
Abstract
We conducted a randomized, double-blind trial of losartan (100 mg QD) versus atenolol (50 mg QD) for 6 months in adults with Marfan syndrome. Carotid-femoral pulse wave velocity (PWV), central augmentation index (AIx), aortic diameter and left ventricular (LV) function were assessed with arterial tonometry and echocardiography. Thirty-four subjects (18 female; median age 35 years, IQR 27, 45) were randomized. Central systolic and diastolic blood pressure decreased comparably with atenolol and losartan (p = 0.64 and 0.31, respectively); heart rate decreased with atenolol (p = 0.02), but not with losartan. PWV decreased in patients treated with atenolol (–1.15 ± 1.68 m/s; p = 0.01), but not in those treated with losartan (–0.22 ± 0.59 m/s; p = 0.15; between-group difference p = 0.04). In contrast, AIx decreased in the losartan group (–9.6 ± 8.6%; p < 0.001) but not in the atenolol group (0.9 ± 6.2%, p = 0.57; between-group difference p < 0.001). There was no significant change in aortic diameters or LV ejection fraction in either treatment group. In adults with Marfan syndrome, 6 months of treatment with atenolol improves PWV, whereas losartan reduces the AIx. By improving vascular stiffness via distinct mechanisms of action, there is physiologic value to considering the use of both medications in individuals with Marfan syndrome.
Keywords
Introduction
Aortic dissection and aortic rupture are the leading causes of premature death in patients with Marfan syndrome.1,2 In Marfan syndrome, gene mutations lead to deficiency of fibrillin-1, a constituent of the extracellular matrix microfibrils responsible for sequestration of the transforming growth factor beta (TGF-β) complex. This leads to extracellular matrix disruption, allowing TGF-β overexpression, thickening of the aortic media, fragmentation and disarray of elastic fibers, and increased collagen deposition.3,4 These changes impair elastic recoil of the aortic wall, which may manifest as aortic stiffness even in the absence of aortic dilation.5–7 Indeed, aortic stiffness is greater in patients with Marfan syndrome compared with healthy persons.8–12 Abnormal aortic elasticity predicts aortic dilation and aortic dissection in individuals with Marfan syndrome.13,14 Also, the disproportionate vascular load associated with increased aortic stiffness may contribute to left ventricular systolic and diastolic dysfunction, which can occur in adults with Marfan syndrome.15–19
Current treatment for adults with Marfan syndrome centers on β-receptor blockade, which is recommended to decrease the aortic dilation rate and reduce aortic event risk.20–22 The degree of aortic dilation, however, varies in adults with Marfan syndrome and the response to β-receptor blockers in adults with Marfan syndrome is heterogeneous.21,23,24 Angiotensin receptor blockers (ARBs) reverse aortic pathology in fibrillin mutation mouse models of Marfan syndrome. 3 Small clinical studies also suggest that renin-angiotensin system inhibitors favorably affect aortic structure and function, notably decreasing aortic stiffness and reducing the rate of aortic expansion in patients with Marfan syndrome.25–29
We administered losartan and atenolol in a randomized double-blind trial to compare their effects on arterial stiffness and left ventricular function in adults with Marfan syndrome.
Methods
Patient selection
After approval from the Partners Human Research Committee, individuals with Marfan syndrome were screened for eligibility. Eligible participants were over age 18 years, able to consent, and met the 1996 Ghent Criteria for Marfan syndrome. 30 Participants were enrolled between March 2008 and May 2012. Patients with a history of aortic dissection, prior cardiac or aortic surgery, a planned aortic operation in the next 6 months, congestive heart failure, greater than mild aortic or mitral regurgitation by echocardiography, chronic ARB use, a previous adverse reaction to ARB or β-blocker treatment, serum creatinine >2.0 mg/dL, hypertension (>140/90 mm Hg), bronchospastic disease, hyperthyroidism, and pregnancy were excluded.
Research design
This was a randomized, double-blind, parallel design trial of losartan versus atenolol. Computer-generated numbers specified the drug allocation sequence. Patients were evaluated at a screening visit and those who met all inclusion/exclusion criteria were enrolled. Patients taking a β-receptor blocker or angiotensin-converting enzyme (ACE) inhibitor underwent a 2-week washout period before baseline measurements were taken.
The treatment period was 6 months. The hospital research pharmacy randomly assigned participants to losartan 50 mg once daily or atenolol 25 mg once daily in a blinded manner. After a 1-week safety period laboratory evaluation and brachial blood pressure measurements were performed. Blood pressure was assessed using auscultation and sphygmomanometry following standard guidelines. Three measurements were performed at rest and averaged. The medication dose was then titrated to losartan 100 mg once daily and atenolol 50 mg once daily. Medication adherence was recorded and there was 98% compliance. Arterial tonometry and echocardiography were performed at baseline and 6 months after randomization. ClinicalTrials.gov Identifier: NCT00723801.
Arterial stiffness measurements
Aortic stiffness was assessed using applanation tonometry (SphygmoCor®; AtCor Medical, Australia) to measure carotid to femoral artery pulse wave velocity (PWV) by a single operator. With the patient lying supine in a quiet environment, a handheld micromanometer-tipped probe was applied to the skin surface over the carotid and femoral arteries, compressing the vessel wall so that transmural forces within the vessel wall were perpendicular to the arterial surface. The distance from the sternal notch to the sites of carotid and femoral pulse acquisition were measured and inputted into the device to represent the relative distance from the carotid to femoral artery. The calculation of distance divided by time of pulse upstroke relative to the upstroke of the QRS on a three-lead surface electrocardiogram was used by the device to calculate velocity. All recorded measurements met the manufacturer’s quality control standards integrated into the software package. Applanation tonometry was also performed at the radial artery. The central aortic pressure was derived from the radial artery pressure waveform using a previously validated mathematical generalized transfer function and a non-invasively measured brachial blood pressure. The transfer function is based on the relationship between pressure waves at different sites and assumes linearity between the two. This enables determination of the central aortic augmentation index (AIx) (the percentage of pulse pressure attributable to reflected waves). Waveform analysis was conducted using software capable of Fourier analysis of the non-invasive velocity and pressure data.
Evaluation of left ventricular function
Two-dimensional echocardiography was performed using a 3.0 MHz transducer (VIVID 7; General Electric Healthcare, USA). Left ventricular and left atrial dimensions were determined in parasternal long axis views. The left ventricular ejection fraction was calculated using the modified Simpsons calculation in the apical two and four chamber views. Diastolic function was assessed using pulsed-wave Doppler measurement of mitral valve inflow (early and atrial filling velocities and deceleration time of E) and Doppler tissue imaging of the septal and lateral mitral annulus to assess myocardial relaxation velocity. Aortic root measurements were made in the parasternal long-axis view at end-diastole (peak of R wave on electrocardiogram) and at the proximal ascending aorta, 1–2 cm above the supra-aortic ridge. All measurements were made using the leading edge technique. The sonographer and interpreter were blinded to the clinical data and treatment assignment.
Statistical analysis
All analyses were performed on an intention-to-treat basis. The study was powered to detect a mean absolute difference in pulse wave velocity of at least 1 m/s between the two groups with an estimated standard deviation of the difference of 0.5 m/s. Continuous variables are summarized using either the mean and standard deviation or median and interquartile range; comparisons were performed between groups with the unpaired t-test or Wilcoxon rank sum test as appropriate. Categorical variables are summarized as frequency and percent and compared using Fisher’s exact test. Changes in outcome measures pre- to post-treatment were assessed using the paired t-test; comparisons of mean changes between treatment groups were performed using the unpaired t-test. Linear regression analysis was used to evaluate whether differences in outcomes between treatment groups were attenuated after adjustment for gender, age, or differences in blood pressure or heart rate. A p-value <0.05 was considered statistically significant.
Results
Baseline demographics
There were 519 patients screened by medical record review at the Brigham and Women’s Hospital, Massachusetts General Hospital and Children’s Hospital of Boston for eligibility. Of these individuals, 105 were deemed eligible and approached: 41 agreed to enroll and 34 completed the study (Figure 1). The seven patients who did not complete the study included one lost to follow up, three who consented initially and then withdrew consent before randomization, and three who consented but upon detailed screening were found not to meet Ghent criteria for Marfan syndrome. Beta-blockers were withdrawn in nine patients 2 weeks prior to performance of any baseline measurements (five in the atenolol arm and four in the losartan arm). No patients were taking ACE-inhibitors 2 weeks prior to enrollment. Baseline data for the 34 enrolled patients are shown in Table 1. The median age was 35 years (IQR 27, 45). There were 53% females. Of the 34 patients, 17 were randomly assigned to atenolol and 17 were assigned to losartan.
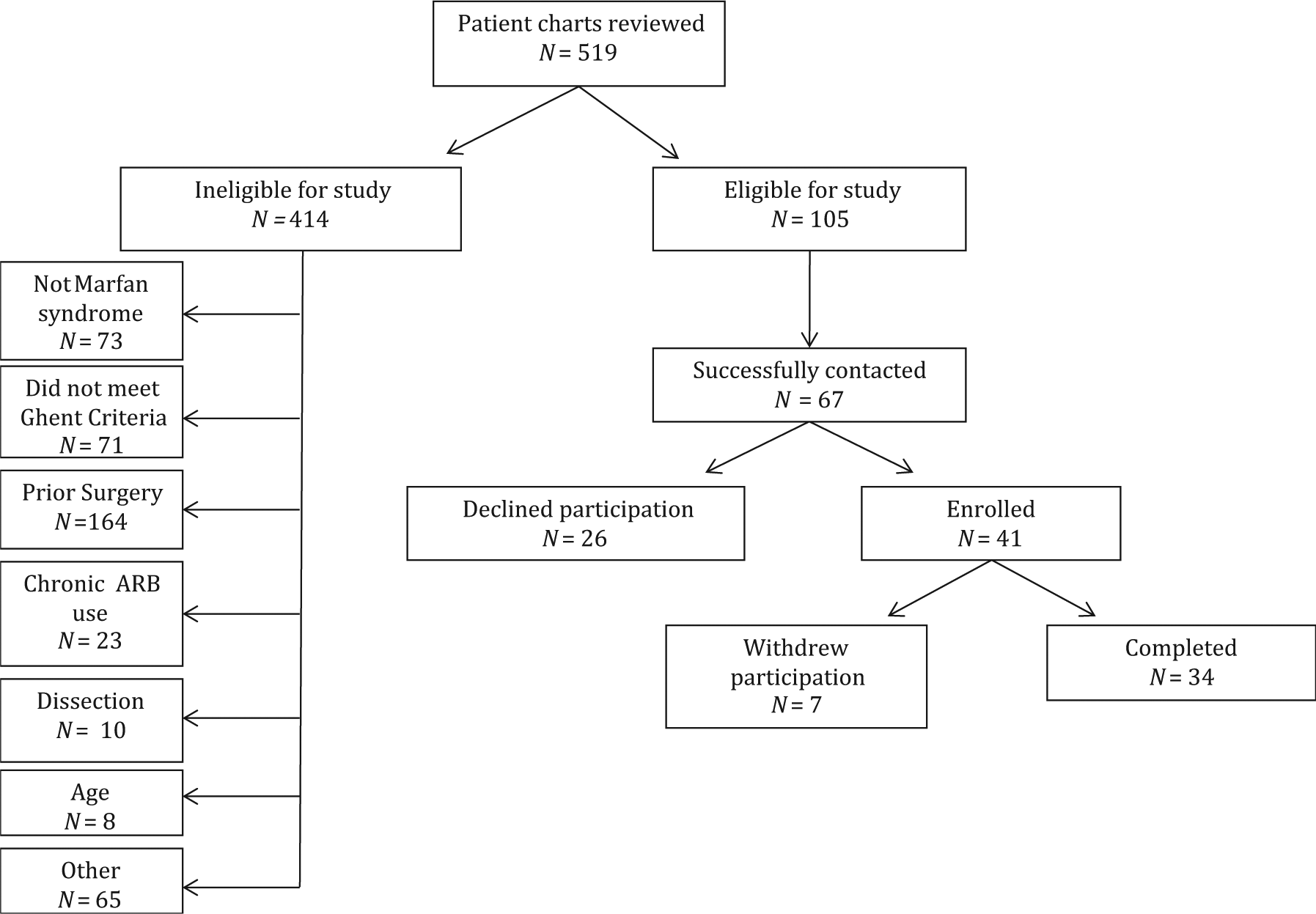
Trial CONSORT diagram. Selection, study enrollment, randomization, and retention of study participants.
Baseline characteristics of participants by treatment group.
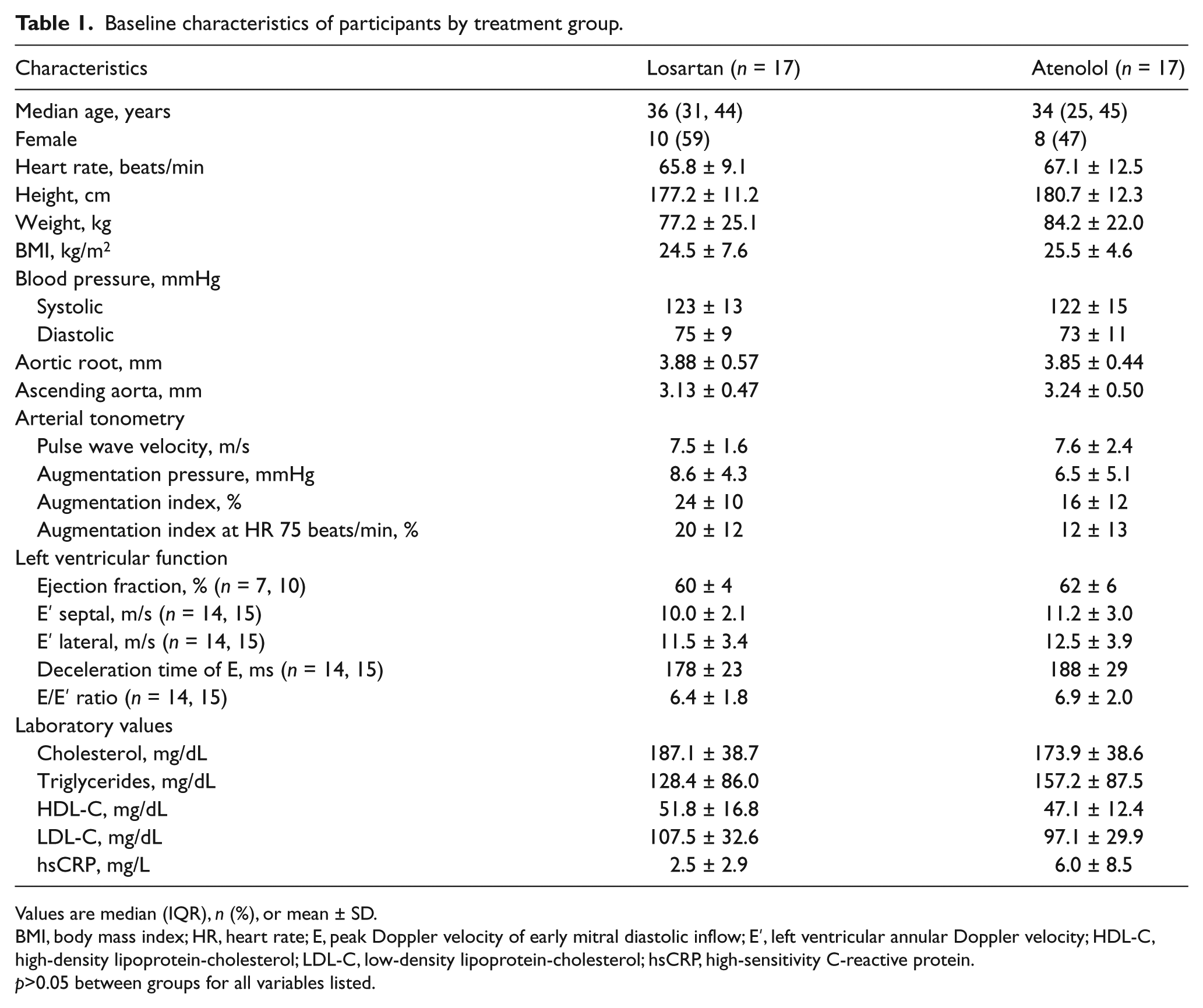
Values are median (IQR), n (%), or mean ± SD.
BMI, body mass index; HR, heart rate; E, peak Doppler velocity of early mitral diastolic inflow; E′, left ventricular annular Doppler velocity; HDL-C, high-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein-cholesterol; hsCRP, high-sensitivity C-reactive protein.
p>0.05 between groups for all variables listed.
The two groups were similar with respect to all pretreatment variables (Table 1), including age, gender, heart rate, blood pressure, laboratory values, PWV, AIx, non-invasive measures of cardiac systolic and diastolic function, and aortic diameter measurements.
All individuals tolerated the initial week of study medication, whether atenolol or losartan, and 100% of patients were able to reach target dosing at 7 days and maintain that dose for the duration of the study.
Measures of vascular stiffness
The effects of both atenolol and losartan on measures of vascular stiffness are detailed in Table 2. PWV decreased significantly in patients treated with atenolol (–1.15 ± 1.68 m/s; p = 0.01), but not in those treated with losartan (–0.22 ± 0.59 m/s; p = 0.15). The difference in effect between the two treatment groups after 6 months of treatment was statistically significant (p = 0.04), indicative of improved aortic stiffness in patients treated with atenolol (Figure 2). The difference in the PWV change between the two treatment groups was unaffected by age, gender, or change in systolic or diastolic blood pressure during the study period. However, the improvement in PWV with atenolol compared with losartan was attenuated when adjusted for change in heart rate (p = 0.22).
Hemodynamic and vascular stiffness measures in response to treatment.
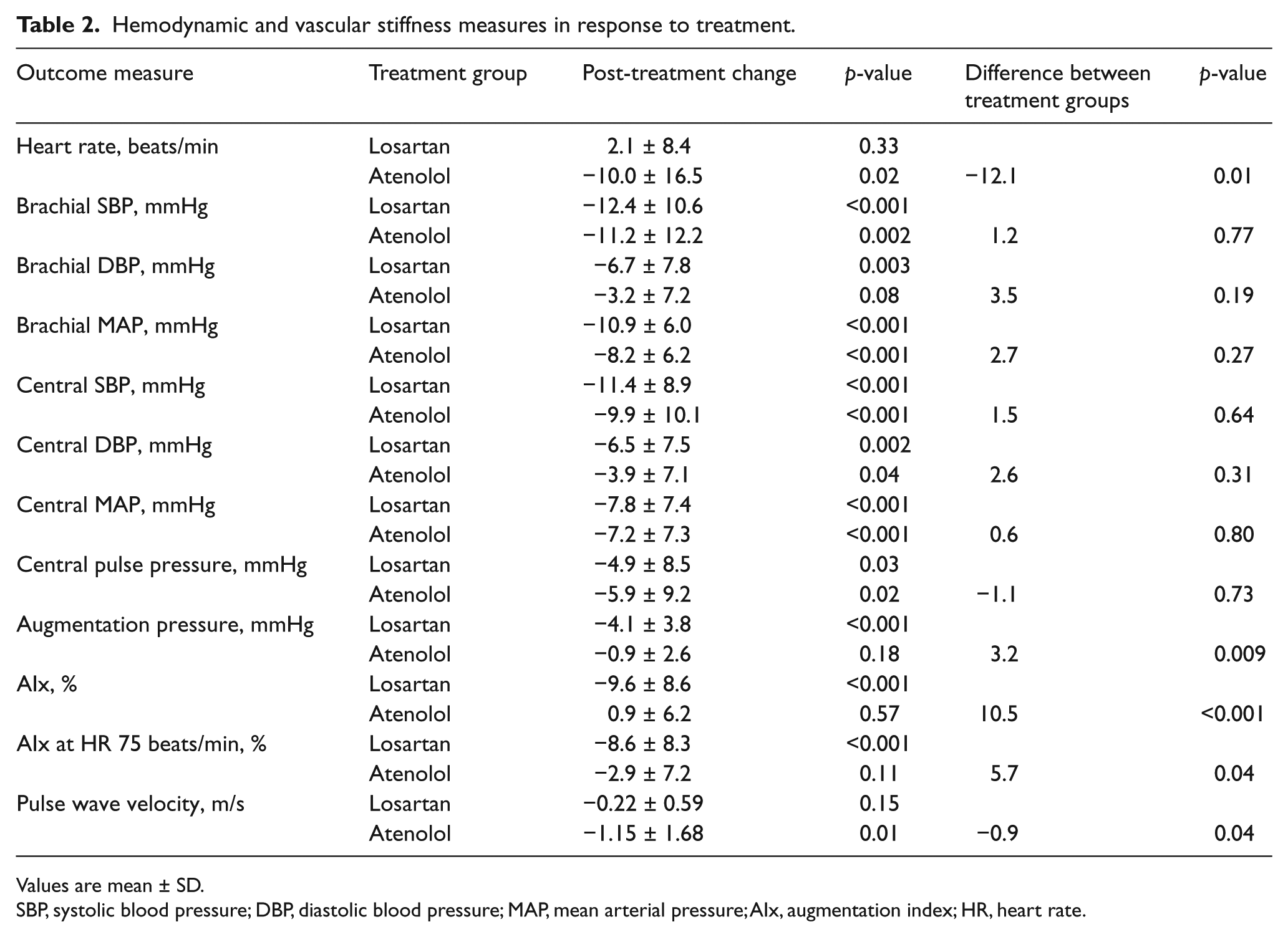
Values are mean ± SD.
SBP, systolic blood pressure; DBP, diastolic blood pressure; MAP, mean arterial pressure; AIx, augmentation index; HR, heart rate.
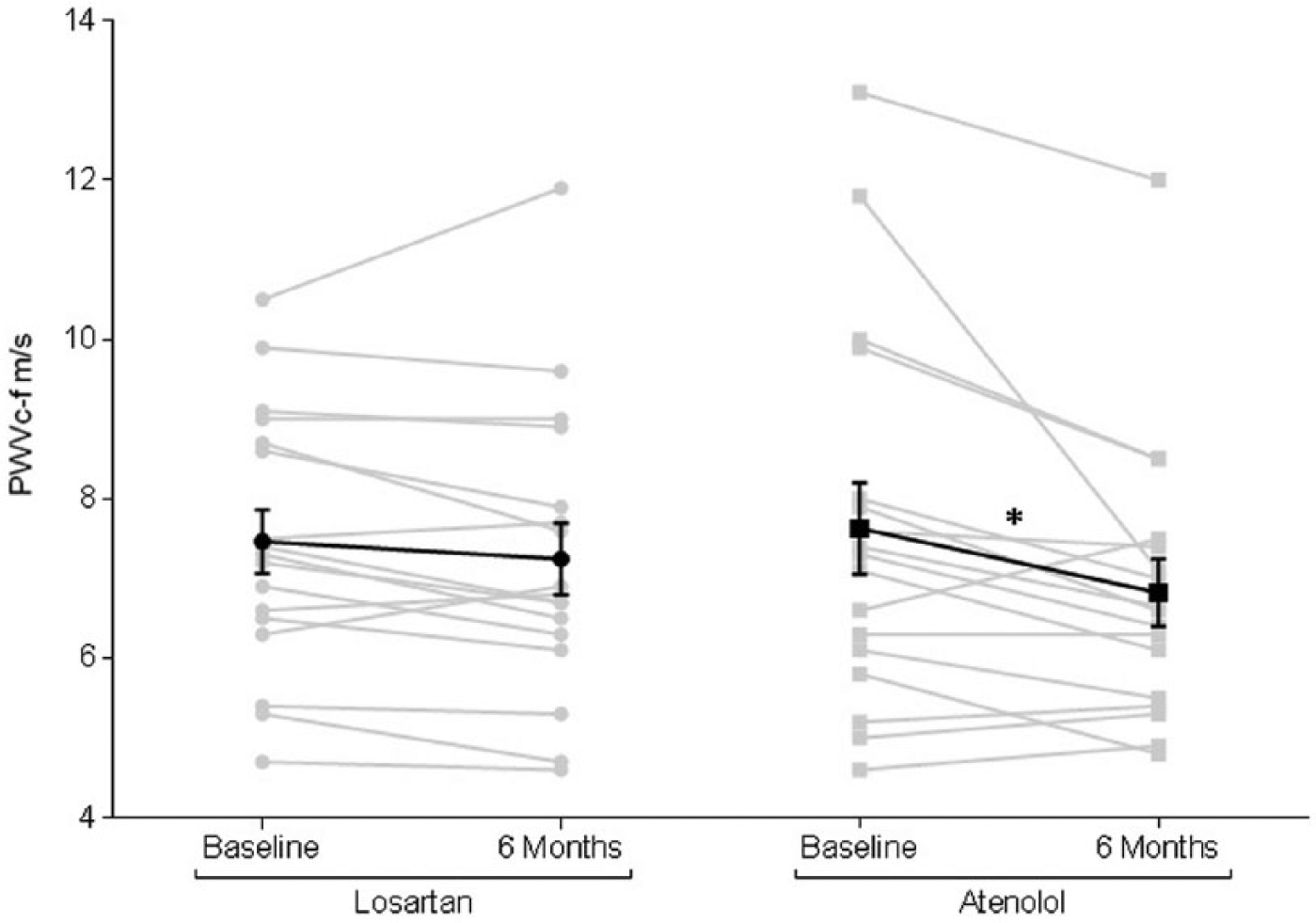
Carotid femoral pulse wave velocity. Individual and mean carotid-femoral PWV (± standard error) in losartan and atenolol groups at baseline and 6 months after randomization. (*p = 0.01, indicative of a significant change in the atenolol treatment group.)
Central augmentation pressure decreased significantly in patients treated with losartan (–4.1 ± 3.8 mmHg, p < 0.001), but not those treated with atenolol (–0.9 ± 2.6 mmHg, p = 0.18), resulting in a significant difference in the change in augmentation pressure between groups (p = 0.009). Consequently, there was a significant decrease in AIx in the losartan group (–9.6 ± 8.6%, p < 0.001) but not the atenolol group (0.9 ± 6.2%, p = 0.57), accounting for a significant difference between groups (p < 0.001). The significance persisted when controlling AIx for heart rate, with a greater response in the losartan (–8.6 ± 8.3%, p < 0.001) compared with the atenolol (–2.9 ± 7.2%, p = 0.11) treatment arm (between-group difference p = 0.04) (Figure 3). The greater lowering (improvement) in AIx with losartan compared with atenolol persisted when controlling for age, gender, change in systolic and diastolic blood pressure and change in heart rate over the study period.
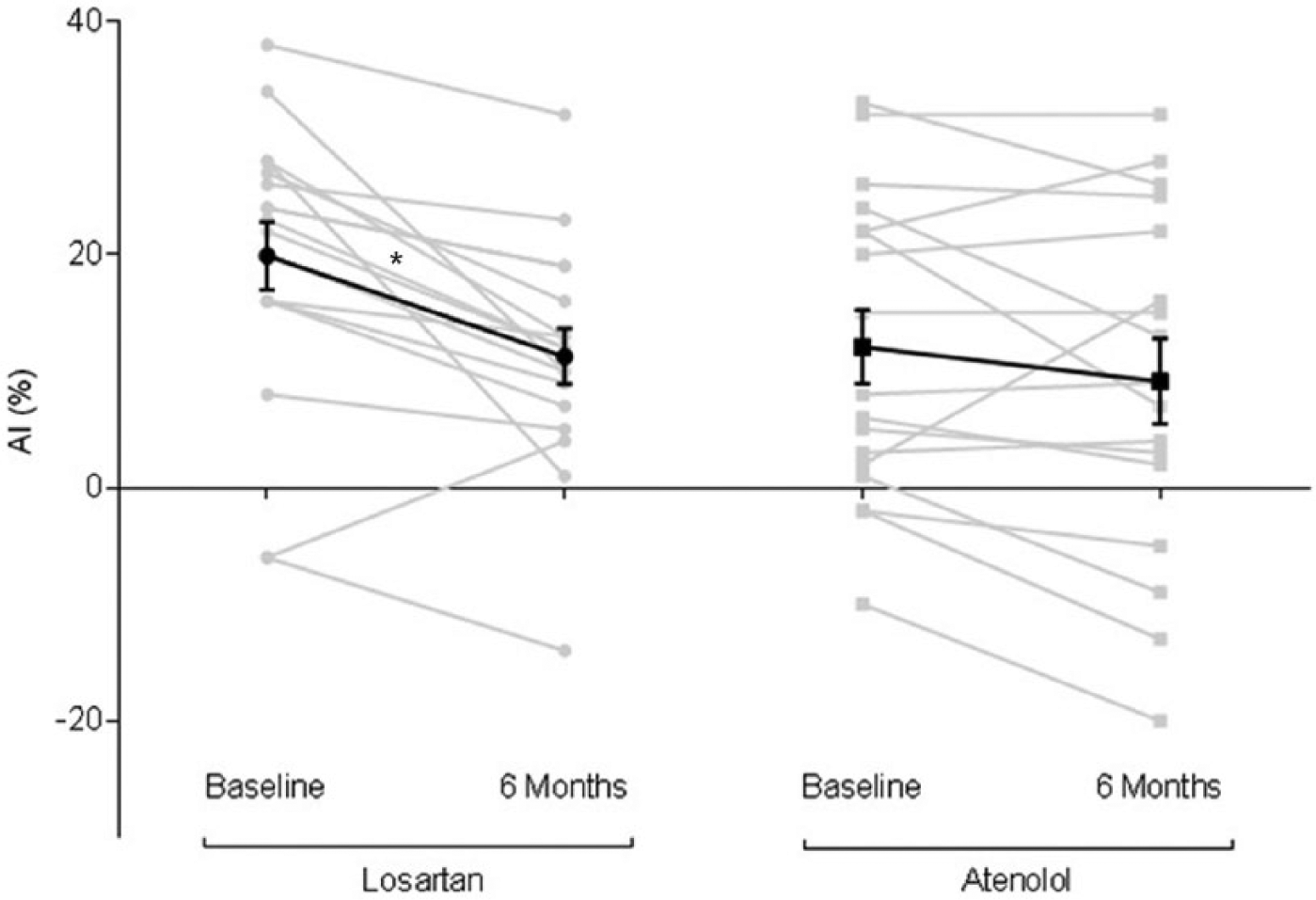
Augmentation index (AIx). Individual and mean AIx (± standard error), standardized to a heart rate of 75 beats/min in the losartan and atenolol groups at baseline and 6 months after randomization. (*p < 0.001, indicative of a significant change in the losartan group.)
Neither the aortic root nor the ascending aortic diameter changed significantly with atenolol or losartan, and there was no significant difference between the treatment groups (Table 3).
Echocardiographic measures in response to treatment.
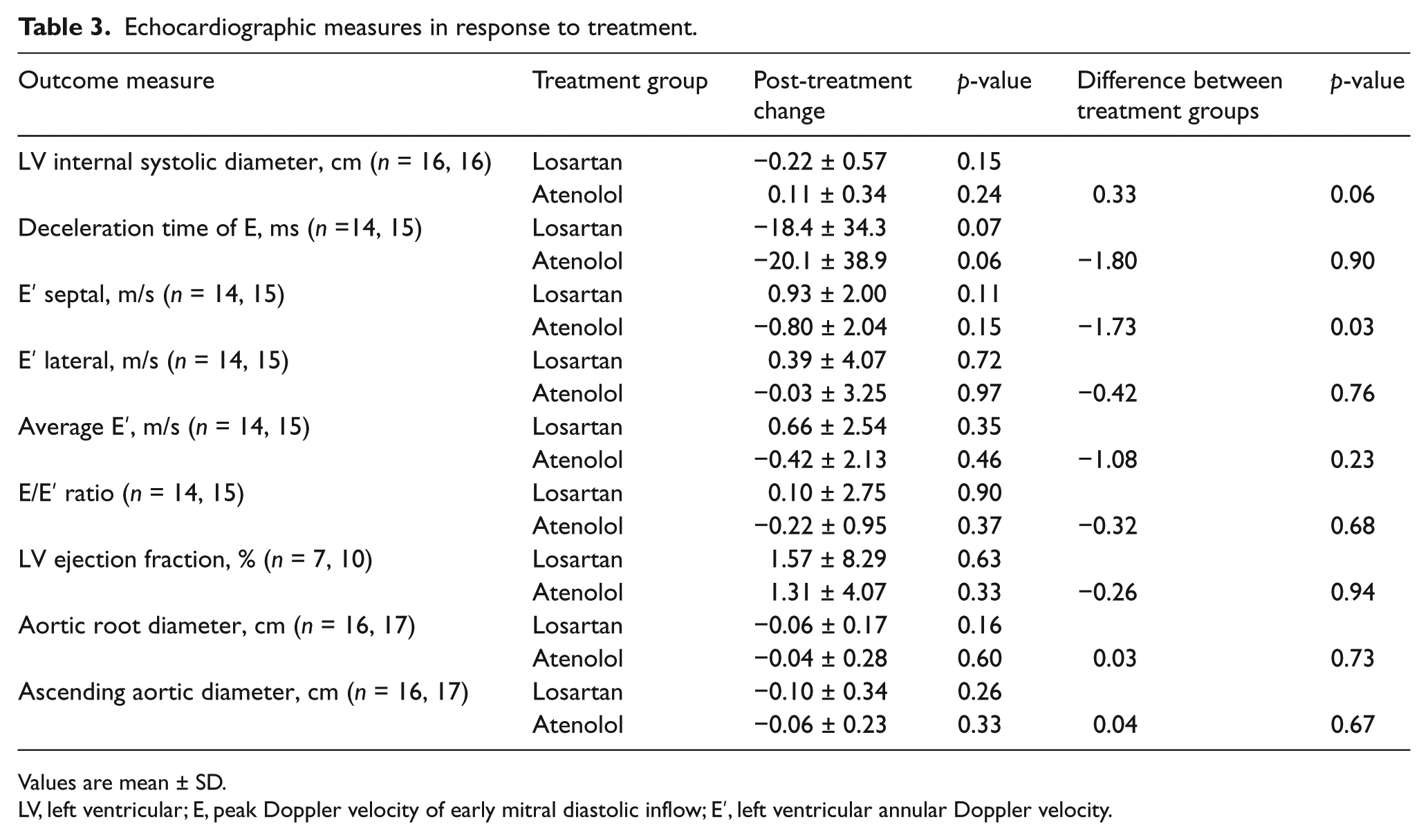
Values are mean ± SD.
LV, left ventricular; E, peak Doppler velocity of early mitral diastolic inflow; E′, left ventricular annular Doppler velocity.
Measures of left ventricular function
Measurements derived from echocardiography are provided in Table 3. Limited echocardiographic windows precluded precise measurements of left ventricular size and function in some patients. The left ventricular ejection fraction did not change in either treatment arm (1.31 ± 4.07% and 1.57 ± 8.29% in the atenolol and losartan groups, respectively). There was no significant difference in the 6-month change in left ventricular ejection fraction between the two groups. E′ septal velocity tended to improve with losartan treatment (0.93 ± 2.00 m/s, p = 0.11) and tended to worsen with atenolol treatment (–0.80 ± 2.04 m/s, p = 0.15) accounting for a significant between-group difference (p = 0.03). There was no change in E′ lateral velocity with either drug and there was no difference between groups. The deceleration time of E tended to decrease with both losartan (–18.4 ± 34.3, p = 0.07) and atenolol (–20.1 ± 38.9, p = 0.06), but there was no significant difference between groups (p = 0.90). There was no change in the E/E′ ratio with either drug and there was no difference between groups.
Discussion
The results of this randomized, double-blind, parallel design study indicate that atenolol and losartan treatment each favorably affect aortic stiffness in adults with Marfan syndrome. Atenolol decreased carotid to femoral PWV, whereas losartan reduced central aortic AIx, implicating different mechanisms through which these drugs improve aortic functional properties.
Individuals with Marfan syndrome have increased aortic stiffness, as evidenced by decreased distensibility and increased PWV and AIx compared to the normal population.8–12,23 Aortic stiffness precedes and independently predicts thoracic aortic dilation in Marfan syndrome, and the risk of aortic dissection and rupture is associated with aortic diameter.13,31,32 Therefore, therapies that prevent or improve aortic stiffness may reduce the risk of aortic complications in patients with Marfan syndrome.
Contemporary practice guidelines recommend that β-adrenergic receptor blocking drugs be administered to all patients with Marfan syndrome and aortic aneurysm to reduce the rate of aortic dilatation. 33 This recommendation stems from an open-label, randomized trial in adolescent and adult patients with Marfan syndrome which found that propanolol decreased the rate of aortic dilatation and reduced aortic complications. 24 This observation was supported by a retrospective study of children with Marfan syndrome which also found that β-blockers reduced the rate of aortic dilatation. 21 However, another study of patients with Marfan syndrome reported that β-blocker therapy resulted in a more heterogeneous response, including both improvement and deterioration of aortic elastic properties. 23 Emerging evidence suggests that ARBs also reduce aortic dilatation. In a study of pediatric patients with Marfan syndrome, ARB therapy, compared with previously administered non-ARB therapies, slowed the rate of progressive aortic-root dilation. 25 In a multicenter, open-label, randomized controlled trial, losartan treatment, compared with no additional treatment, reduced the aortic root dilatation rate in adults with Marfan syndrome. 29
Several studies have assessed the treatment effects of both β-blockers and inhibitors of the renin-angiotensin system on aortic functional and structural characteristics in persons with Marfan syndrome. Some of these focused on young patients; others were limited by low numbers, or lack of randomization and concurrent controls. In a prospective, non-randomized, open-label study of young patients with Marfan syndrome, there was lower aortic stiffness and a smaller increase in aortic root diameter in those treated with enalapril compared with those treated with the β-blockers, propanolol or atenolol. 26 A small crossover trial comparing atenolol, perindopril, and verapamil in adults with Marfan syndrome found that each tended to decrease AIx, but this study lacked power and there was no significant difference between drug treatments. 34 A recent study of 28 pediatric patients with Marfan syndrome and aortic root dilation (z score >2.0) who were randomized to receive β-blocker treatment alone or a β-blocker and losartan for 35 months found that the annual dilation rate of the aortic root was significantly lower with the combined therapy; however, there were no significant differences between these treatment groups in changes of aortic stiffness and cross-sectional compliance. 35 A randomized, double-blind, placebo-controlled trial of 17 adult patients with Marfan syndrome taking β-blocker therapy found that the addition of perindopril compared with placebo reduced both aortic stiffness and aortic root diameter. 36 Most recently, a large multicenter clinical trial compared the effect of losartan with atenolol on slowing aortic root enlargement in 608 young persons with Marfan syndrome. 37 Both drugs decreased the rate of aortic root enlargement relative to body-surface area over the three-year study period and there was no difference in effect between the two treatment groups. These findings indicate that both losartan and atenolol are potentially beneficial in Marfan syndrome. Our study extends previous investigations in that it includes only adult Marfan patients – many of whom have normal aortic dimensions, who do not have prior surgical interventions or aortic events – provides novel comparative functional information between β-blocker and ARB therapy, and suggests a mechanism by which both medications may be beneficial as treatment in this population.
In our study, the effect of atenolol on PWV was significantly greater than the effect of losartan, whereas losartan was more effective in reducing central aortic AIx. These findings are consistent with those in several studies of aortic stiffness in hypertensive patients, which compared atenolol to either an ACE inhibitor or ARB, and found atenolol reduced aortic PWV more effectively than renin-angiotensin system inhibitors, but the latter reduced AIx whereas atenolol did not.38–42
Although PWV and AIx are conceptually related to each other and each is affected by aortic stiffness, drugs may have differential effects depending on their site and mechanism of action. Carotid to femoral PWV relates directly to elastic modulus and is considered the gold standard measurement of arterial stiffness.43,44 The precise mechanism through which β-blockers decrease PWV is not known, though reduction in blood pressure and transfer of stress from collagen to elastin may reduce stiffening of the aortic wall. Alternatively, the bradycardic effect of atenolol may affect PWV, as some, but not all studies have found an association between heart rate and PWV.45–47 PWV may also be influenced by left ventricular ejection time. In our study, adjustment for heart rate attenuated the effect of atenolol on PWV. We did not detect any improvement in left ventricular ejection fraction, but did not measure left ventricular ejection time.
The central AIx is calculated as the difference in pressure between the first and second systolic peaks of the arterial pressure wave form and expressed as a percentage of the pulse pressure. The first peak is due to the forward pressure wave generated by left ventricular systolic contraction, and the second peak incorporates a reflected wave returning centrally from peripheral sites. Both PWV and peripheral impedance influence the speed with which the reflected wave returns and affects central systolic pressure and AIx. Thus, whereas carotid to femoral PWV is a direct measure of aortic stiffness, AIx is an indirect measure of vascular stiffness, which is potentially influenced by drugs or conditions that alter peripheral resistance. 43 In our study, losartan decreased AIx, implicating a slower speed of the reflected wave. As losartan did not change PWV, it is inferred that peripheral impedance was lowered as a consequence of vascular smooth muscle relaxation. Indeed, similar findings have been observed in hypertensive patients who receive ARBs or other vasodilators.48–56
Parameters of left ventricular systolic and diastolic function were assessed in each group to determine if either atenolol or losartan treatment favorably affected myocardial function along with vascular stiffness. Baseline left ventricular ejection fraction was normal in each group. Neither atenolol nor losartan changed the left ventricular ejection fraction. E′ septal, a measure of diastolic function, tended to improve in the losartan group and worsen in the atenolol group, resulting in a significant difference between groups over 6 months of therapy. No other diastolic function parameter changes were significantly different between the two treatment groups. Whether the modest change in E′ septal reflects a direct effect of these drugs on myocardial function, or an indirect effect related to changes in loading conditions, cannot be determined from this study. In clinical trials of antihypertensive therapies, the reduction of systolic blood pressure and arterial stiffness correlated with improvement in diastolic function,57,58 but that association was not investigated in this study.
Limitations
Our study was designed to evaluate the effect of an ARB compared with a β-blocker on aortic stiffness, and was not powered to determine the efficacy of these drugs on change in aortic diameter or preventing acute aortic events. Medications were not titrated to the highest tolerated dose; however, the doses used were those commonly prescribed in clinical practice. Both drugs were well tolerated and no patient-reported side effects. This study did not evaluate the efficacy of both atenolol and losartan in combination, and it would have been interesting to see if the findings observed in each group were additive when the two drugs were used together. We did not include a ‘no-treatment’ group. Treatment of patients with Marfan syndrome with a β-blocker (class I) or ARB (class IIa) is recommended by the ACCF/AHA Thoracic Aortic Disease Guidelines, precluding a no treatment option in most patients for ethical reasons. 59 Unfortunately, enrollment of an adequate number of patients with Marfan syndrome at a single site to achieve sufficient statistical power for another treatment group in a timely manner was not feasible.
Conclusions
Aortic complications, specifically aortic dissection and rupture, are the major source of morbidity and mortality in adults with Marfan syndrome. Aortic stiffness is increased in patients with Marfan syndrome, and this presages aortic dilatation and acute aortic events. Our findings demonstrate that both β-adrenergic blockade and angiotensin receptor blockade improve measures of vascular stiffness, albeit via distinct mechanisms. Based on our observations, there may be a role for both β-blockers and ARBs in the treatment of Marfan syndrome.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the National Marfan Foundation, Port Washington, NY and the American College of Cardiology Merck Fellowship in Cardiovascular and Metabolic Disease, Washington, DC, USA.