
Abstract
While treatment with low-dose aspirin has been established as a therapeutic tool for secondary prevention, the role of aspirin on primary prevention remains controversial. Aortic stiffness and wave reflections are independent predictors of cardiovascular events. The aim of the present study was to investigate the effect of low-dose aspirin on aortic stiffness and wave reflections in hypertensive patients. We studied 30 patients with grade I hypertension. Fifteen patients were treated with 160 mg of aspirin and 15 patients with placebo. Aortic stiffness and wave reflections were assessed by measuring carotid–femoral pulse wave velocity (PWV) and heart rate-adjusted augmentation index (AIx75), respectively. All measurements were conducted at baseline and 2 weeks after treatment. In the aspirin group, there was a significant reduction in PWV compared to the placebo group (from 8.9±1.5 to 8.5±1.6 m/s for the aspirin group vs from 8.6±1.4 to 8.7±1.6 m/s for the placebo group, net change: –0.5 m/s; p=0.02). AIx75 showed a marginal decrease (from 28.0±5.4 to 26.2±5.0% for the aspirin group vs from 31.2±9.7 to 30.6±9.2% for the placebo group, net change: –1.2%; p=0.06). In conclusion, a 2-week course of aspirin administration has a favorable effect on aortic stiffness and, to a lesser extent, on wave reflections in hypertensive patients. Whether the reduction in arterial stiffness is translated to fewer cardiovascular events needs to be confirmed by future prospective studies.
Introduction
While treatment with low-dose aspirin is an established first-line therapy for secondary prevention of cardiovascular disease, 1 mainly due to its antithrombotic properties, the beneficial effects of aspirin on primary prevention have been questioned. The few studies exploring possible beneficial cardiovascular effects of aspirin on primary prevention have shown conflicting results.2–6 Furthermore, the risk-to-benefit ratio has not been fully clarified. Indeed, recent data showed that bleeding events outweigh the potential beneficial effects from the aspirin use. 7 Given the skepticism about the role of aspirin on primary prevention, current guidelines recommend that prophylactic use of low-dose aspirin might be considered in well-controlled hypertensive patients with reduced kidney function or at high cardiovascular risk 8 and in diabetic patients at increased cardiovascular risk (10-year risk >10%). 9 Recently, investigators proposed a high coronary artery calcium score as a guide for aspirin use in primary prevention, 10 whereas a more recent position statement suggests the use of low-dose aspirin for primary prevention in patients with an estimated 10-year risk of major cardiovascular events >20%. 11
Aortic stiffness and wave reflections are independent predictors of cardiovascular events in several populations, including hypertensives.12–17 Furthermore, aortic stiffness is independently related to inflammatory status in hypertensive patients.18–21 Many interventional studies have demonstrated the beneficial effect of anti-inflammatory drugs22,23 or cardiovascular drugs with anti-inflammatory properties, such as statins,24,25 on aortic stiffness. Moreover, the favorable effect of the anti-inflammatory dose of aspirin on arterial stiffness has been demonstrated: indeed, previous data on healthy subjects from our department showed that inflammation is implicated in the pathophysiology of aortic stiffness, while treatment with a high dose of aspirin (anti-inflammatory dose) eliminated the increase in PWV induced by inflammation. 26 Nevertheless, the impact of low-dose aspirin on aortic stiffness is less clear.
Given first, the prognostic value of aortic stiffness in hypertensive patients and second, the previous knowledge on the association between aortic stiffness and inflammatory status in hypertensive patients, as well as the beneficial effects of anti-inflammatory agents on aortic stiffness, the aim of the present study was to assess the effect of low-dose aspirin on aortic stiffness in hypertensive patients.
Methods
Study design
This is a randomized, placebo-controlled study. We enrolled 30 non-diabetic, never-treated hypertensive patients, recruited from the Peripheral Vessels and Hypertension Unit of our department. Fifteen patients were allocated to treatment with 160 mg of aspirin and 15 patients with placebo. All hemodynamic measurements were conducted at baseline (day 1) and 2 weeks after treatment (day 15).
Office blood pressure (BP) was measured by an auscultatory sphygmomanometer, taking at least three measurements spaced by 1 minute, allowing the patients to rest for 10 minutes before examination. According to the guidelines of the European Society of Hypertension, measurement of systolic blood pressure (SBP) ≥140 mmHg and diastolic blood pressure (DBP) ≥90 mmHg were considered as systolic and diastolic arterial hypertension, respectively. Hypertension grade I was defined as SBP of 140–159 mmHg and/or DBP of 90–99 mmHg. Pulse pressure (PP) was calculated as SBP minus DBP and mean arterial pressure (MAP) as DBP +1/3 PP. The inclusion criterion of hypertension grade I was chosen to avoid possible adverse effects from aspirin use in patients with very high BP levels. Anti-hypertensive treatment was started immediately after the completion of the study, as appropriate.
Body weight and height were measured in all subjects and body mass index (BMI) was calculated. Smoking status was assessed by recording the habit of smoking. Patients with secondary hypertension, cerebrovascular disease, coronary heart disease, severe heart valvular disease and chronic, systematic diseases were excluded from the study. Use of anti-inflammatory agents, including statins, was also an exclusion criterion.
All participants gave their informed consent to participate in the study, which was approved by the Local Ethics Committee.
Aortic stiffness and wave reflections evaluation
Aortic stiffness was evaluated non-invasively by the measurement of carotid–femoral PWV. Carotid–femoral PWV, an established marker of aortic stiffness, 13 was obtained using a validated non-invasive device (Complior®, Artech Medical, Pantin, France), 27 which allows online pulse-wave recording and automatic calculation of PWV. Two different pressure-waveforms were obtained simultaneously at two sites: the right carotid and femoral artery. The time delay (t) between the feet of the recorded proximal and distal waves was automatically calculated. For the carotid–femoral segment, the distance (d) was estimated by subtracting the distance between carotid location and sternal notch from the distance between sternal notch and femoral site. The mean PWV of at least 10 consecutive pressure waveforms was calculated for further analysis.
Augmentation index (AIx) was measured as an index of wave reflections. AIx is a composite measure of the magnitude of wave reflection and aortic stiffness which affects timing of wave reflections. Augmented pressure (AP) is the pressure added to the incident wave by the returning reflected wave and represents the increased afterload that the left ventricle must cope with. AIx is defined as AP divided by central pulse pressure and is expressed as a percentage. The peripheral pulse wave was recorded from the radial artery using the method of applanation tonometry. The radial pulse wave was transformed into the central pulse wave of the aorta through analysis of the pulse wave with the SphygmoCor device (AtCor Medical, Sydney, Australia).28,29 Measurements were performed by a single investigator. AIx was averaged from 10 to 12 successive waves and it was corrected for a steady heart rate of 75 beats/min (AIx75).
All measurements were conducted in the morning, with the individual in the supine position, in a quiet environment. Participants were requested to abstain from tobacco, coffee and food at least 5 hours and from alcohol 12 hours before the examination.
Laboratory assays
Blood samples were taken between 8.00 and 9.00 in the morning after an overnight fast. The white blood cell (WBC) and platelet (PLT) count were measured in all subjects. Routine biochemical parameters, including blood glucose and lipids (total cholesterol, low-density cholesterol and triglycerides), were also determined at baseline with standard techniques by an autoanalyzer. Inflammatory status was assessed by measuring high-sensitivity C-reactive protein (hsCRP) using an immunonephelometric method (Dade Behring High Sensitivity CRP assay; Dade Behring, Marburg, Germany). The upper normal limit of hsCRP was 3 mg/L with intra and inter-assay coefficients of variation <4.4 and 5.7%, respectively). High-sensitivity CRP was measured in all participants at baseline and 2 weeks after treatment.
Statistical analysis
We hypothesized that aspirin treatment would produce an absolute decrease of 0.7 m/s in PWV, a clinically meaningful change according to previous studies. Given a standard deviation of 0.9 m/s, a representative value of similar populations, we calculated that 13 patients in two equal groups would provide 80% power at the 5% level of significance. To ensure confidence we recruited 30 patients who were allocated into two equal treatment groups. Patients were randomized to their assigned treatment group using appropriate statistical software and sequentially numbered sealed envelopes.
Continuous variables are presented as mean value ± 1 standard deviation, whereas qualitative variables are presented as absolute and relative frequencies. Statistical normality was checked with the Kolmogorov–Smirnov test. High-sensitivity CRP was log-transformed due to its skewed distribution.
The difference in baseline characteristics between the two groups was studied using the independent-samples t-test. Analysis of difference in categorical data was carried out with the chi-squared test. Pearson’s correlation was used, in the whole population, to test the associations of PWV and AIx75 with the baseline characteristics. The difference in aortic stiffness, wave reflections, hemodynamic parameters and hsCRP levels between the two groups, from day 1 to day 15, was investigated with the ANOVA for repeated measures. Exact p-values <0.05 were considered as statistically significant. Data analysis was performed with SPSS software, version 17.0 (Chicago, IL, USA).
Results
Baseline characteristics of the two groups of patients are presented in Table 1. No difference was observed in the level of peripheral SBP, DBP, PP and heart rate between the two groups at baseline (day 1) (p=NS). Moreover, patients did not differ in the levels of serum glucose, total cholesterol, low-density lipoprotein (LDL) cholesterol and triglycerides (p=NS). Platelet and WBC count did not show a significant difference between the two groups (p=NS). Patients in the aspirin group had similar levels of hsCRP compared to the placebo group (p=NS).
Baseline characteristics of the two groups of hypertensive patients.
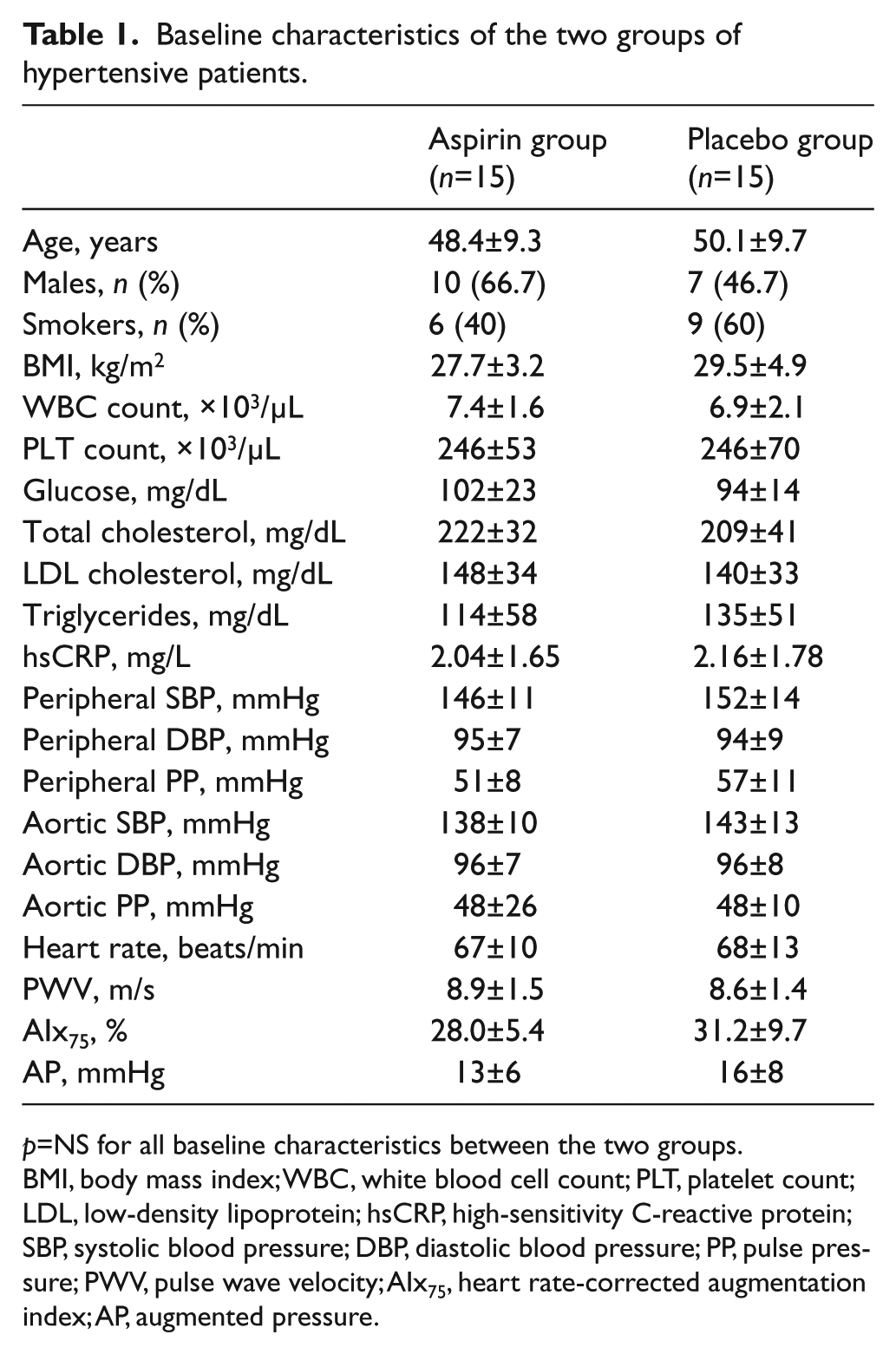
p=NS for all baseline characteristics between the two groups.
BMI, body mass index; WBC, white blood cell count; PLT, platelet count; LDL, low-density lipoprotein; hsCRP, high-sensitivity C-reactive protein; SBP, systolic blood pressure; DBP, diastolic blood pressure; PP, pulse pressure; PWV, pulse wave velocity; AIx75, heart rate-corrected augmentation index; AP, augmented pressure.
Baseline values of PWV and AIx75 did not differ between aspirin and placebo groups (p=NS) (Table 1). Following the same trend, aortic SBP, DBP and PP levels were similar between the groups (p=NS) (Table 1). In the whole population, PWV correlated with age (r=0.47, p=0.008) and glucose concentration (r=0.43, p=0.02). AIx75 was associated with age (r=0.38, p=0.04), female sex (r=0.44, p=0.01) and inversely with DBP (r = −0.38, p=0.04).
The hemodynamic parameters (peripheral and aortic SBP, peripheral and aortic DBP, and heart rate), from day 1 to day 15, did not differ significantly between the two groups (Table 2). After 2 weeks of treatment, a significant decrease in PWV was demonstrated in the aspirin group, whereas no significant change was observed in the placebo group (from 8.9±1.5 to 8.5±1.6 m/s for the aspirin group vs from 8.6±1.4 to 8.7±1.6 m/s for the placebo group, net change: –0.5 m/s; p=0.02) (Figure 1). Similarly, there was a trend for a decrease of AIx75 in hypertensive patients treated with aspirin, compared to placebo, but reaching only a marginally statistical significant level (from 28.0±5.4 to 26.2±5.0% for the aspirin group vs from 31.2±9.7 to 30.6±9.2% for the placebo group, net change: –1.2%; p=0.06).
Hemodynamic parameters and hsCRP levels after 2 weeks of aspirin administration.
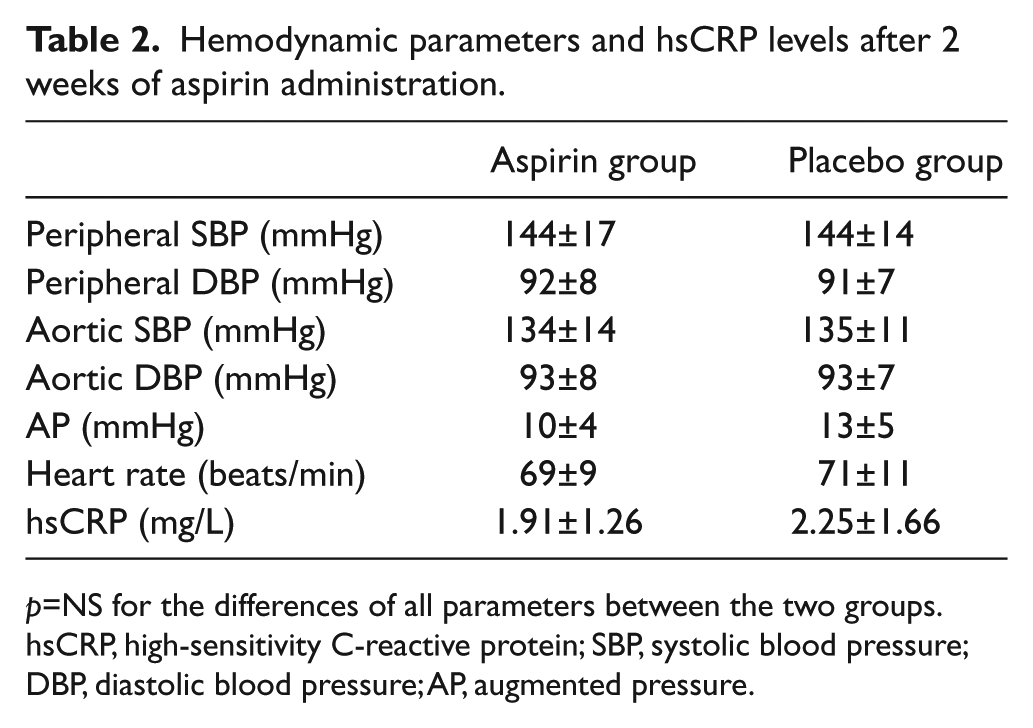
p=NS for the differences of all parameters between the two groups.
hsCRP, high-sensitivity C-reactive protein; SBP, systolic blood pressure; DBP, diastolic blood pressure; AP, augmented pressure.
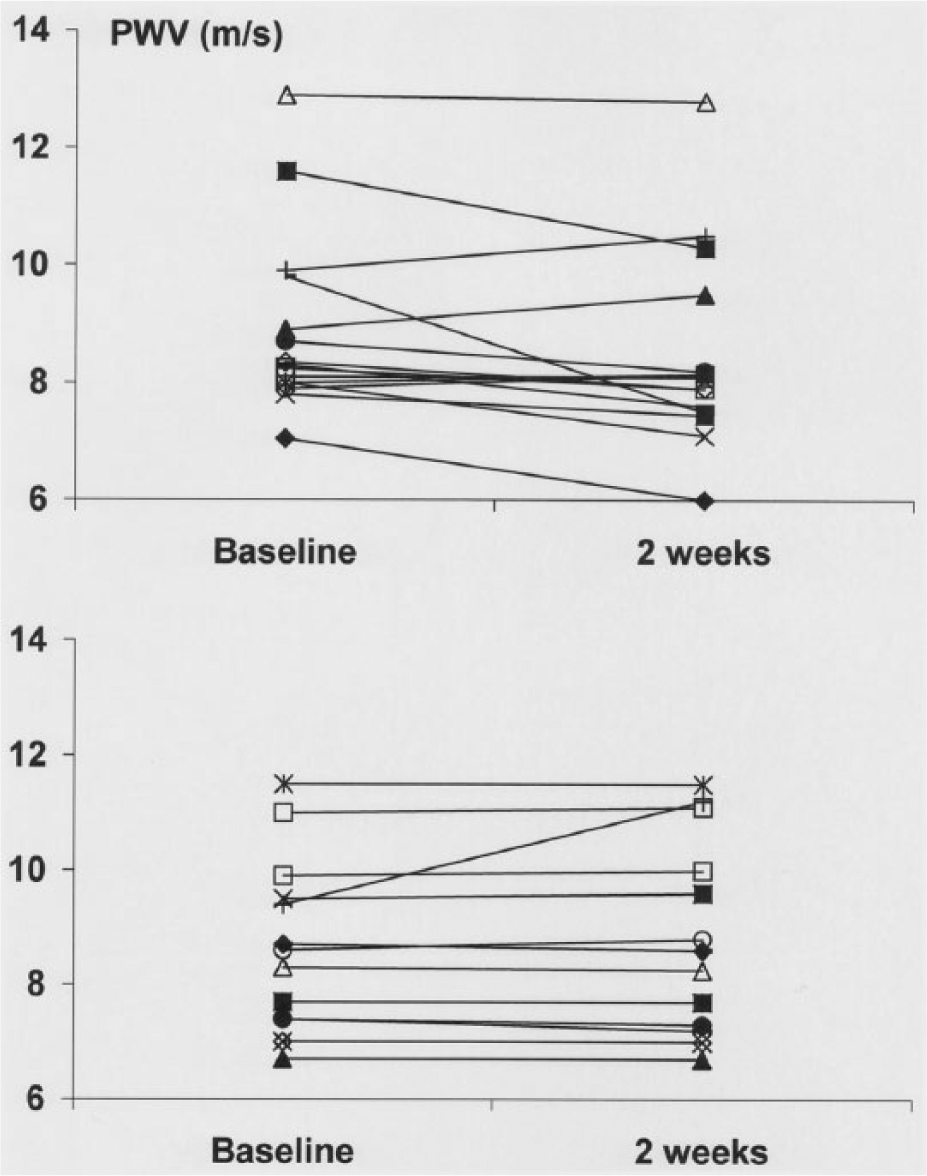
Change in pulse wave velocity (PWV, m/s) in each hypertensive patient treated with 160 mg of aspirin (upper panel) compared to placebo (lower panel) after 2 weeks of treatment.
Discussion
The present study highlights, for the first time, the beneficial effect of low-dose aspirin on aortic stiffness in the hypertensive population. Considering that aortic stiffness is a powerful, independent predictor of cardiovascular events in hypertensive patients, this finding may have important clinical implications. However, the present results need to be confirmed by future, prospective studies that will further show whether a decrease in aortic stiffness after aspirin treatment is associated with lower rates of cardiovascular events.
Effect of aspirin on aortic stiffness and wave reflections: possible pathophysiological links
Apart from the pathophysiological mechanism of inflammation, inhibition of platelet reactivity, which may be increased in hypertensive patients, might serve as another contributor to the protective effects of low-dose aspirin on aortic stiffness. In a large sample of the general population, a recent study demonstrated an independent relationship between ankle–brachial PWV and mean platelet volume, an indicator of platelet activation. 35 In addition, previous data have shown that activated platelets express P-selectin, a glycoprotein that enhances endothelial dysfunction and has been associated with carotid thickness and stiffness. 36 Activated platelets promote endothelial dysfunction also through release of proinflammatory cytokines, suggesting a novel mechanism of inflammatory-mediated vessel wall injury by platelets.37,38 Considering that endothelium-derived nitric oxide regulates arterial elasticity, platelet reactivity might play an integrated role in the crosstalk between endothelial dysfunction and arterial stiffness.39,40
Finally, the tendency for a reduction in wave reflections after aspirin administration, as this was observed by the present study, might be explained by the reduction of aortic stiffness. Considering the augmentation index depends both on the timing of the reflected wave (and thus, from aortic stiffness) and on the magnitude of the wave reflections, the lack of a statistically significant reduction might be ascribed to the absence of reduction in the magnitude of wave reflections which are determined by peripheral resistance. Nevertheless, further studies need to confirm this observation and elucidate the possible underlying mechanism.
Limitations
The present study has some limitations. We investigated the effect of low-dose aspirin on aortic stiffness and wave reflections in hypertensive patients. Whether this finding also applies in different populations is unclear. In addition, given the 2-week course of aspirin treatment, no assumptions can be made on the long-term efficacy of aspirin on aortic stiffness. Furthermore, although this is an interventional study, no definite pathophysiological relationships can be demonstrated. Nevertheless, given that the beneficial effect of aspirin was exerted in a relatively short time, it could be argued that this was mediated by functional vascular changes (e.g. changes in endothelial function and resultant changes in vascular tone) rather than structural changes of the aortic wall which require a longer period of treatment to realize. Finally, the small sample size, although pre-specified, is another limitation of the study. While the difference in aortic stiffness after aspirin administration was evident, the change in wave reflections was marginally significant, a finding that might have been different in a larger population.
Conclusion
The present study highlights, for the first time, a favorable effect of low-dose aspirin on aortic stiffness in hypertensive patients. Although no etiological relationships can be established and the underlying pathophysiological mechanisms remain unraveled, this novel finding offers new insights into the pathways that might be implicated in the process of aortic stiffening and provides the substrate for further investigation. The confirmation of the present results by larger studies and its extension on different populations may have important clinical implications related to the beneficial effect of aspirin.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The present study was, in part, funded by the Hellenic Cardiovascular Research Society.