
Abstract
Fibromuscular dysplasia is an uncommon non-inflammatory arteriopathy. Hormonal factors are believed to play a role in disease pathogenesis given the overwhelming female predominance of this disease. We describe a case of a 56-year-old transgender man on prolonged testosterone therapy diagnosed with renal fibromuscular dysplasia after presenting with hypertensive urgency.
Introduction
Fibromuscular dysplasia (FMD) is an uncommon, non-inflammatory vascular disease. It is recognized by the National Organization for Rare Disorders (https://rarediseases.org/), but has also been reported to have a prevalence of 2.0%–6.6% based on studies involving potential healthy renal transplant donors. 1 Increased use of computed tomographic angiography (CTA) and magnetic resonance angiography (MRA) has led to increased identification of vascular aneurysm and dissection among patients with FMD, allowing for early counseling on modifiable risk factors and selection of treatment options and surveillance protocols. 2 Although the exact pathogenesis of FMD remains unknown, several studies have identified hormonal, genetic, and environmental factors, such as cigarette smoking, as potential etiologic factors.3,4 One pilot study by Silhol et al. 5 that studied renal artery specimens of patients with FMD requiring nephrectomy demonstrated that progesterone receptor expression was higher as compared with specimens from controls without FMD who underwent nephrectomy for other, non-vascular causes. Hormonal factors, such as progesterone receptor density and estrogen exposure, may contribute to the marked predominance of the female sex in FMD prevalence and are discussed in this case report of a transgender male diagnosed with FMD. The patient presented consented to this publication and use of the included images.
Case presentation
A 56-year-old Caucasian transgender man presented to the emergency department (ED) three times over the course of a week with blood pressures ranging from 180 to 220s/140 to 150s mmHg and a chief complaint of headache. The patient did not have a known history of hypertension and had previously received regular medical care. The headache was bitemporal in location and was similar to his chronic tension headaches. He had no other presenting symptoms, including chest pain or vision changes. The patient had been started on oral amlodipine at a prior ED visit and was taking this medication. Upon ultimate admission to the hospital, physical examination findings included blood pressure 207/136 mmHg with pulse 105 bpm, absence of cervical bruits, normal cardiac and vascular examination, equal bilateral upper extremity blood pressure measurements, and normal peripheral pulses. He had no abdominal striae, abdominal bruits, or lower extremity edema. He was admitted for additional evaluation and treatment of hypertensive urgency.
His medical history was significant for dyslipidemia, hypothyroidism, and nicotine dependence (1/2 pack-per day cigarette smoker). Born a biological female, he underwent gender reconstruction surgery, including bilateral mastectomy, oophorectomy, and hysterectomy at age 29. He had been on oral/topical testosterone therapy since age 18 and was under the care of a primary care physician and endocrinologist.
Electrocardiogram was significant for left ventricular hypertrophy and chest radiography was negative for a widened mediastinum or other acute processes. Urine drug screen was negative for cocaine. Thyroid-stimulating hormone, urine and serum aldosterone, and morning cortisol were within normal limits. Serum potassium was 4.9 mmol/L, serum sodium 136 mmol/L, and creatinine 1.20 mg/dL. Hormone levels were not obtained. Given concern for an underlying secondary cause of his hypertensive urgency, a renal duplex ultrasound was performed and demonstrated severely increased velocities (Figures 1 and 2) in the right mid-to-distal renal artery (highest peak-systolic velocity 501 cm/s, end-diastolic velocity 246 cm/s, renal/aortic ratio 7.6). The right kidney measured nearly 2 cm smaller than the left (8.6 cm vs 10.5 cm). There was no hemodynamically significant stenosis of the left renal artery. A CTA of the abdomen and pelvis (Figures 3 and 4) demonstrated beading of the mid segment of the right renal artery with mild atrophy of the right kidney, suggestive of FMD. The CTA also revealed multiple other arteries with ectasia or aneurysm, including the splenic artery, hepatic artery, and bilateral internal iliac arteries. At a previous ED visit for hypertension and headache, he had undergone an MRA of the head and neck, which did not show any findings of FMD in the intracranial arteries, though a moderate atherosclerotic carotid stenosis in the right internal carotid artery was seen. Carotid duplex ultrasound demonstrated plaque and associated 50%–69% stenosis of the right internal carotid artery and <50% stenosis of the left internal carotid artery without evidence of mid to distal velocity increase suggestive of FMD. Transthoracic echocardiogram was significant for left ventricular ejection fraction of 60% with left ventricular concentric remodeling.

Renal duplex ultrasound of the right kidney. Peak systolic velocity notable for 501.3 cm/s with an end-diastolic velocity of 245.9 cm/s.
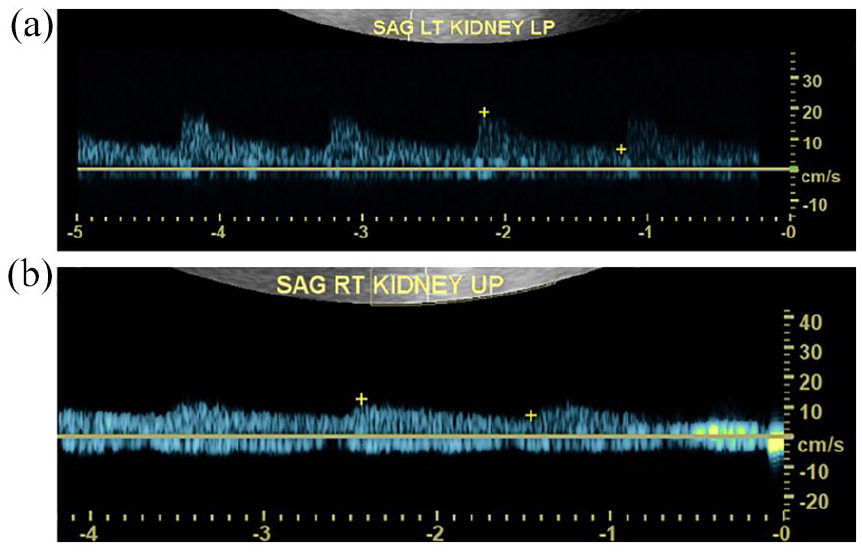
Renal duplex ultrasound of bilateral kidneys. Appreciable blunting of wave forms in the right kidney (Panel a) in comparison to the left kidney (Panel b).

CT angiogram of the abdomen/pelvis revealed significant beading of the mid right renal artery (solid white arrow), as well as ectasia of the right iliac and hepatic arteries (unfilled arrows).

CT angiogram of the abdomen/pelvis with demonstration of the classic “beads on a string” appearance of the mid right renal artery.
The patient was continued on amlodipine and was started on oral captopril, which was gradually titrated up for a goal blood pressure of <150/90 mmHg. Vascular medicine was consulted and plans were made for elective angiography and intervention on an elective basis since blood pressure was adequately controlled within 1 month’s time. He was discharged home on oral lisinopril, amlodipine, aspirin, and atorvastatin and was counseled on smoking cessation. Approximately 3 weeks later, he underwent elective angiography and intervention of the right renal artery. Angiography demonstrated multifocal FMD of the right renal artery with severe stenosis confirmed by intravascular ultrasound (IVUS) and optical coherence tomography (OCT; Figures 5 and 6). Serial balloon dilations were performed using 3.0 and 4.0 mm balloons with good angiographic result and no dissection or perforation (Figure 5). Prior to angioplasty, OCT of the right renal artery revealed circumferential fibrotic tissue at the stenotic lesions, consistent with FMD pathology (Figures 6 and 7). He was discharged home and required only amlodipine for blood pressure control at follow-up. Dual-antiplatelet therapy with aspirin 81 mg and clopidogrel 75 mg was prescribed empirically for 3 months at the discretion of the interventionalist, followed by aspirin 81 mg alone, and the patient was continued on atorvastatin 80 mg given atherosclerotic carotid disease.
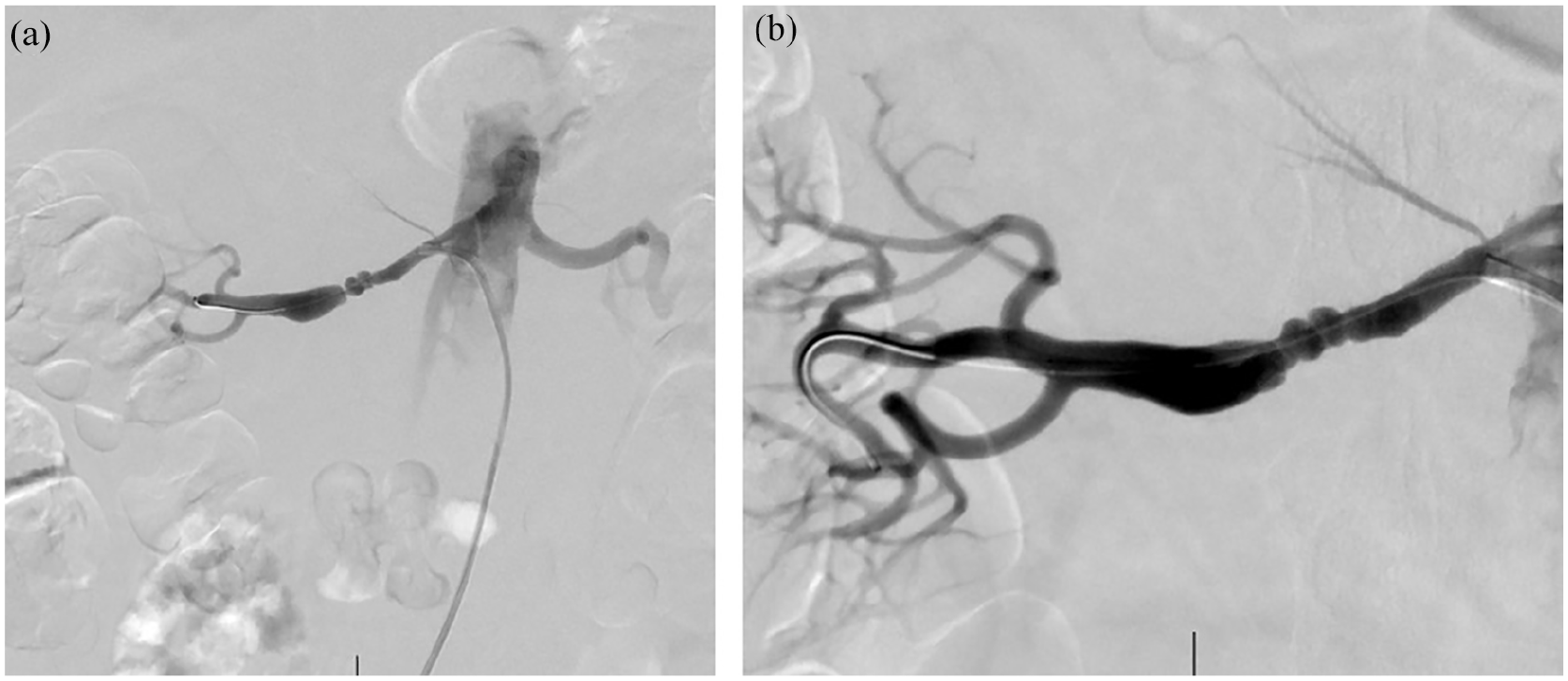
Right renal artery angiography (a) before and (b) after serial balloon dilations. Image (a) demonstrates the significant narrowing of the mid-artery.

Lumen profile of the right renal artery with optical coherence technology (OCT). Demonstration of multiple sequential sections of luminal narrowing consistent with FMD.

OCT of the right renal artery with demonstratable narrowing of the lumen.
IVUS and OCT-guided percutaneous transluminal angioplasty was the elected management option for this patient, in the setting of pharmacologic adjuvants until the time of intervention. One month following balloon angioplasty, blood pressure was controlled on amlodipine and a repeat duplex ultrasound following the angioplasty demonstrated improvement of velocities in the right renal artery. He is under the care of a vascular medicine specialist and his extra-renal beaded and aneurysmal segments will be monitored along with his renal arteries. At follow up of 10 months after the procedure, he remained on amlodipine alone with good blood pressure control, although renal duplex showed slight elevation in velocities within the right renal artery.
Discussion
Here, we present the case of a transgender male patient diagnosed with FMD after presenting with hypertensive emergency. Only one other instance of FMD reported in a transgender patient was found in the literature. Shalan et al. 6 describe a case of FMD with a superior mesenteric artery aneurysm in a 54-year-old transgender female patient who had undergone gender reassignment surgery and had been prescribed topical estrogen for 10 years. The authors propose that her topical estrogen may have predisposed her to develop FMD. At this time, the exact pathogenesis of FMD remains unclear, and the specific role of endogenous and exogenous female hormones is uncertain. 3 However, among other potential pathogenic factors in this patient, such as cigarette smoking, our case suggests that exposure to estrogen in early childhood and adolescence may be sufficient for the development of multivessel, multifocal FMD, as in this transgender male with prior oophorectomy and almost 40-year use of testosterone with no known familial history of vascular disease. In a case–control study, Sang et al. 4 found no significant association of oral contraceptive use and renal FMD. Furthermore, there are no previous case reports of testosterone supplementation and the development of FMD. Further research is thus required to better identify the influence of exogenous sex hormone exposure and the pathogenesis of FMD. This has been identified as an area in need of further research by a group of international experts. 7
This case also demonstrates important considerations in the management of renovascular hypertension presenting with hypertensive urgency in a previously asymptomatic patient. Randomized controlled trials of renal revascularization have not been performed in patients with FMD. However, based on a meta-analysis by Trinquart et al., 8 complete resolution of hypertension following angioplasty for FMD is relatively low (36%), with better outcomes in younger patients with a shorter duration of hypertension diagnosis. Percutaneous angioplasty is the preferred method of revascularization, with stenting reserved for lesions that fail balloon angioplasty or for bail out in the setting of dissection or aneurysm. 3 Utilization of both IVUS and OCT during angioplasty may be helpful in both the visualization of vascular stenoses and diagnosis of FMD and in guiding angioplasty intervention. 3 In addition, a consensus-based protocol for hemodynamic assessment of the renal artery with measurement of translesional pressure gradients prior to and after intervention has been proposed. 3
Among patients presenting with hypertensive urgency, including transgender patients, renovascular hypertension due to FMD should be included in the differential diagnosis. While outpatient blood pressure readings for the patient presented here were within normal limits, his electrocardiogram (left ventricular hypertrophy) and echocardiogram (left ventricle concentric remodeling) findings do suggest effects of long-standing hypertension. Similarly, following angiographic intervention of his renal FMD, he required ongoing pharmacologic therapy for his hypertension. Patients with FMD thus require ongoing monitoring and management of potential concomitant primary hypertension following intervention for renovascular hypertension.
Conclusion
Thorough investigation of patients presenting with hypertensive emergency is needed. FMD and renal artery stenosis should be considered in the differential diagnosis of all patients, including transgender individuals. Further research on the influence of hormonal factors in the development of FMD is warranted.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from the Institutional Review Board at Case Western Reserve University Hospitals Cleveland Medical Center (Study Number 20191551).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.