin system in 43 patients with renal FMD and 89 matched controls. Allele frequencies did not significantly differ between the groups with the exception of the angiotensin-converting enzyme (ACE) I allele, which was found at a significantly higher frequency in renal FMD patients than in controls. The significance of this is not clear and the finding has not been confirmed in subsequent larger studies. 29
A recent 2015 case–control series published by Silhol and colleagues compared histologic findings from surgically removed renal arteries from six FMD patients (who underwent surgery for stenosis or aneurysm caused by FMD) and three controls (who underwent nephrectomy for non-vascular causes). 30 Immunohistochemical staining detected intense progesterone receptor expression in the nuclei of smooth muscle cells in the FMD patients, whereas no progesterone receptor expression was found in the control patients. There was no difference in estrogen receptor expression between the groups. Further validation of these findings is necessary in larger populations of patients to determine if progesterone receptors play a role in FMD pathogenesis.
At the 2015 American Heart Association Scientific Sessions, Kiando and colleagues presented in abstract format the results of the largest genetic association study conducted to date. They performed a genetic association study in European ancestry individuals (393 FMD cases and 2537 controls) and found that the FMD risk variant is intronic to the phosphatase and actin regulator 1 gene (PHACTR1), involved in angiogenesis and cell migration, and also known to be a risk locus for coronary artery disease, migraine, and cervical artery dissection. 31 This is the first report of a risk locus for FMD, and validation studies are anxiously awaited.
Given the overlapping features of FMD with well-characterized vascular connective tissue disorders such as Loeys-Dietz syndrome or Ehlers-Danlos syndrome-type IV (vascular subtype), different investigators have pursued genetic testing for these conditions in patients with confirmed FMD. In 2012, Poloskey and colleagues reviewed 216 consecutive FMD patients, of whom 63 were referred for genetic counseling with genetic testing performed in 35 (35/63; 55.6%). Two patients, both with a history of arterial dissection, were found to have distinct and novel variants of the transforming growth factor TGFβR1 gene, while no mutations were found in the other 33 patients. 32 A 2014 multicenter study by Ganesh and colleagues examined 47 patients with FMD; in their cohort, screening for known mutations associated with genetically mediated arteriopathies was unrevealing (zero pathogenic mutations identified out of 47 patients). 33 They did find statistically significant evidence of elevated plasma TGF-B1 and TGF-B2 levels as well as increased secretion of the same by fibroblasts derived from FMD patients when compared to matched controls; however, the significance of this remains unclear. Both groups concluded that there appears to be a very low yield for routine genetic testing of known vascular connective tissue disorders such as Loeys-Dietz or Ehlers-Danlos in patients with FMD.
Environmental interactions
Considerable attention has been given to a number of environmental factors which may be associated with FMD. The role of smoking in other vascular diseases is well established, and several studies have sought to clarify its role as a risk factor or disease modifier in FMD. Savard and colleagues reported data on 337 FMD patients matched to controls with primary (‘essential’) hypertension and found that the proportion of current smokers was significantly higher in the FMD group than in the matched controls. Active smoking was also strongly associated with a younger age of diagnosis for both hypertension and FMD in their cohort, suggesting that smoking may mediate more aggressive disease in certain susceptible individuals. 34 This replicated an earlier finding of Bofinger and colleagues who had examined 50 patients with angiographically confirmed FMD and conducted detailed smoking histories. Twenty-four of 50 patients were smokers and smoking was associated with an earlier onset and increased severity of FMD disease. 35 In a smaller study comparing 33 angiographically diagnosed FMD patients to 61 renal transplant donor control subjects and a second group of 934 ambulatory control subjects, Sang and colleagues similarly found higher rates of current or former smoking among patients with FMD. 27
Given the female predominance among patients diagnosed with FMD, attention has also focused on the potential influences of estrogen or other hormonal contributors. The study described above by Sang and colleagues was one of the first to attempt to identify gender-specific associations, and collected information on history of oral contraceptive use, age of menarche, number of pregnancies, spontaneous abortions, gynecological disorders, and hysterectomy for both FMD patients and matched controls. They did not find any significant differences between their groups for these characteristics, though were likely under-powered given the small sample sizes of their groups. 27
Concluding remarks
While our understanding of FMD has evolved considerably since its first description over 75 years ago, the causes, natural history, and epidemiology of FMD in the general population remain incompletely understood. Our current estimates of FMD prevalence are based on studies of candidates for renal transplant donation, sub-studies of renal stent/intervention trials, cerebral angiography studies which evaluated consecutive patients, and autopsy series, each with their own limitations when trying to generalize to the population as a whole. The largest published data come from evaluation of healthy candidates for renal transplant donation, and in that population the prevalence of FMD is consistently 3–4%. The currently available evidence supports a consensus that FMD is likely a multifactorial disease with some contribution from genetic, environmental, and possibly hormonal/gender-specific influences. While there appears to be some association with smoking and FMD onset and severity, the literature has not yet established a clear link with hormonal or genetic factors, beyond the known overwhelming female predominance of the disorder. Future studies are required to further characterize FMD prevalence in general populations and advance our understanding of the causes and genetics of this important disorder.
Footnotes
Dr. Jeffrey Olin served as guest editor for this manuscript
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.