
Abstract
Sedentary behavior is an adverse health risk factor that is independent of physical activity. The relationship between sedentary behavior, exercise activity and the ankle-brachial index (ABI) is not well understood. We analyzed data from the National Health and Nutrition Examination Survey (NHANES) 2003–2004. Accelerometer data were used to quantify exercise and sedentary time for each participant. A low ABI was defined as a value <1.0 (including borderline values). Multi-variable adjusted logistic regression analyses were performed with sedentary and exercise times as independent variables, adjusting for important confounders. There were 1443 asymptomatic participants (mean age 61 years, 49% female, 55% current/prior smokers) with mean daily sedentary and exercise times of 454±144 and 18±20 minutes, respectively. Of the participants, 23% had an ABI <1.0 (8.7% with ABI <0.9). Sedentary time was positively associated with a low ABI (odds ratio [OR] 1.22 per 1 standard deviation [SD], [95% confidence interval (CI), 1.03–1.43]; p=0.02) while exercise time was inversely associated with a low ABI (OR 0.71 per 1 SD, [95% CI, 0.57–0.89]; p=0.003). Sedentary time is associated with low ABI values in the asymptomatic population. This association appears to be independent of exercise time and warrants further investigation.
Keywords
Introduction
Lower extremity peripheral arterial disease (PAD) affects nearly a fifth of all adults older than 55 years, with increased prevalence in high-risk subgroups such as those with diabetes and smokers.1,2 PAD is associated with higher cardiovascular morbidity and mortality and is currently regarded as a coronary heart disease risk equivalent, 3 regardless of symptoms.4,5
The beneficial effects of physical activity and cardiorespiratory fitness on incident cardiovascular events in unselected populations are well established.6,7 Moreover, there is increasing evidence that the long-term health consequences related to habitual sedentary behavior (sitting too much) are distinct from the effects of a lack of moderate-to-vigorous physical activity (too little exercise).6,8–12 The burden of sedentary behavior appears to be associated with both cardiovascular 13 and all-cause mortality,11,14–16 cardiovascular disease (CVD) events 9 and heart failure. 17
An inverse association between higher levels of physical activity and intentional exercise with PAD has been demonstrated. 18 However, less is known about the role of sedentary behavior, independent of exercise, in this context. Therefore, we sought to characterize the associations of objective measures of physical activity and sedentary behavior with a low ankle-brachial index (ABI) in asymptomatic individuals from the population using data from the National Health and Nutrition Examination Survey (NHANES) 2003–2004.
Methods
Cohort description
NHANES is an ongoing series of surveys that have been conducted by the National Center for Health Statistics since the early 1960s to assess the health and nutritional status of the US civilian, non-institutionalized population. Fifteen geographic locations are selected annually and sampled to represent the general population with a complex, multi-stage probability design. To produce reliable statistics, NHANES over-samples persons aged 60 years and older, African Americans, and Hispanics. The three main components of the study include an interview in the participants’ homes, a medical exam completed at a mobile examination center, and several medical and laboratory tests. The interview includes demographic, socioeconomic, dietary, and health-related questions. Co-morbidities are assessed by self-report. NHANES 2003–2004 included ABI testing for participants aged 40 years and older. All participants were eligible for physical activity monitoring using an accelerometer device. The National Center for Health Statistics Ethics Review Board approved the protocols, and informed consent was obtained from all subjects.
Accelerometer measurements
Participants were asked to wear a single axis ActiGraph model 7164 accelerometer (ActiGraph, LLC, Pensacola, FL) on their right hip during all waking hours for seven consecutive days (except when exposed to water – bathing, showering, swimming, etc.). Accelerometers describe the intensity, duration, frequency, and patterns of movement of an individual. Details of the accelerometer protocol are available. 19 The data collected by the physical activity monitor reflect the intensity of activity as described as counts during a set period of time (1-minute intervals). Data were analyzed using SAS syntax provided by the National Cancer Institute. 20 Wear time was determined by subtracting non-wear time from 24 hours. Non-wear time was defined by an interval of at least 60 consecutive minutes of zero activity counts, with allowance of up to two minutes of counts between 0 and 100. Intensity-threshold criteria for adults have been previously established: 21 2020 counts for moderate intensity (equivalent to three metabolic equivalents [METs]) and 5999 counts for vigorous intensity (equivalent to 6 METs) activities. Exercise minutes were defined as all minutes above these count thresholds and quantified as the mean minutes of exercise activity per day for each participant. Sedentary behavior is defined as behaviors that involve low levels of energy expenditure (1.0–1.5 METs, including sitting, watching TV, reading, and driving). 12 By accelerometer, sedentary time was defined as <100 counts per minute of wear time in mean minutes per day. 21 Mean count intensity is defined by the raw counts provided by the accelerometer without imposition of any external criteria. It encompasses all activity (sedentary, light, moderate, and vigorous-intensity) into a single variable, with every minute accounted for. Mean count intensity was calculated by dividing the sum of 1-minute count intensities for a valid day by the number of minutes of wear time, averaged across all valid days. Higher mean count intensity indicates a more active profile (but not necessarily more exercise).
Ankle-brachial index
An ABI <0.90 has up to 99% specificity and, at most, 80% sensitivity for angiographically significant PAD. 22 Using an ABI ⩽1.0, the sensitivity increases to as high as 100%. The Parks Mini-Lab IV, Model 3100 (Aloha, OR), a vascular testing device, was used to measure systolic pressures in the extremities (calibration checked daily). The appropriate cuff to be used was determined by the circumference of the participant’s bare upper arm at the midpoint. In the supine position, systolic blood pressure (SBP) was measured in one arm (brachial artery, right arm if accessible) and both ankles (posterior tibial vessels) with an 8.1 MHz Doppler probe. Each pressure was measured twice in subjects aged 40–59 years, while each pressure was measured only once for subjects aged 60 years and older to reduce the time for this testing component in that age group. The ABI was automatically calculated by the computer system for each leg as the ankle pressure divided by the arm pressure. All ABI data were verified by the National Center for Health Statistics before data release. 23 Using an ABI value of ⩽1.0 increases sensitivity for significant PAD to as high as 100%. 22 Therefore, we defined a low ABI as <1.0 in either leg (to include borderline values of 0.91–0.99). Normal ABI was defined as an ABI of 1.0 to 1.4. Participants with an ABI over 1.4 were excluded from this analysis, as these individuals generally have artificially-elevated lower extremity arterial pressures from calcified arterial vessels.
Other measures
Age, sex, race, tobacco use (⩾100 cigarettes in lifetime), history of atherosclerotic cardiovascular disease (CVD), hypertension, hyperlipidemia, and diabetes mellitus were based on participant self-report. Height and weight were obtained by trained health technicians and followed a standard protocol. The physical functioning questionnaire section in NHANES includes questions about limitations caused by any long-term physical, mental or emotional problem or illness. 24 In order to restrict our analysis to asymptomatic persons, participants were eliminated if they answered ‘yes’ to either of the following questions: 1) Are you limited in the kind or amount of work you can do because of a physical, mental or emotional problem? 2) Because of a health problem, do you have difficulty walking without using any special equipment?
Statistical analysis
Baseline characteristics, ABI and accelerometer-derived variables were compared across tertiles of sedentary time using the Jonckheere-Terpstra test for trend. 25 For the primary analysis, multivariable-adjusted logistic regression analyses were performed with abnormal ABI as the dependent (dichotomous) variable. In another multivariable-adjusted linear regression model, ABI was further assessed as a continuous outcome variable. All models were adjusted for age, gender, BMI, race, tobacco use (⩾100 cigarettes in lifetime), diabetes mellitus, hypertension, hyperlipidemia, height, known CVD, and mean accelerometer wear time. Exposure variables included accelerometer-derived sedentary time and combined moderate and vigorous exercise time together in the same model. Because prior studies have shown gender differences in ABI that are reduced by adjusting for height, we also included height as a covariate. 22
Sensitivity analyses were performed with lower thresholds for defining a low ABI: ⩽0.95 and ⩽0.90. An additional analysis was performed after restricting the participant population to those free of CVD. In a final analysis, mean count intensity, a measure of the average accelerometer count intensity per day over the entire length of accelerometer wear time, replaced the exposure variables of sedentary and exercise time. All analyses were performed using SAS version 9.2 (SAS Institute, Inc, Cary, NC).
Results
A total of 2238 NHANES participants underwent ABI testing. Among them, 279 participants did not have at least one valid day of physical activity monitoring (a valid day is defined as ⩾10 hours of accelerometer wear time), 332 were missing important covariates and five more were excluded due to an ABI >1.4. After excluding an additional 179 on the basis of a physical functioning impairment, the final population consisted of 1443 participants with ABI testing and sufficient accelerometer data.
The mean age of the study population was 61 (SD 13) years with 49% female; 12.6% had known CVD. Mean daily exercise time was 18 (SD 20) minutes, while mean daily sedentary time was 454 (SD 144) minutes. Baseline characteristics of all participants, stratified by sedentary time tertiles, are shown in Table 1. Participants with higher sedentary times were more likely to be older, male, and to have a higher prevalence of co-morbidities such as diabetes, hypertension, and known CVD. No difference was observed in BMI across sedentary time tertiles. Exercise time was inversely associated with sedentary time (r=−0.334, p=<0.0001).
Baseline characteristics of participants stratified by sedentary time tertile.
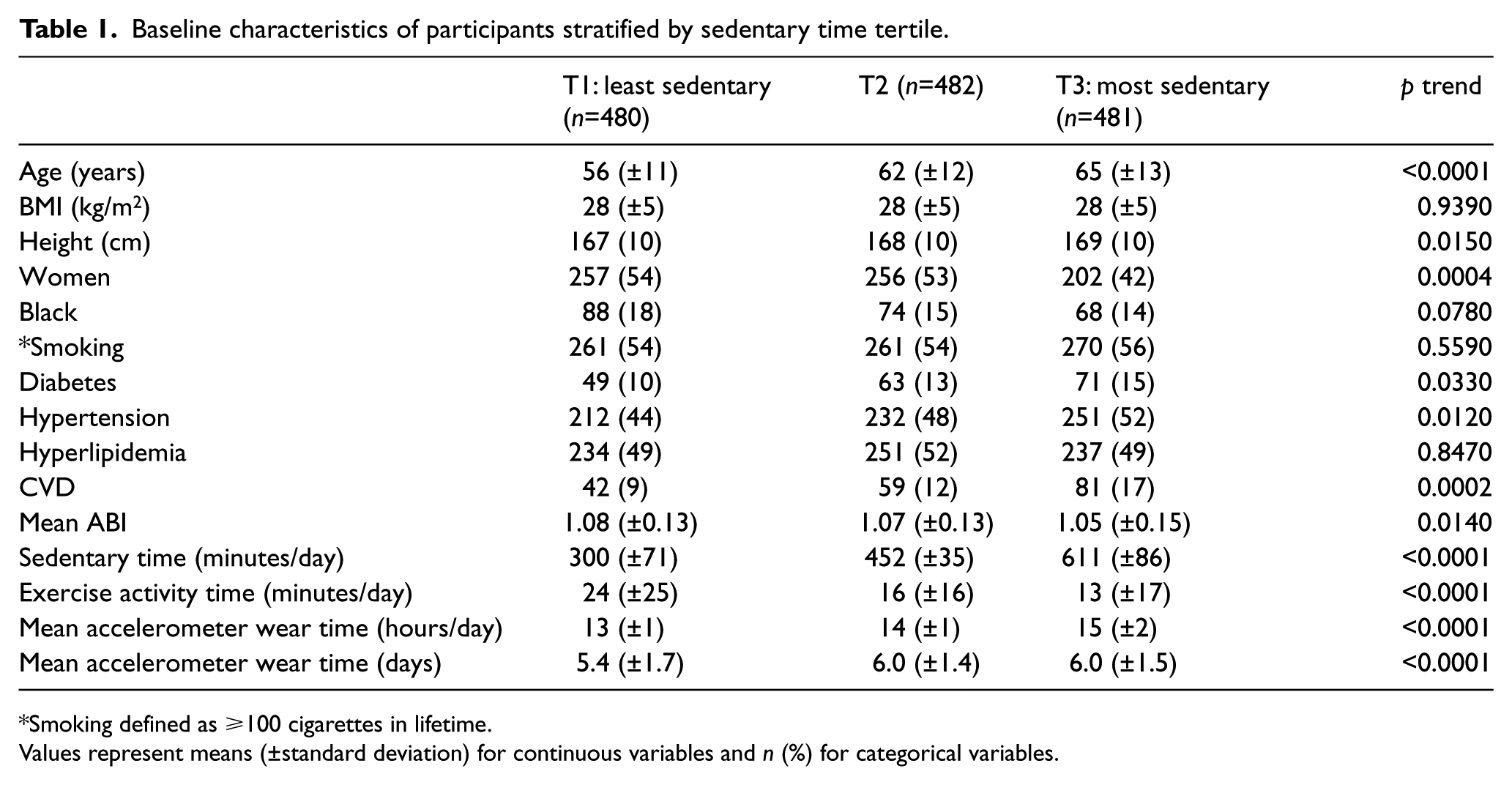
Smoking defined as ⩾100 cigarettes in lifetime.
Values represent means (±standard deviation) for continuous variables and n (%) for categorical variables.
ABI decreased across sedentary time tertiles (mean±SD: 1.08±0.13, 1.07±0.13, 1.05±0.15, p trend <0.0001). The proportion of individuals with a low ABI was 23% in the overall cohort and increased in a stepwise fashion across sedentary time tertiles (19.6%, 21.6%, 27.9%; p trend=0.002). In multivariable logistic regression analyses, higher daily sedentary time was associated with a 22% higher odds of having a low ABI (odds ratio [OR]=1.22 per 1 standard deviation [SD] [144 minutes] change; [95% confidence interval (CI), 1.03–1.43], p=0.018) (Figure 1). Exercise time was independently associated with a 29% lower odds of having a low ABI (OR=0.71 per 1 SD [13 minutes] change; [95% CI, 0.57–0.89], p=0.003) (Figure 1). Other variables independently associated with a low ABI were age, black race, short height, tobacco use, diabetes mellitus, and known CVD (Figure 1). In a multivariable linear regression model with ABI as a continuous outcome variable, sedentary time was inversely associated with ABI (β=−0.012 per SD, p=0.003) while exercise time was positively associated with ABI (β=0.008 per SD, p=0.019).
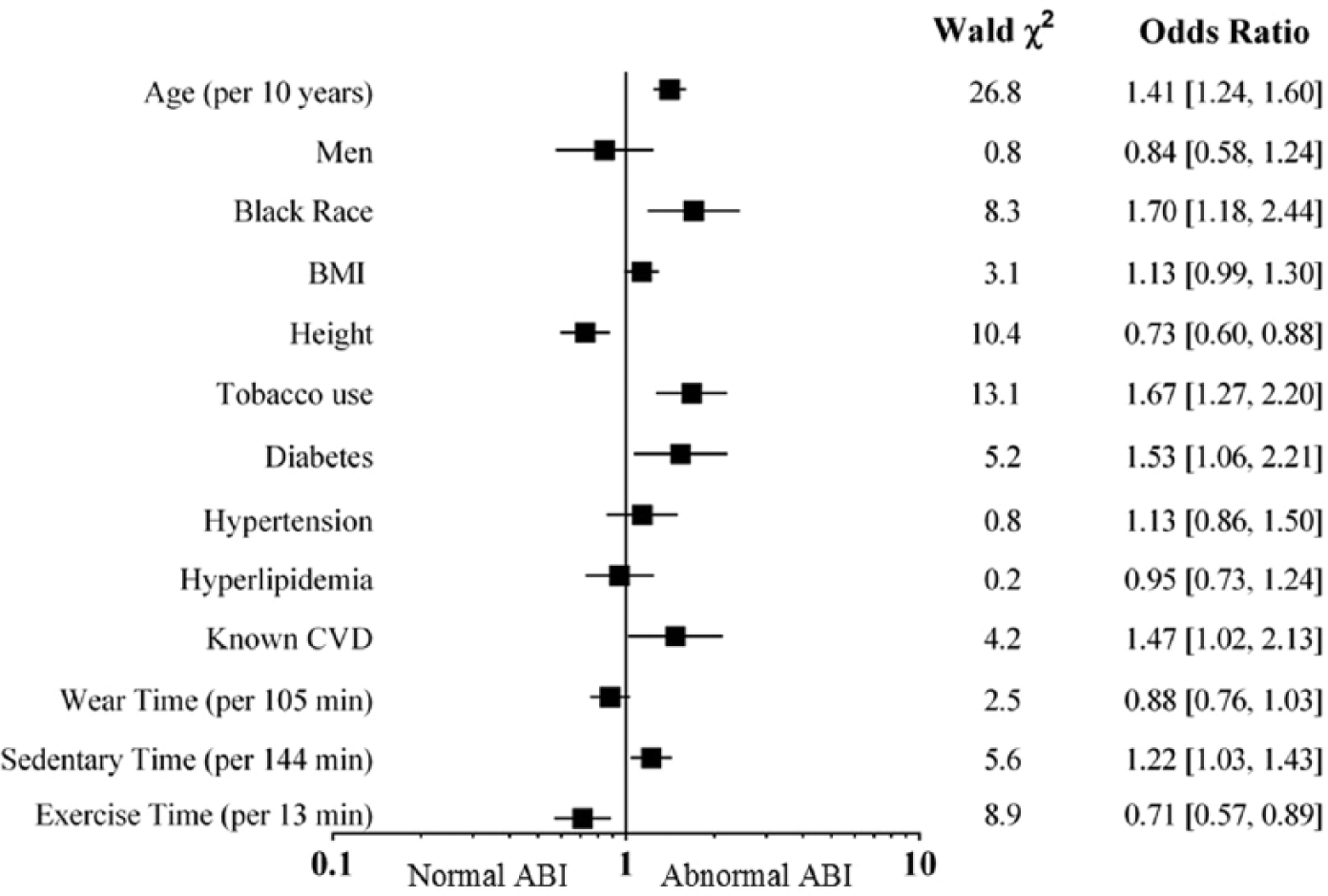
Odds ratios for abnormal ABI (with 95% confidence intervals) are displayed for all covariates including exposure variables of sedentary time and exercise time. Wald chi-square values are also shown. With the exception of age, continuous variables (BMI, height, sedentary time, and exercise time) are per one standard deviation.
Sensitivity analyses
ABI values ⩽0.95 and ⩽0.90 were observed in 13.6% (n=196) and 8.7% (n=125) of all participants, respectively. In sensitivity analyses restricting the definition of abnormal ABI to ⩽0.95, sedentary and exercise times remained independently associated with abnormal ABI (OR=1.30 [95% CI, 1.06–1.59]; p=0.01 and OR=0.71 [95% CI, 0.52–0.95]; p=0.02, respectively). After further restricting the definition of abnormal ABI to ⩽0.90, sedentary time was of borderline significance (OR=1.26 [95% CI, 0.98–1.62]; p=0.06); exercise time was no longer statistically significant (OR=0.81 [95% CI, 0.58–1.14]; p=0.23). Of note, diabetes mellitus also lost statistical significance (p=0.17) in this analysis, suggesting that this may be due to low statistical power (Table 2).
Primary and sensitivity analyses for an abnormal ABI result with activity exposure variables (n=1443).
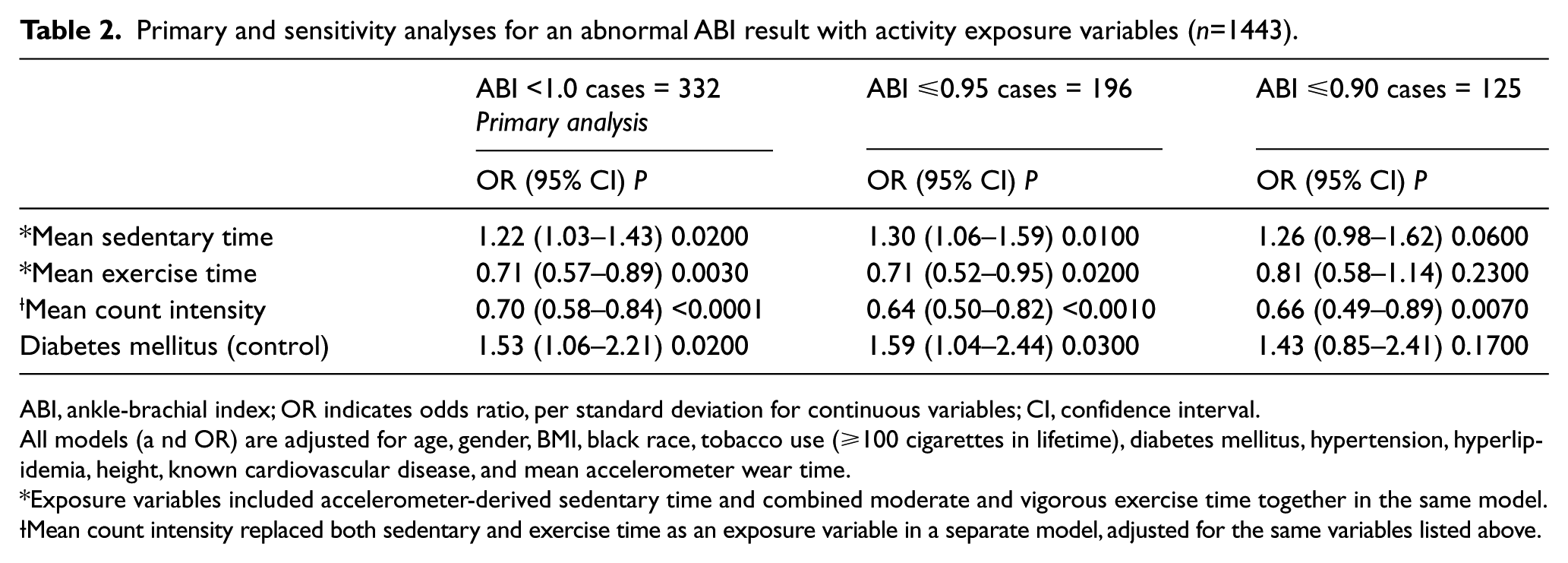
ABI, ankle-brachial index; OR indicates odds ratio, per standard deviation for continuous variables; CI, confidence interval.
All models (a nd OR) are adjusted for age, gender, BMI, black race, tobacco use (⩾100 cigarettes in lifetime), diabetes mellitus, hypertension, hyperlipidemia, height, known cardiovascular disease, and mean accelerometer wear time.
Exposure variables included accelerometer-derived sedentary time and combined moderate and vigorous exercise time together in the same model.
Mean count intensity replaced both sedentary and exercise time as an exposure variable in a separate model, adjusted for the same variables listed above.
When mean count intensity was substituted as the exposure variable for both the sedentary and exercise time exposure variables in the fully adjusted model, we observed an inverse association between mean count intensity and abnormal ABI (OR=0.70 [95% CI, 0.58–0.84]; p<0.0001). This association was insensitive to the definition for abnormal ABI (Table 2). In a second series of sensitivity analyses, 183 participants with known CVD were excluded. Results of the multivariable logistic regression analyses were similar to those in the overall study population (Table 3).
Multivariable logistic regression analyses after excluding participants with known cardiovascular disease (n=1260).
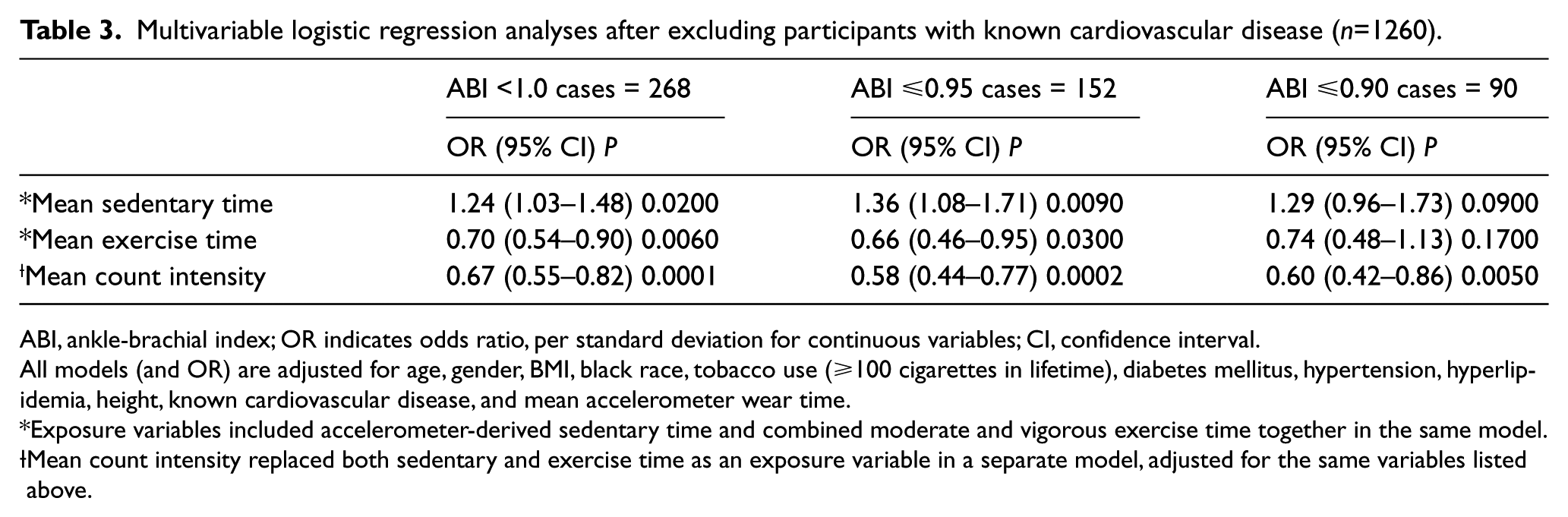
ABI, ankle-brachial index; OR indicates odds ratio, per standard deviation for continuous variables; CI, confidence interval.
All models (and OR) are adjusted for age, gender, BMI, black race, tobacco use (⩾100 cigarettes in lifetime), diabetes mellitus, hypertension, hyperlipidemia, height, known cardiovascular disease, and mean accelerometer wear time.
Exposure variables included accelerometer-derived sedentary time and combined moderate and vigorous exercise time together in the same model.
Mean count intensity replaced both sedentary and exercise time as an exposure variable in a separate model, adjusted for the same variables listed above.
Discussion
In this analysis of 1443 asymptomatic participants from the general population, higher sedentary time is directly associated with a low ABI, independent of the inverse association of exercise time with a low ABI. These associations are independent of traditional PAD risk factors, including age, smoking, diabetes mellitus, and known CVD. This study is one of the largest to evaluate the association between objectively-measured exercise time and a low ABI, and, to our knowledge, one of the first to demonstrate a positive association between sedentary time and a low ABI, independent of physical activity.
The relationship between exercise activity and PAD has been examined in a few studies. In an analysis of consecutive patients referred to two hospitals for coronary angiography, Wilson and colleagues reported that self-reported low lifetime recreational activity was associated with having a low ABI. 26 Sedentary behavior was not included. Similarly, an analysis from the Multi-Ethnic Study of Atherosclerosis (MESA) cohort noted that self-reported intentional exercise was protective against incident PAD. 18 McDermott and colleagues have reported that asymptomatic PAD is associated with lower accelerometer-measured physical activity and impaired lower extremity function, including slower walking velocity and a shorter distance walked in 6 minutes. While they did use accelerometers to measure physical activity, they did not specifically quantify exercise and sedentary time.27,28 Overall, there are scant data on the relationship between sedentary and exercise activity and a low ABI. Our study illustrates the unique relationship between sedentary time and a low ABI, independent of exercise activity time. Furthermore, the significance of the mean count intensity variable, encompassing all daily activity and sedentary time, emphasizes the value of routine, non-exercise (light-intensity) activities and staying active throughout the day. Because ABIs up to and including 1.10 (many of which will be asymptomatic) are associated with elevated cardiovascular risk and mortality, 22 expanding knowledge of potentially modifiable risk factors (such as activity patterns) may lead to early intervention and prevention of the disabling consequences of PAD.
A major strength of our study is the use of objective measures to define sedentary and exercise times. This has been a major limitation of prior studies, which have predominantly relied on questionnaire data to assess physical activity and/or sedentary time. For example, the MESA activity questionnaire quantifies sedentary time as the sum of reading and watching television. 18 Another study’s questionnaire intentionally discounted all sedentary time that was part of one’s occupation. 17 Time spent sitting while driving, riding in a bus or even while eating, all contribute to daily sedentary time. Given the increase in urbanization, technology advancement, and fewer manual labor jobs, occupational sedentary time is undoubtedly important as well. Our study is also novel in that it highlights the association of both components of physical inactivity (lack of exercise and sedentary lifestyle) with a low ABI.
Accelerometers allow for more robust assessments of activity behaviors than self-report and can more accurately measure the full range of activity, from sedentary behavior to vigorous intensity exercise. Incorporating accelerometers into population-based public health research has been instrumental in advancing the field of sedentary physiology 29 and has contributed to our understanding that the physiological effects of sedentary behavior are distinct from low physical activity. Studies indicate that the detrimental effects of sedentary behavior may be related to adverse metabolic changes including a reduction in muscle lipoprotein lipase activity and increased fasting insulin levels for which the magnitude of the deleterious effects of sedentary behavior far exceed that of the beneficial effects of exercise.8,30 Sedentary behavior also appears to negatively impact endothelial function, resulting in microvascular dysfunction and a reduction in endothelium-dependent vasodilation in healthy volunteers subjected to as little as 3 hours of sitting.29,31–33 These deleterious changes were prevented by aerobic and resistance exercise, suggesting a common mechanism linking vascular health to both sedentary and exercise activity.29,31
Our study has several limitations. The most substantial limitation, since this is a cross-sectional study, is the likelihood that a low ABI promotes more sedentary behaviors due to claudication symptoms or that people may unknowingly limit their activity to avoid leg symptoms and become asymptomatic (i.e. reverse causation). 28 We attempted to minimize this by excluding subjects with self-reported limitations in physical activity. Moreover, we also excluded participants with known CVD, and observed similar results. The questions used to exclude these participants were what was captured in NHANES, but may not identify those who have truly asymptomatic PAD.27,34,35 Earlier studies from NHANES have, however, demonstrated a correlation between physical disability (used in this study as an exclusion for possible ‘symptomatic’ PAD) and the presence of PAD. 36 We were underpowered to consider only ABIs ⩽0.90 as abnormal. Although an ABI cut-off point of 0.90 is used to diagnose PAD, the ABI Collaboration has concluded that both cardiovascular events and mortality increase as the ABI decreases below a threshold of 1.10, regardless of symptoms. 37 Therefore, we included borderline ABI values of 0.91–0.99 in our abnormal ABI cases for this analysis. Finally, a uniaxial accelerometer was used in this study. Although triaxial accelerometers were designed to capture more information from different types of activities (as they incorporate acceleration from three orthogonal directions), population studies have concluded that these two types of accelerometers do not differ in their measurement of physical activity in population studies, and that either could be used. 38
In conclusion, our study is the first to document independent relationships between sedentary times and a low ABI. This association appears to be independent of exercise time. Because of the expanding epidemiology evidence of the adverse health risks associated with increased sitting time, independent of the lack of exercise, understanding this gap in the scientific literature could have important implications for public health physical activity guidelines.
Footnotes
Declaration of conflicting interest
Dr Kumbhani has received honoraria from the American College of Cardiology. Dr De Lemos has received honoraria from Astra Zeneca, consulting income from Janssen Pharmaceuticals, and serves on a Data Safety Monitoring Board for Novo Nordisk. Dr Berry is a member of the Speaker’s Bureau for Merck & Co. Dr Banerjee has received consultant honoraria from Medtronic, research grants from Boston Scientific and Gilead, and has intellectual property/ownership in Mdcare Global and Hygeia Tel.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Abbreviations
NHANES = National Health and Nutrition Examination Survey
ABI = ankle-brachial index
PAD = peripheral arterial disease
CVD = cardiovascular disease
BMI = body mass index