
Abstract

What is thrombophilia?
Thrombophilia is an inherited (genetic) or acquired tendency to form blood clots, commonly in the veins, and, in some cases, in the arteries. Blood clots in veins usually occur in the legs (a condition referred to as deep vein thrombosis or DVT) or the lungs (pulmonary embolism or PE). Blood clots in arteries can cause heart attacks, strokes, or blocked blood flow to an arm or leg. A variety of thrombophilias, also referred to as clotting disorders or hypercoagulable states, exist.
The two most common inherited thrombophilias are the factor V Leiden mutation, occurring in 5% of people of European descent, and the prothrombin G20210A gene mutation (also referred to as factor II mutation), present in 2% of the population. People can have one abnormal gene (referred to as heterozygous state or carrier state) or two abnormal genes (referred to as homozygous state). Less common inherited thrombophilias include deficiencies of the blood clotting proteins called protein C, protein S and anti-thrombin. The most common acquired thrombophilia is antiphospholipid antibody syndrome (APS). Other clotting disorders exist, and this is an active area of research.
Most people who have one of these thrombophilias never develop a blood clot. Blood clots are often due to a combination of risk factors, such as surgery, hospitalization and extensive immobility, estrogen therapy (such as birth control or hormone replacement after menopause), pregnancy, obesity, smoking, a family history of blood clots, and advanced age. Thrombophilias can contribute to blood clot formation, but they are typically not the only reason for the clot. For an individual patient who has had a blood clot, all contributing factors must be considered. The decision about how long to treat with a blood thinner (anticoagulant) depends on the combination of risk factors, not just the thrombophilia itself. When a clot occurs without an external triggering factor, it is referred to as unprovoked or idiopathic.
Thrombophilias can roughly be grouped into mild and strong ones (Table 1). It is important to realize that limited scientific data exist on some of these strong thrombophilias because they are rare and have not been extensively studied.
Risk of first and recurrent blood clots associated with different thrombophilias.
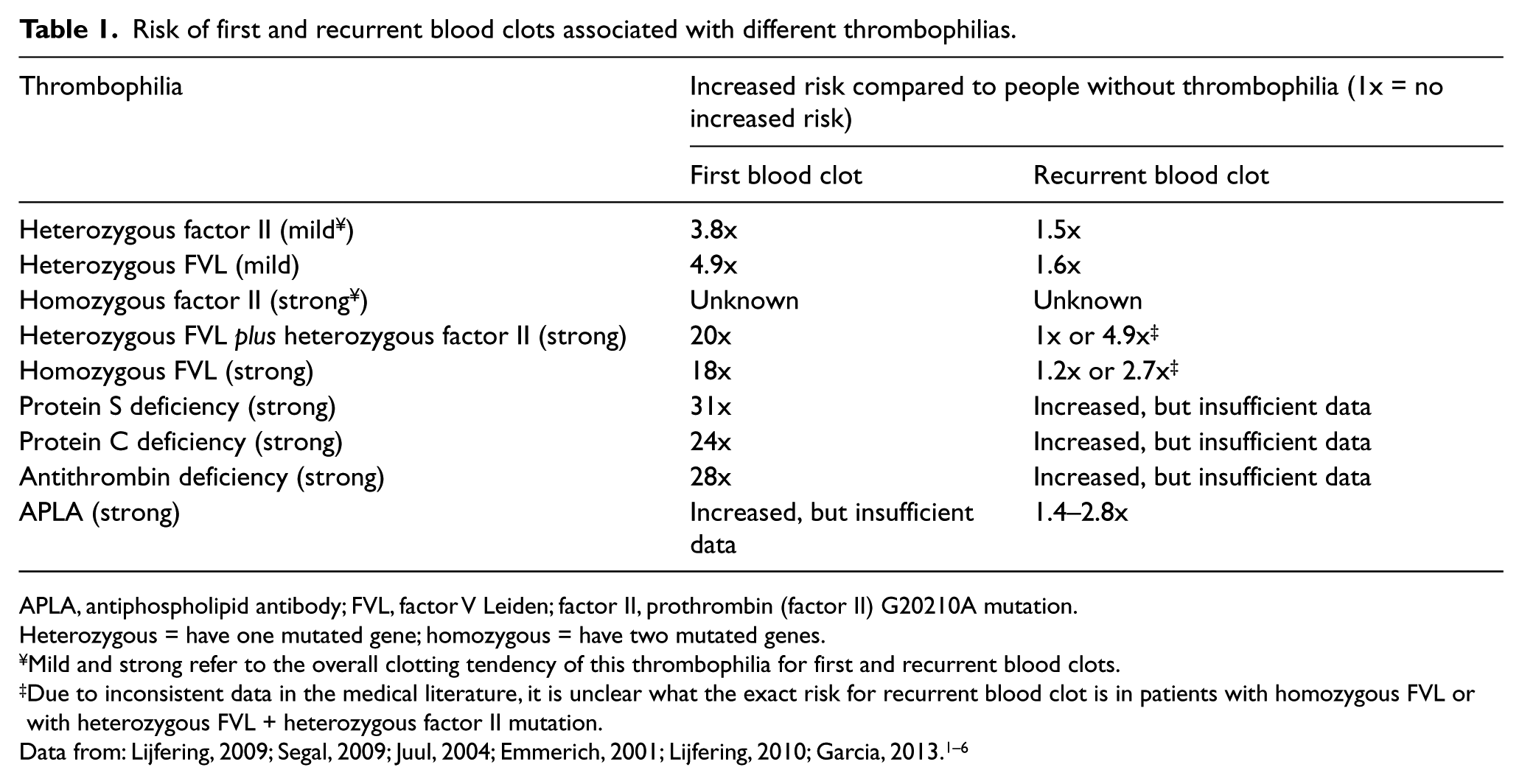
APLA, antiphospholipid antibody; FVL, factor V Leiden; factor II, prothrombin (factor II) G20210A mutation.
Heterozygous = have one mutated gene; homozygous = have two mutated genes.
Mild and strong refer to the overall clotting tendency of this thrombophilia for first and recurrent blood clots.
Due to inconsistent data in the medical literature, it is unclear what the exact risk for recurrent blood clot is in patients with homozygous FVL or with heterozygous FVL + heterozygous factor II mutation.
Thrombophilias increase the risk of developing a first blood clot (Table 1). Everybody who has had a blood clot is at somewhat increased risk for a second (recurrent) one. The presence of a mild thrombophilia does not increase that risk much further. Therefore, decisions about how long to treat a patient who has had a blood clot with anticoagulants, or blood thinners, are typically not influenced by the finding of a mild thrombophilia. However, people with a strong thrombophilia are at significantly higher risk for having a second blood clot (Table 1). Finding such a thrombophilia can be one of the reasons to consider long-term blood thinner therapy.
How is thrombophilia diagnosed?
Thrombophilia is diagnosed via blood tests. These tests can identify gene mutations, the level of clotting proteins, and the presence of antiphospholipid antibodies. Ideally, these thrombophilia blood tests should be ordered by health care providers who are experts in caring for patients with blood clots, to ensure that only appropriate patients get tested, the correct tests are ordered, counseling and education are provided before and after the tests, the lab tests are properly interpreted, and correct treatment advice is given. The results of these blood tests can take a week or two to come back.
The timing of testing is important because some of these tests can be temporarily or falsely abnormal if the patient has had a recent blood clot or is on a blood thinner. Thus, these tests may need to be repeated at a later time to confirm the thrombophilia diagnosis. It is important to note that the patient may still have an inherited or acquired tendency to form blood clots, even if the results from all the currently available thrombophilia blood tests are normal.
Who should be tested for thrombophilia?
There is no general consensus on which patients with blood clots and which family members should be tested for thrombophilia. Multiple guidelines have been published by professional medical societies about testing for thrombophilia, but recommendations vary widely.
Reasons to consider thrombophilia testing include: (1) if the test result will influence how long a patient who has had a blood clot will need blood thinners, (2) if the test will help explain why the clot happened, and (3) if the thrombophilia test result has consequences for other family members who have never had a blood clot.
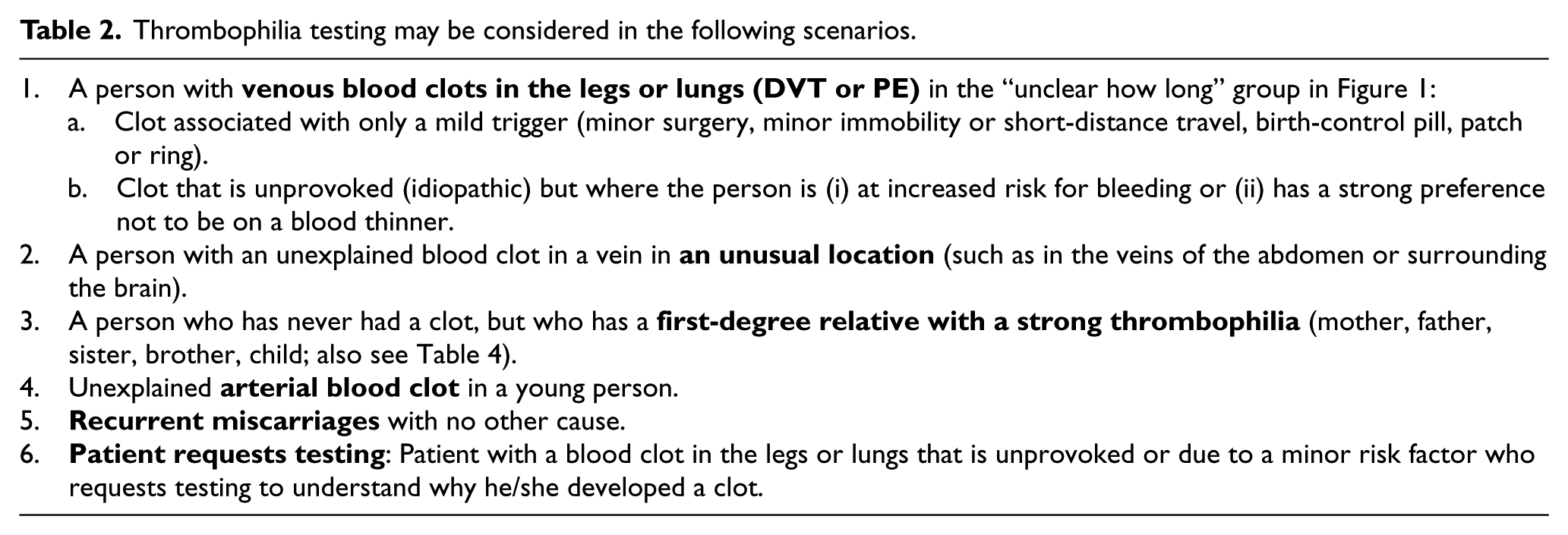
Table 2 lists patients in whom testing could be considered to look for a strong thrombophilia. However, individual decisions need to be made regarding whom to test, what to test, and what consequences the results may have. Table 3 lists the common tests we obtain (and do not obtain) when we decide to test a patient for thrombophilia. Table 4 shows which family members may be considered for testing if a patient has been found to have a thrombophilia.
Thrombophilia testing may be considered in the following scenarios.
Common thrombophilia tests.
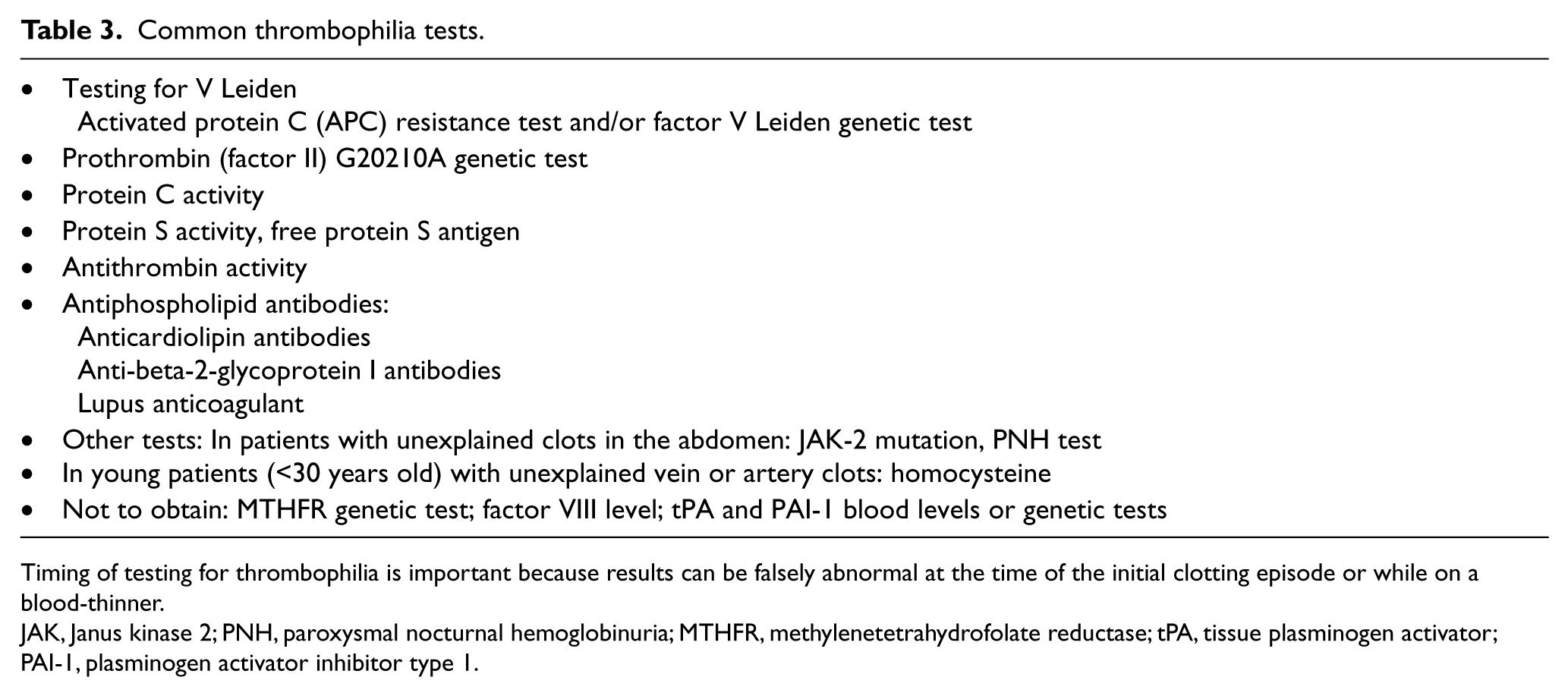
Timing of testing for thrombophilia is important because results can be falsely abnormal at the time of the initial clotting episode or while on a blood-thinner.
JAK, Janus kinase 2; PNH, paroxysmal nocturnal hemoglobinuria; MTHFR, methylenetetrahydrofolate reductase; tPA, tissue plasminogen activator; PAI-1, plasminogen activator inhibitor type 1.
Which family members may consider thrombophilia testing?
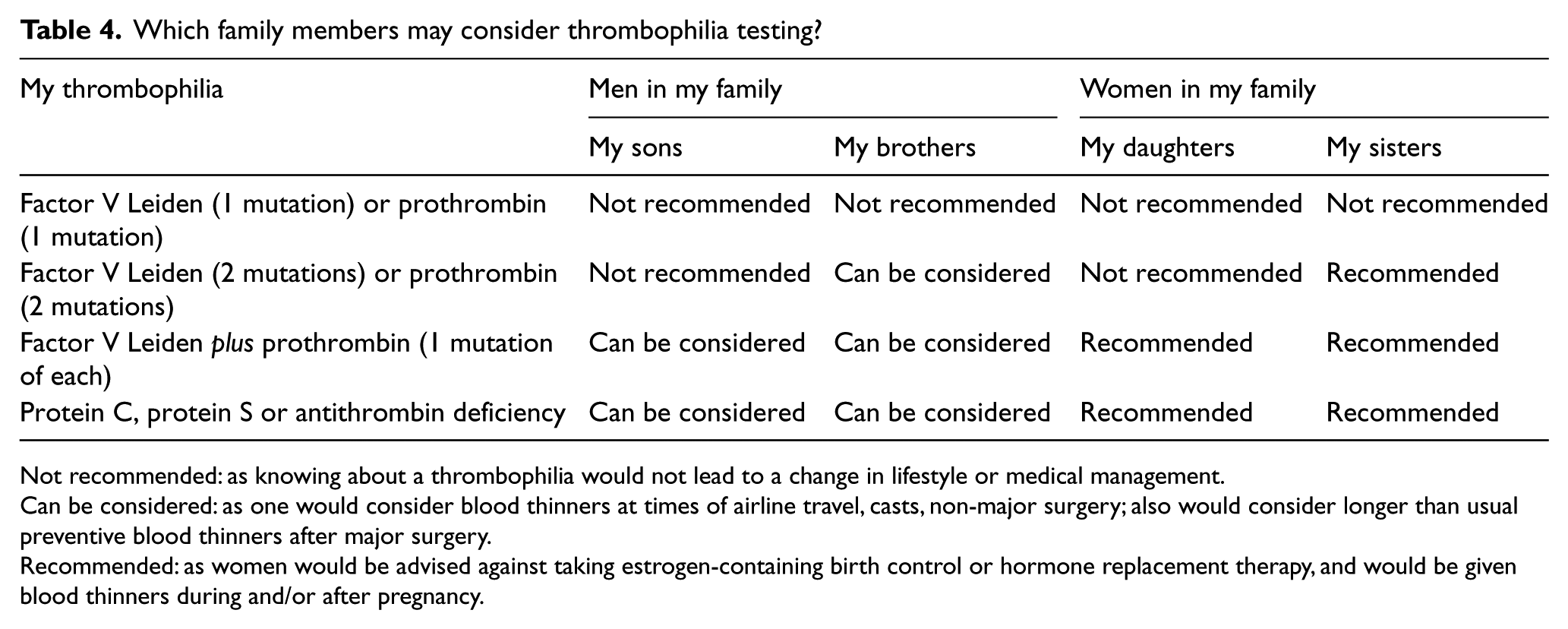
Not recommended: as knowing about a thrombophilia would not lead to a change in lifestyle or medical management.
Can be considered: as one would consider blood thinners at times of airline travel, casts, non-major surgery; also would consider longer than usual preventive blood thinners after major surgery.
Recommended: as women would be advised against taking estrogen-containing birth control or hormone replacement therapy, and would be given blood thinners during and/or after pregnancy.
How does thrombophilia affect me?
If you had a blood clot in a vein (such as a DVT or PE) and were diagnosed with thrombophilia, the physician may change the length of treatment with blood thinners after assessing the risk factors associated with your blood clot. These risk factors strongly predict your risk of developing more blood clots in the future (recurrence). The risk of recurrence triangle shown in Figure 1 helps to illustrate this concept.
If your blood clot developed after a major surgical procedure, you have a low risk of recurrence (top of the triangle). The finding of thrombophilia would not change the duration of treatment with blood thinners (3 months), and you should generally not be tested in the first place.
If no risk factors were identified that led to your blood clot (i.e. you had an idiopathic/unprovoked clot), then you have a higher risk of recurrence (base of the triangle). Men with an idiopathic blood clot have the highest risk of recurrence (bottom of the triangle); women with an idiopathic blood clot are also in the lower part of the triangle, but are at lower risk than men with an idiopathic blood clot. Given the high risk of recurrence for patients with idiopathic blood clots, long-term blood thinners are usually recommended, regardless of the presence or absence of thrombophilia. The finding of a strong thrombophilia would merely help to support this decision.
If your blood clot was associated with minor risk factor(s), such as estrogen-containing birth control pill, patch or ring, hormone replacement therapy, pregnancy, minor surgery or minor immobility, you have an intermediate risk of blood clot recurrence (middle area of the triangle). The finding of a strong thrombophilia moves your position in the triangle downwards (towards the broad base of the triangle), indicating a higher risk of recurrence. Long-term blood thinners may be recommended. On the other hand, the presence of a mild thrombophilia does not change or only slightly changes your position downward in the triangle.
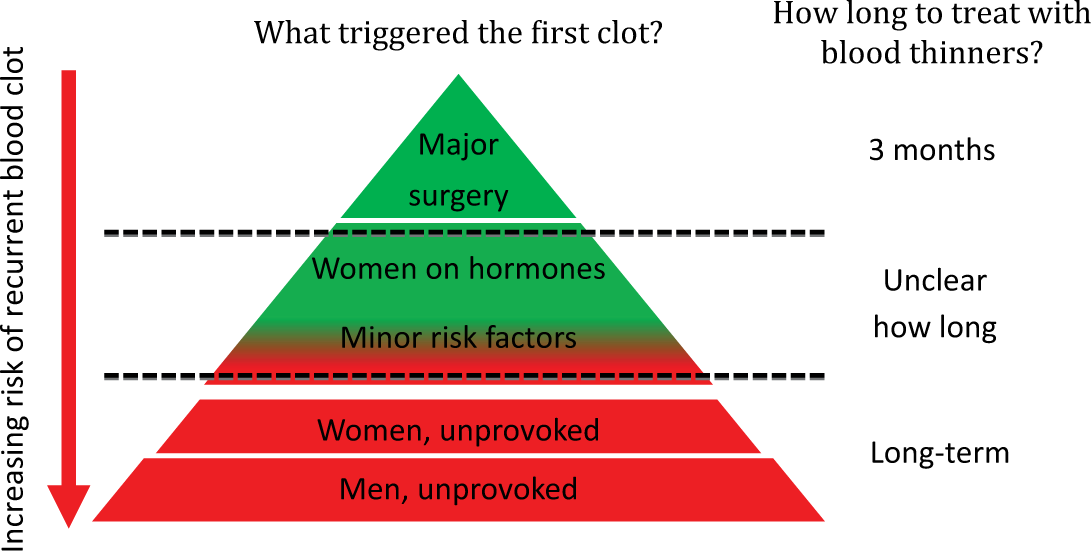
Risk of recurrence triangle.
If you are placed on long-term blood thinners, it is important that you undergo periodic evaluation with your physician to reassess the risks and benefits of being on blood thinners, taking into consideration your risk of bleeding, your treatment preference and lifestyle.
How does thrombophilia affect my family members?
If you are diagnosed with thrombophilia and have had a blood clot, the question arises whether your family members should be tested for the same thrombophilia. This depends on the type of thrombophilia that you have (see Table 4). If you have a mild inherited thrombophilia, testing of family members is not recommended because the results will have no impact on the treatment of family members.
The finding of a strong thrombophilia in a family member who has never had a blood clot does not usually lead to the recommendation for that family member to start long-term blood thinners for prevention of blood clots. However, finding a strong thrombophilia may lead to different treatment recommendations in certain situations:
Giving blood thinners temporarily to prevent clots in high-risk situations: before long-distance travel (>8 hours); at times of certain surgeries, such as arthroscopic knee surgery, or leg injury requiring an immobilizer or cast; during pregnancy and/or for six weeks after delivery.
Longer duration of treatment with preventive doses of blood thinners after surgical procedures or hospital admissions.
Advice to avoid estrogen-containing birth control methods or hormone replacement therapy.
Abbreviations
APLA = antiphospholipid antibodies
APS = antiphospholipid antibody syndrome
DVT = deep vein thrombosis
FVL = factor V Leiden
PE = pulmonary embolism
VTE = venous thromboembolism (a general term for DVT and PE)
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Further non-profit resources for patients
www.clotconnect.org. Clot Connect is a comprehensive web-based educational resource for patients with information on DVT, PE, thrombophilia and anticoagulation.
stoptheclot.org
. The National Blood Clot Alliance (NBCA) is a patient-led advocacy organization for patients with blood clots. www.natfonline.org. The North American Thrombosis Forum is a health organization which is helpful in creating patient support groups.