
Abstract
We compared the associations of diabetes mellitus (DM) and other cardiovascular disease (CVD) risk factors with decline in the ankle–brachial index (ABI) over 4 years in participants with and without peripheral artery disease (PAD). A total of 566 participants, 300 with PAD, were followed prospectively for 4 years. Mean (SD) baseline ABI values were 0.70 (0.13) for participants with both PAD and DM, 0.67 (0.14) for participants with only PAD, 1.10 (0.13) for participants with only DM, and 1.10 (0.10) for participants with neither PAD nor DM. After adjusting for age, sex, and baseline ABI, the corresponding ABI change from baseline to 4-year follow-up were −0.02, –0.04, +0.05, and +0.05, respectively. Compared to participants with neither PAD nor DM, participants with only PAD showed significantly more ABI decline (p <0.01), while the decline in participants with both PAD and DM was borderline non-significant (p = 0.06). After adjustments for baseline ABI, age, sex, African American ethnicity, and other CVD risk factors, independent factors associated with ABI decline in participants with PAD in the lower ABI leg were older age and elevated D-dimer. DM was not related to ABI decline. Despite being an important risk factor for PAD, DM was not independently associated with ABI decline. This could reflect the effect of DM promoting both PAD and lower-extremity arterial stiffness, resulting in a small decline in the ABI over time. In conclusion, ABI change over time in persons with diabetes may not accurately reflect underlying atherosclerosis.
Keywords
Introduction
The ankle–brachial index (ABI) is the ratio of systolic blood pressure (SBP) at the ankle divided by SBP at the arm, and is a standard primary diagnostic tool used to identify individuals with peripheral artery disease (PAD). 1 A low ABI (<0.90) has good sensitivity and excellent specificity for detecting PAD compared to the angiographic gold standard. 2 Compared to individuals with a normal ABI (0.90–1.30), individuals with PAD have poorer physical functioning, more rapid mobility loss, greater functional decline, and have an increased risk of incident cardiovascular events.3–8
Diabetes mellitus (DM) is an important risk factor for PAD, including limb loss, but also can be associated with stiff lower-extremity arteries.9–11 Stiff ankle arteries lead to falsely-normal or high ABI values (ABI >1.3) since, in this setting, the measured ankle SBP may reflect arterial wall stiffness rather than just the inter-arterial blood pressure. Thus, DM could promote lowering of the ABI due to atherosclerosis, or increase the ABI due to stiff vessels. This dichotomy may limit the prognostic value of the ABI in diabetic patients.
Few studies have evaluated longitudinal decline in the ABI in patients with PAD. ABI decline may serve as an important marker for adverse PAD outcomes. The aim of this study was to determine the characteristics associated with ABI decline over time, with a primary focus on DM.
Methods
Study participants
We studied individuals from the Walking and Leg Circulation Study (WALCS) and WALCS II cohorts. 12 WALCS consisted of 740 participants (age 55 or older) with and without PAD recruited between October 1998 and January 2000. WALCS II included 414 WALCS participants attending their fourth annual visit and 425 newly identified persons (age 59 or older) with and without PAD enrolled between November 2002 and May 2004. 13 In both WALCS and WALCS II, persons with PAD were identified from consecutive patients diagnosed with PAD from three Chicago-area non-invasive vascular laboratories. Participants without PAD were identified from among consecutive patients with normal lower-extremity arterial testing identified from the same three Chicago-area non-invasive vascular laboratories, and from a large general internal medicine practice at Northwestern Medical Center. Participants attended a baseline study visit, and returned for annual follow-up. The Institutional Review Board at Northwestern University and Catholic Health Partners Hospital approved the protocol. All participants gave informed consent.
Exclusion criteria
Exclusion criteria for both WALCS cohorts have been reported.6,14 Participants with dementia, knee amputations (above or below the knee) and recent major surgery (within 30 days) were excluded from this study. Participants who did not speak English, were confined to a wheelchair, or resided in a nursing home were also excluded from participation.
Ankle–brachial index
Systolic pressures in the bilateral brachial, dorsalis pedis and posterior tibial arteries were measured twice with a hand-held Doppler probe (Nicolet Vascular Pocket-Dop II; Nicolet Biomedical, Golden, CO, USA). The ABI was calculated by dividing the mean of the dorsalis pedis and posterior tibial pressures in each leg by the mean of all four brachial pressures. Because of possible subclavian stenosis, when one brachial artery pressure was greater than the opposite brachial arterial pressure in both measurement sets and the right and left brachial arterial pressures differed by at least 10 mmHg, the average brachial pressures in the arm with the highest pressure were used to calculate the ABI for both legs. 15 PAD was defined as an ABI <0.90. The lower of the right and left ABI values was used to determine PAD status.
Co-morbidity and risk factor assessments
Information was obtained from patient report, physical examination, laboratory values, primary care physician questionnaire, and assays of venous blood. The number of cardiovascular diseases was determined using established co-morbidity algorithms from The Women’s Health and Aging Study (i.e. DM, hypertension, myocardial infarction, stroke, and heart failure). 16 Cigarette smoking history was obtained from patient self-report. Participants brought in their medication bottles to ascertain medication use. Baseline measurements of height and weight were used to calculate body mass index (BMI) as (weight [kg]/height [m]2).
D-dimer and C-reactive protein (CRP)
Blood specimens were collected and stored at –70°C until the time of measurement. An Asserachrom D-Di kit (Diagnostica Stago, Parsippany, NJ, USA) was used to measure D-dimer using an ELISA procedure. The Asserachrom D-Di kit has a lower detection limit of 5 ng/ml. Concentrations of high-sensitivity CRP were determined using an immunoturbidimetric assay on the Hitachi 917 analyzer (Roche Diagnostics, Indianapolis, IN, USA) using reagents and calibrators from Denka Seiken (Niigata, Japan). This assay has a sensitivity of 0.003 mg/dl.
Total and HDL cholesterol
Total cholesterol was measured with an enzymatic reaction (peroxidase/phenol-4-aminophenazone indicator reaction). 17 High-density lipoprotein (HDL) cholesterol was measured with direct enzymatic colorimetric assay. 18
Leg symptoms
The San Diego Claudication Questionnaire was used to classify PAD participants into one of four groups based on leg symptoms. 19 The categories are as follows: (1) asymptomatic; (2) intermittent claudication (IC, calf pain on exertion that does not begin at rest, causes the participant to stop walking, and resolves within 10 minutes of rest); (3) leg pain on exertion and rest (different from critical limb ischemia (leg pain at rest, ulcers, or gangrene)); and (4) atypical leg pain on exertion.12,20
Statistical analysis
Our analysis includes 566 participants, mostly Caucasian and African American (there were low frequencies of Hispanic and Asian American ethnicity) who had an ABI at baseline and at the 4-year follow-up. Our study sample size was derived in the following steps: the first step presented the initial cohort; the second step excluded limbs without our outcome (ABI change between baseline and 4-year follow-up); and the final step excluded limbs with revascularization (either prior to baseline, or during 4-year follow-up). We excluded 240 limbs with revascularization prior to or during follow-up. Combining WALCS and WALCS II together, there were 489 (312 + 177) lower ABI legs and 555 (358 + 197) higher ABI legs. There were 77 participants with higher ABI legs but not lower ABI legs, and 11 participants with lower ABI legs but not higher ABI legs in our analysis. This resulted in our current study sample of 566 participants contributing 1044 limbs free from revascularization. Limbs with revascularization during the 4-year follow-up period were included in time to event (interval censoring) analyses for the composite endpoint of ABI decline ≥0.15 or revascularization. The latter analysis resulted in a larger sample size of 956 participants.
Cohort characteristics were summarized by mean (SD) for continuous variables, and proportions (n) for categorical variables. Participants were assigned to four groups: both PAD and DM, only PAD, only DM, and neither PAD nor DM. Linear regression models were used to compare ABI change from baseline to year 4 in all four groups. Time to event (interval censoring) analyses were used to determine the likelihood of the combined outcome of ABI decline ≥0.15 or revascularization. For both linear regressions and time to event analyses, participants with neither PAD nor DM were the reference group, and adjustments were made for baseline ABI, age, and sex. Step-wise selection multivariable linear regression models (p <0.1 criterion) were used to determine independent associations of ABI change, first for the entire cohort, and then stratified by PAD status. Baseline ABI, age, sex, African American ethnicity, BMI, cigarette smoking status, pack-years of smoking, total cholesterol, HDL cholesterol, hypertension, DM, use of statin medications, CRP, D-dimer, number of cardiovascular diseases, and leg symptoms were included in the initial model. Baseline ABI, age, sex, ethnicity, leg symptom classification, and diabetes were forced into the final models. A p-value <0.05 was considered statistically significant. A multiplicative term, DM*baseline ABI, was used to test for interaction in the final models for the entire cohort (p <0.1 was considered statistically significant).
Sensitivity analysis was conducted to determine the effect of excluding limbs with revascularization during the 4-year follow-up. These included: (1) carrying forward ABI values obtained prior to revascularization; and (2) using imputed ABI values calculated from imputation and variance estimation software (IVEware; University of Michigan, Ann Arbor, MI, USA). All analyses were conducted on SAS version 9.3, were limb-specific, and conducted separately for the lower and higher ABI limb.
Results
Among 566 participants from the WALCS and WALCS II cohorts who met eligibility criteria for our study, 72.3% were recruited from the vascular lab, and 27.7% from internal medicine practices. The mean age was 71 ± 8 years, and 53% had PAD (Table 1). Compared to participants without PAD, those with PAD had a lower baseline ABI, were older, less likely to be African American, more likely to be male, and more likely to be diagnosed with DM.
Baseline clinical characteristics among participants with and without peripheral artery disease.
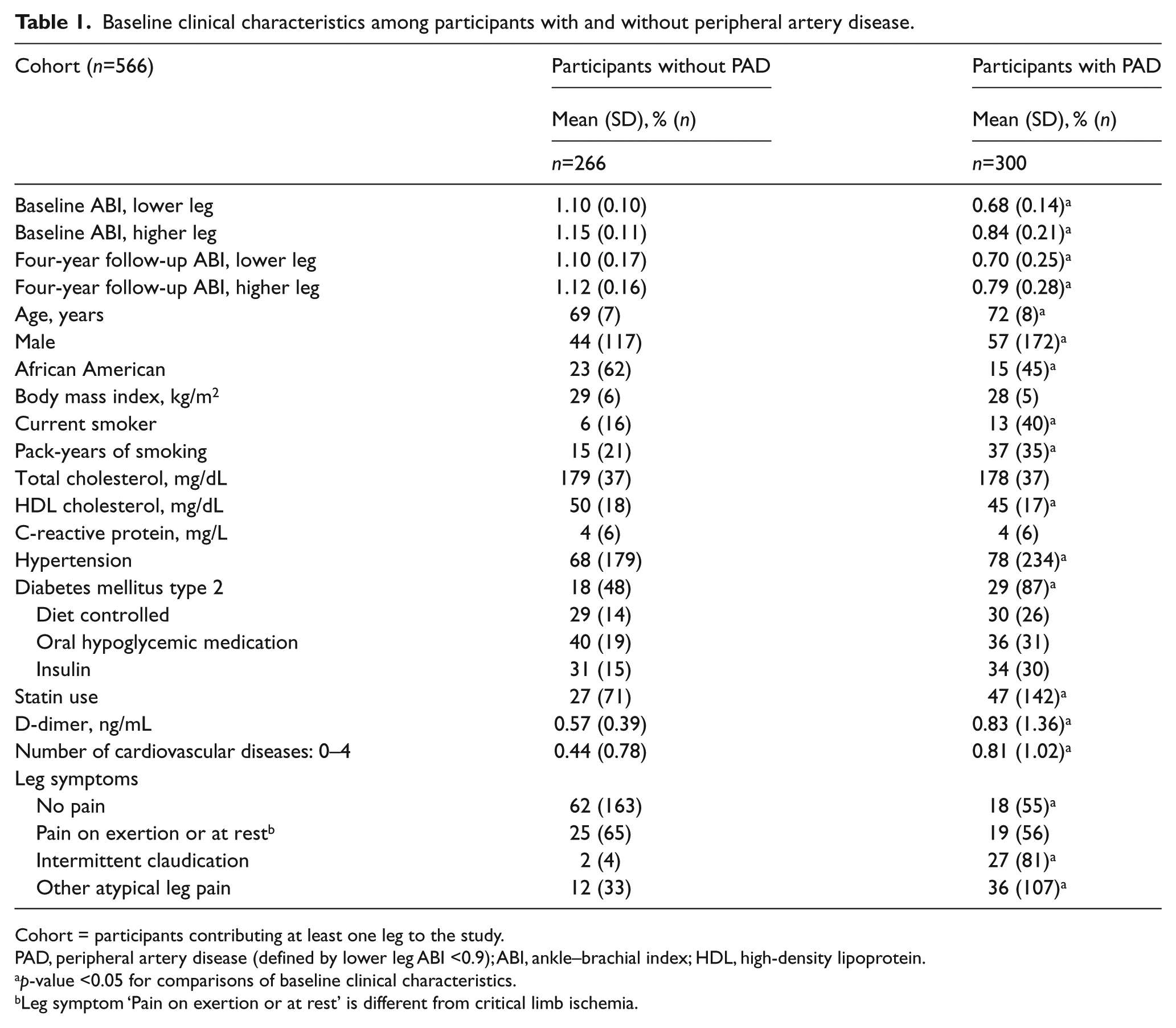
Cohort = participants contributing at least one leg to the study.
PAD, peripheral artery disease (defined by lower leg ABI <0.9); ABI, ankle–brachial index; HDL, high-density lipoprotein.
p-value <0.05 for comparisons of baseline clinical characteristics.
Leg symptom ‘Pain on exertion or at rest’ is different from critical limb ischemia.
When examining the leg with the lower ABI at baseline, mean (SD) baseline ABI values were 0.70 (0.13) for participants with both PAD and DM, 0.67 (0.14) for participants with only PAD, 1.10 (0.13) for participants with only DM, and 1.10 (0.10) for participants with neither PAD nor DM (Table 2). After adjusting for age, sex, and baseline ABI, corresponding ABI changes by group from baseline to 4-year follow-up were −0.02 (95% CI: –0.08, 0.03), –0.04 (95% CI: –0.09, 0.001), +0.05 (95% CI: –0.01, 0.11), and +0.05 (95% CI: 0.02, 0.09), respectively. Compared to participants with neither PAD nor DM, participants with only PAD showed significant ABI decline (p < 0.01) while decline in participants with both PAD and DM was borderline non-significant (p = 0.06). Also, the change in ABI for those with only DM was not significantly different from those with neither PAD nor DM (p = 0.99). For the leg with a higher ABI at baseline, the mean (SD) baseline ABI was 0.84 (0.25) for participants with PAD and DM, 0.84 (0.18) for participants with only PAD, 1.15 (0.13) for participants with only DM, and 1.15 (0.11) for participants with neither PAD nor DM (Table 2). After adjusting for age, sex, and baseline ABI, corresponding ABI changes at the 4-year follow-up were −0.07 (95% CI: –0.11, –0.03), –0.07 (95% CI: –0.01, –0.04), +0.02 (95% CI: –0.04, 0.07), and −0.02 (95% CI: –0.04, 0.01), respectively. Compared to participants with neither PAD nor DM, the ABI change in participants with both PAD and DM was borderline non-significant, while participants with only PAD showed significant decline. In both lower and higher ABI leg analyses, no significant differences were observed when comparing participants with both PAD and DM versus participants with only PAD, though in the higher leg the coefficient was positive for DM only and negative for neither DM nor PAD (p = 0.23 for difference).
Average change in ankle–brachial index from baseline to 4-year follow-up.
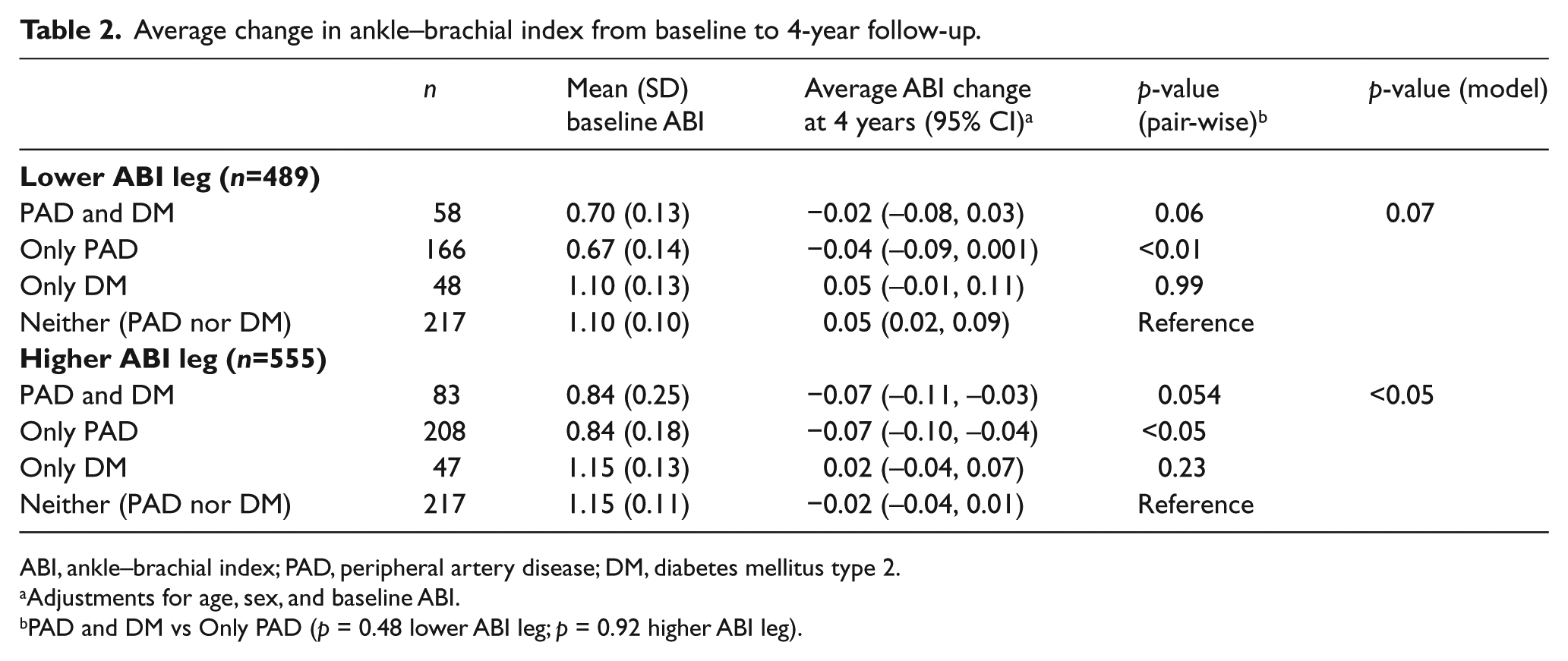
ABI, ankle–brachial index; PAD, peripheral artery disease; DM, diabetes mellitus type 2.
Adjustments for age, sex, and baseline ABI.
PAD and DM vs Only PAD (p = 0.48 lower ABI leg; p = 0.92 higher ABI leg).
Table 3 shows hazard ratios for the likelihood of the combined outcome of ABI decline ≥0.15 or revascularization from baseline to 4-year follow-up. For the lower leg ABI, compared to participants with neither PAD nor DM, participants with both PAD and DM along with those with only PAD were more likely to have a ≥0.15 decline in their ABI or revascularization during follow-up (HR=3.05, 95% CI: 1.56–5.95 and HR=3.25, 95% CI: 1.73–6.10, respectively). Participants with only DM were also more likely to have either ABI decline ≥0.15 or revascularization during the same period (HR=1.81, 95% CI: 1.06–3.09). Similar results were observed for the higher ABI leg.
Hazard ratio for ankle–brachial index decline ≥0.15 or revascularization from baseline to 4-year follow-up.
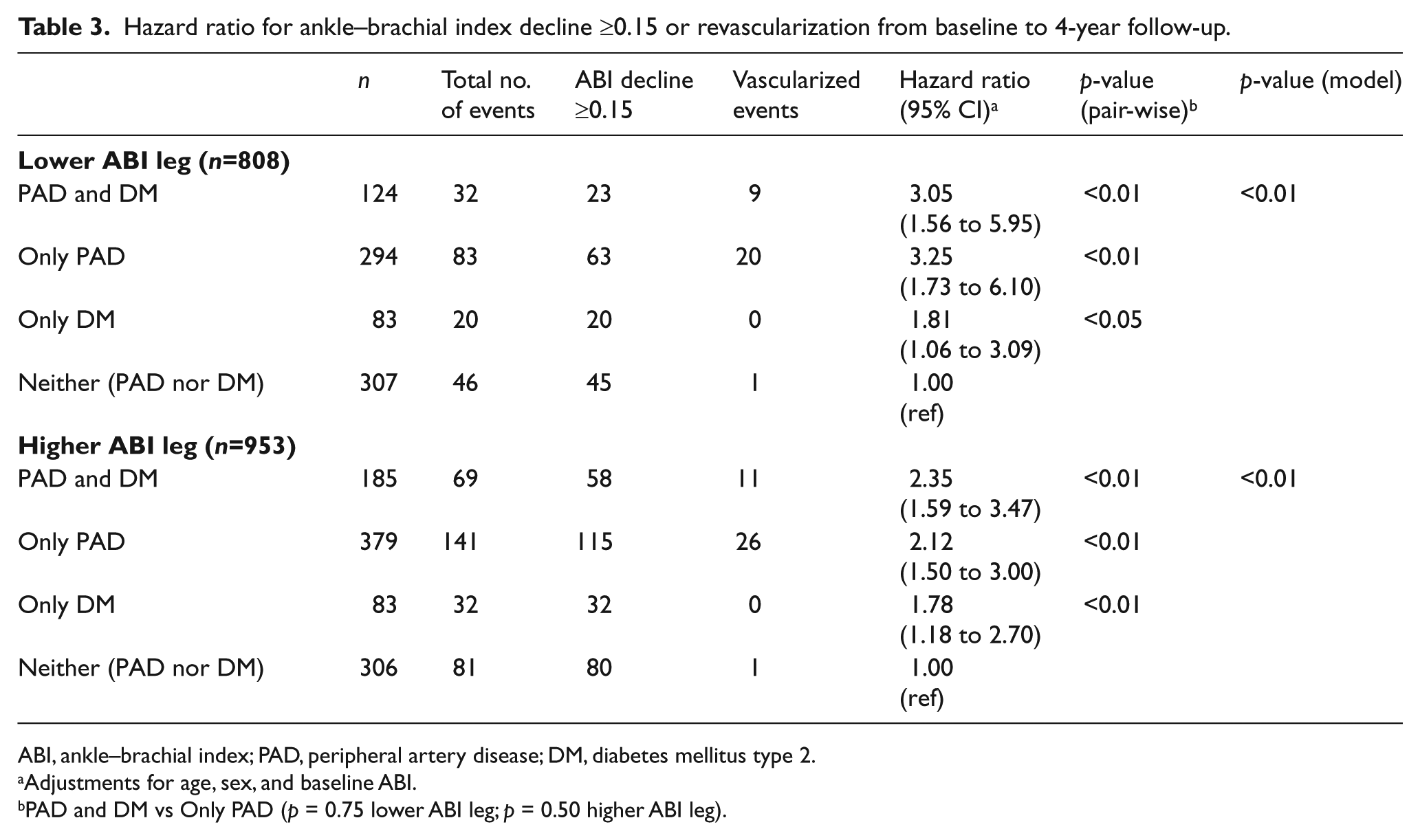
ABI, ankle–brachial index; PAD, peripheral artery disease; DM, diabetes mellitus type 2.
Adjustments for age, sex, and baseline ABI.
PAD and DM vs Only PAD (p = 0.75 lower ABI leg; p = 0.50 higher ABI leg).
Table 4a shows the results of multivariable adjusted analyses relating baseline ABI, age, sex, ethnicity, BMI, cigarette smoking status, pack-years of smoking cigarettes, total cholesterol, HDL cholesterol, CRP, hypertension, DM, use of statin medications, D-dimer, number of cardiovascular diseases, leg symptoms of pain on exertion or at rest, intermittent claudication, and other atypical leg pain with change in the ABI over 4 years. PAD, older age, and higher levels of D-dimer were each independently associated with progression to lower ABI at the 4-year follow-up. DM was not associated with ABI change (p=0.98), and in fact the coefficient was positive, suggesting a slight increase in the ABI in the whole cohort and separately in the PAD and non-PAD groups. The test for DM interaction with baseline ABI (DM*baseline ABI) was not significant (p=0.11). Separate analyses were conducted for participants with and without PAD. In participants with PAD, older age and elevated D-dimer were significantly associated with a lower ABI at the 4-year follow-up (Table 4a). In participants without PAD, more pack-years of smoking and a greater number of cardiovascular diseases were associated with a lower ABI at the 4-year follow-up. In the leg with a higher ABI (Table 4b), after the same adjustments as described above, PAD, lower BMI, higher levels of total cholesterol, use of statin medications, and higher levels of D-dimer were independently associated with lower ABI at the 4-year follow-up, while more pack-years of smoking and a lower HDL cholesterol were borderline non-significant (p = 0.054 and 0.059, respectively). DM was not significantly associated with ABI change over 4 years (p = 0.61), and the test for DM interaction with baseline ABI (DM*baseline ABI) was negative (p = 0.56). When only participants with PAD were evaluated, more pack-years of smoking and elevated D-dimer were independently associated with a lower ABI over 4 years, while older age was borderline non-significant. In non-PAD participants, the leg symptom of intermittent claudication was associated with an increased ABI over 4 years.
Multivariable associations of lower leg ankle–brachial index change over 4 years.
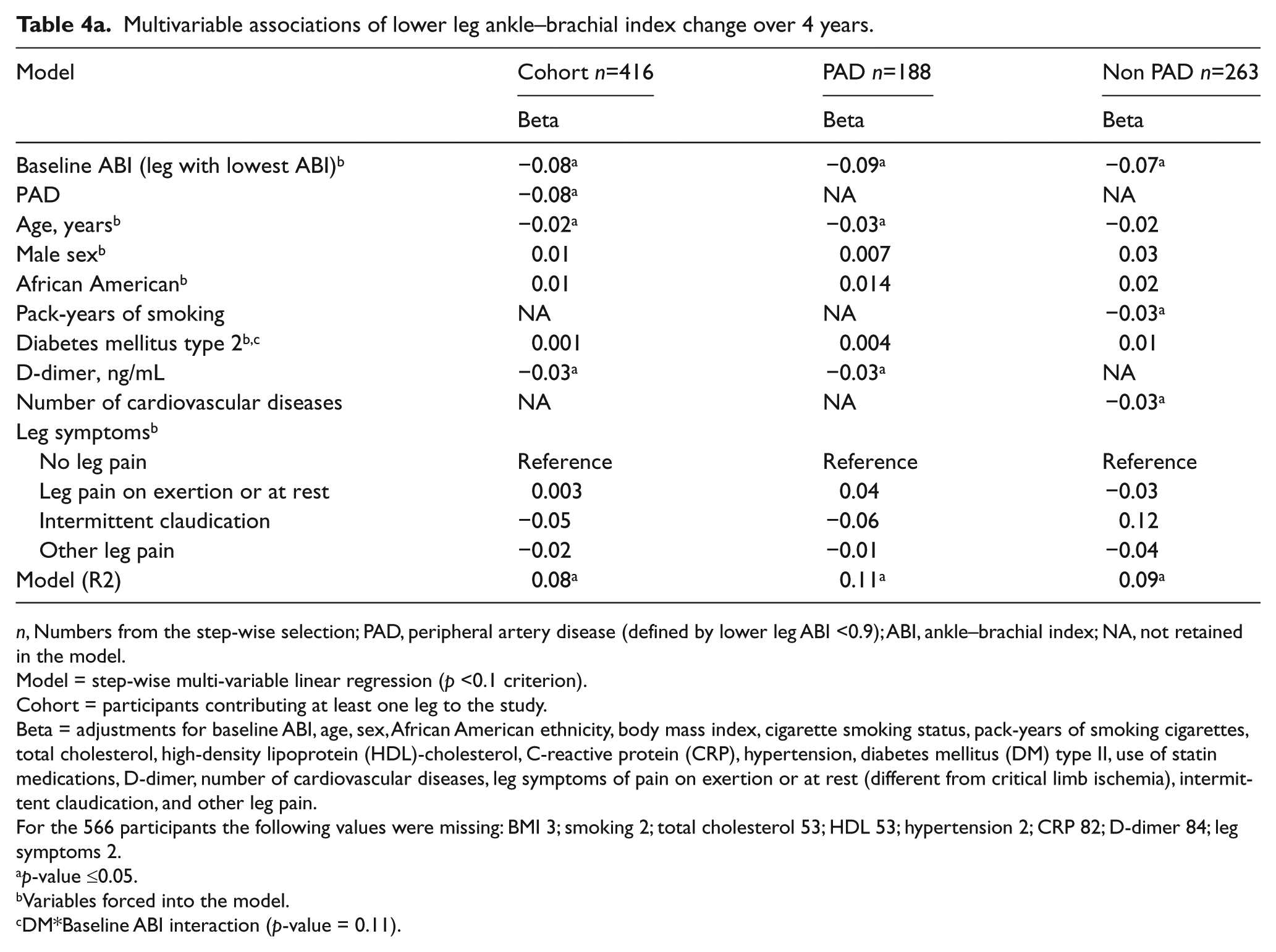
n, Numbers from the step-wise selection; PAD, peripheral artery disease (defined by lower leg ABI <0.9); ABI, ankle–brachial index; NA, not retained in the model.
Model = step-wise multi-variable linear regression (p <0.1 criterion).
Cohort = participants contributing at least one leg to the study.
Beta = adjustments for baseline ABI, age, sex, African American ethnicity, body mass index, cigarette smoking status, pack-years of smoking cigarettes, total cholesterol, high-density lipoprotein (HDL)-cholesterol, C-reactive protein (CRP), hypertension, diabetes mellitus (DM) type II, use of statin medications, D-dimer, number of cardiovascular diseases, leg symptoms of pain on exertion or at rest (different from critical limb ischemia), intermittent claudication, and other leg pain.
For the 566 participants the following values were missing: BMI 3; smoking 2; total cholesterol 53; HDL 53; hypertension 2; CRP 82; D-dimer 84; leg symptoms 2.
p-value ≤0.05.
Variables forced into the model.
DM*Baseline ABI interaction (p-value = 0.11).
Multivariable associations of higher leg ankle–brachial index change over 4 years.
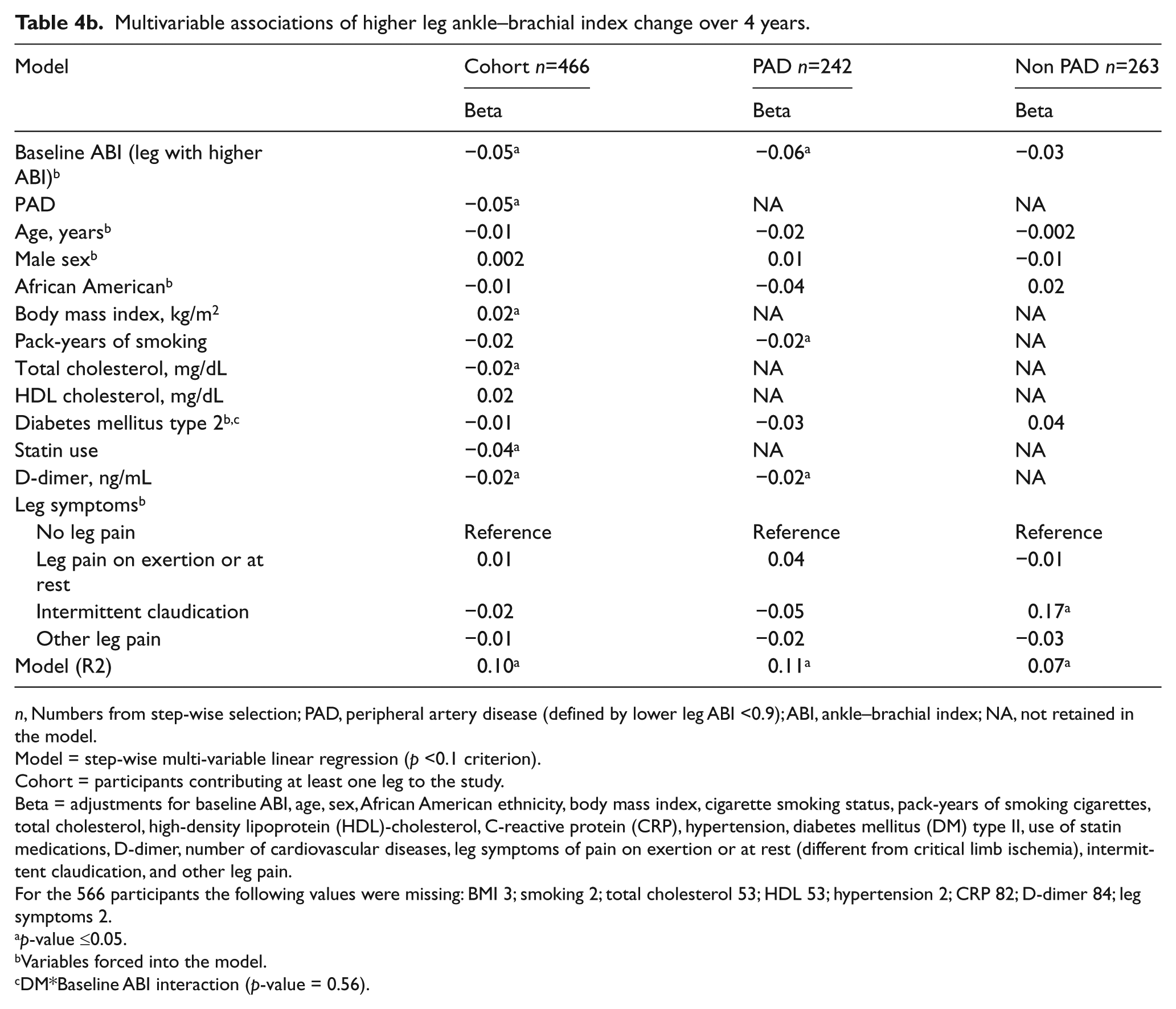
n, Numbers from step-wise selection; PAD, peripheral artery disease (defined by lower leg ABI <0.9); ABI, ankle–brachial index; NA, not retained in the model.
Model = step-wise multi-variable linear regression (p <0.1 criterion).
Cohort = participants contributing at least one leg to the study.
Beta = adjustments for baseline ABI, age, sex, African American ethnicity, body mass index, cigarette smoking status, pack-years of smoking cigarettes, total cholesterol, high-density lipoprotein (HDL)-cholesterol, C-reactive protein (CRP), hypertension, diabetes mellitus (DM) type II, use of statin medications, D-dimer, number of cardiovascular diseases, leg symptoms of pain on exertion or at rest (different from critical limb ischemia), intermittent claudication, and other leg pain.
For the 566 participants the following values were missing: BMI 3; smoking 2; total cholesterol 53; HDL 53; hypertension 2; CRP 82; D-dimer 84; leg symptoms 2.
p-value ≤0.05.
Variables forced into the model.
DM*Baseline ABI interaction (p-value = 0.56).
Sensitivity analysis evaluating the impact of excluding limbs with revascularization during follow-up did not yield significantly different results (not shown). In another sensitivity analysis (also not shown), when considering the higher leg ABI, compared to participants with neither DM nor PAD, those with both DM and PAD had the greatest hazard of ABI increase ≥0.15 (HR=1.92, 95% CI: 0.98 to 3.78). However, this association was borderline non-significant (p = 0.058). Hazards for those with only DM (HR=1.67, 95% CI: 0.82 to 3.39) and only PAD (HR=1.22, 95% CI: 0.66 to 2.27) were not significant.
Discussion
Among individuals diagnosed with PAD, there was a suggestion in our data that participants who also had DM have a smaller ABI decline at the 4-year follow-up. In our cohort, independent factors associated with ABI decline in the leg with the lower ABI were a diagnosis of PAD, older age, and elevated D-dimer. ABI decline at the 4-year follow-up in the leg with the higher ABI was similarly associated with a diagnosis of PAD and elevated D-dimer, but also lower BMI, abnormal lipids, and the use of statin medications. DM was not significantly associated with progression in either the lower or higher leg ABI in multivariable analysis, likely due to the antagonistic effects of DM promoting both PAD and stiff lower-extremity arteries.
DM is a very strong independent risk factor for critical limb ischemia and amputation, as well as incident PAD in population studies.1,21,22 Although a report from a vascular laboratory study indicated that DM did predict ABI decline over an average of 4.6 years of follow-up, the authors excluded follow-up ABI values >1.15 because of likely arterial stiffening. 23 A later report from the same vascular laboratory showed that DM was not related to ABI decline, but was highly and significantly related to a toe–brachial index (TBI) decline. 24 Since the TBI is much less sensitive to arterial stiffening than the ABI, this strongly suggests arterial stiffening in persons with DM during follow-up. Of interest is that in the Cardiovascular Health Study, DM was associated with incident clinical PAD, but not associated with ABI decline over time – again strongly suggesting that DM influences both atherosclerosis and arterial stiffening and that its effects on atherosclerotic PAD may be missed if evaluated using serial ABI measurements. 21 Stiffening may mask the progression of obstructive disease leading to reduced ABI decline, no ABI changes, or slight ABI increases over time. We postulated that due to arterial stiffening, individuals with both PAD and DM might see either an increase in ABI over time or a reduced rate of decline in their ABI over 4 years. We also postulated that this observation would be more prevalent in the higher ABI leg. Though suggestive, our results were not supportive of the latter.
Consistent with this hypothesis, our results demonstrate that the largest decline over 4 years was observed in participants with only PAD. When considering the leg with the lower ABI value (generally used to determine PAD status), these participants had a lower ABI at baseline and a greater decline at 4-year follow-up compared to participants with both PAD and DM, who only had half as much decline.
After adjustments for baseline ABI, older age and abnormal lipids were independently associated with ABI decline in our study. More pack-years of smoking was independently associated with a decline in higher leg ABI for participants with PAD. Smoking cessation is a primary component in the management of PAD because of its strong association with disease incidence and severity. 1
Higher D-dimer levels were associated with ABI decline for both the lower and higher leg ABI. Others have reported the predictive role of D-dimer in the incidence, severity, and progression of PAD.25,26 In fact, in our stratified analysis based on PAD status, an elevated level of D-dimer was the only consistent predictor of ABI decline. Elevated plasma levels of D-dimer may reflect active ongoing atherosclerotic disease progression. 25
This study has some limitations. Participants were recruited from vascular labs in academic medical centers, and results may not be generalizable to other settings. A 4-year follow-up may be too short a time interval to fully characterize ABI change. Limbs with revascularizations prior or during the follow-up period were excluded from the analysis. For individuals with revascularizations in one limb only, the limb without intervention was included in the analysis. Revascularization in one leg may unmask symptoms of intermittent claudication in the other leg. Individuals with revascularizations in both limbs were excluded from the analysis. It is likely that these individuals had increased disease severity, and their exclusion would bias our associations towards the null. Taken together, the overall modest ABI decline in PAD may reflect exclusion of limbs with the greatest burden of lower-extremity atherosclerosis.
Conclusions
In our cohort, cardiovascular disease risk factors of older age and elevated D-dimer were associated with an ABI decline at the 4-year follow-up in persons with PAD. DM was not associated with longitudinal ABI decline. This may reflect its unique opposing effects on ABI by promoting both occlusive atherosclerotic disease and arterial stiffening. This may limit the prognostic value of the ABI in diabetic patients.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflict of interest.
Funding
Funding was received from T32 HL079891, NIH-NHLBI Training Grant ‘UCSD Integrated Cardiovascular Epidemiology Fellowship’.