
Abstract
Introduction
Telehealth services using videoconference and telephone modalities have been increasing exponentially in primary care since the coronavirus pandemic. The challenge now is ensuring that these services remain sustainable. This review investigates the cost-effectiveness of videoconference and telephone consultations in primary care settings, by summarizing the available published evidence.
Methods
A systematic search of PubMed, Embase, Scopus, and CINAHL databases was used to identify articles published from January 2000 to July 2020, using keyword synonyms for telehealth, primary care, and economic evaluation. Databases were searched, and title, abstract, and full-text reviews were conducted. Article reporting quality was assessed using the Consolidated Health Economic Evaluation Reporting Standards checklist.
Results
Twenty articles were selected for inclusion, with 12 describing telephone triage services, seven describing telehealth substitution services, and one describing another telehealth service in primary care. These services were delivered by nurses, doctors, and allied health clinicians. Of the 20 included studies, 11 used cost analyses, five used cost-minimization analyses, and four used one or more methods, including either a cost–consequence analysis, a cost–utility analysis, or a cost-effectiveness analysis.
Conclusions
Telephone and videoconference consultations in primary care were cost-effective to the health system when deemed clinically appropriate, clinician when time was used efficiently, and when overall demand on health services was reduced. The societal benefits of telehealth consultations should be considered an important part of telehealth planning and should influence funding reform decisions for telehealth services in primary care.
Introduction
Telehealth is the delivery of a healthcare service from a distance. Common telehealth modalities include videoconference, store-and-forward, and remote monitoring. The benefits of telehealth are well reported and include improved access to care, reduced need for travel, and better continuity of care.1–3 Despite these benefits, the routine uptake of telehealth by health services prior to the coronavirus (COVID-19) pandemic was slow and fragmented. 4 Telehealth use has increased globally since COVID-19 because it obviates the need for direct physical contact.5–9 Payers, including governments and health insurers, responded to this need by funding telehealth (i.e. videoconference and telephone consultations) in a similar way to in-person (traditional) consultations.1,10–12 In primary care, videoconference and telephone consultations have been reimbursed to reduce the risk of COVID-19 transmission.1,13 Primary care is generally an individual's first encounter with the health system and includes general practitioner (GP) or family physician services, nurse-led clinics, or other multidisciplinary services. 14 Many of these clinicians are now routinely using videoconference and telephone modalities to provide patient care.
Videoconference and telephone consultations in primary care settings have grown exponentially during the pandemic; the challenge now is ensuring the sustainability of telehealth as a business-as-usual service post-pandemic. 9 A viable telehealth service requires funding to support infrastructure and personnel costs. To assist decision-makers with telehealth funding choices, evaluations summarizing the economic evidence for videoconference and telephone consultations are required. Economic evaluations should consider both the costs and consequences (or benefits) of a service to determine if it is cost-effective. 15 Consequences are quantified by measuring the effectiveness of a service, either through a clinical outcome or utility value, such as the quality-adjusted life year (QALY).15,16 Previous research has investigated the safety and effectiveness of telehealth in primary care17–20; however, there is limited literature on the economic evaluation of telehealth of any kind in primary care. This review aims to investigate the cost-effectiveness of videoconference and telephone consultations in primary care settings, by summarizing the available published evidence.
Methods
This systematic review was conducted in accordance with the published protocol in the International Prospective Register of Systematic Reviews (ID CRD42020205098). 21
Search strategy and article screening
The Boolean searches of PubMed, EMBASE, Scopus, and CINAHL databases were conducted using keyword synonyms for telehealth, primary care, and economic evaluation (Supplementary File S1). COVID-19 was included as a search term in case telehealth was investigated in this context. The comprehensiveness of results was guaranteed by hand-searching reference lists of returned articles. Duplicates were removed, titles and abstracts were screened for eligibility, and articles were read in full text by two reviewers (KD and CM). Any conflicts were revised by a third reviewer (CS) to reach consensus for the final included articles.
Eligibility criteria
The search strategy included articles published in English from January 2000 to July 2020.
Included studies reported on:
telehealth services integrated in primary care settings (services must be connected with local clinics or providers); videoconference consultations, telephone triage, and telephone consultations; comparisons between telehealth and usual care (i.e. usually an in-person consultation); economic outcomes of telehealth. alternative telehealth modalities (remote monitoring or store-and-forward); telehealth in secondary, tertiary, or quaternary care settings; telehealth consultations involving a specialist; telehealth not integrated into primary care (e.g. national government help line).
Excluded studies reported on:
Data extraction and data synthesis
Data were extracted from the included studies by one reviewer (KD) and cross-checked by another reviewer (CS). Extracted data included study characteristics, service model descriptions, type of economic evaluations, and key economic findings. Telehealth service models were classified as: “triage,” where telehealth was used for remote patient assessment; “substitution,” where a telehealth consultation directly substituted an in-person consultation; and “other service,” which did not fit into these categories. Triage services prioritized care or determined need for treatment and were staffed by clinical personnel who could provide self-management advice to patients if an in-person consultation was not required. Economic evaluations were characterized as: a cost analysis (CA), a cost-minimization analysis (CMA), a cost-effectiveness analysis (CEA), a cost–utility analysis (CUA) or a cost–consequence analysis (CCA). The further descriptions of these analysis types are provided (Table 1). The economic findings were synthesized narratively and categorized by service model description. Meta-analysis was not completed due to the inappropriateness of combining economic outcomes between different patient populations, countries, and health systems. All costs and price years were adjusted to 2020 US$ using price deflators for GDP and purchasing price parities for GDP. 22
Description of economic analysis types.
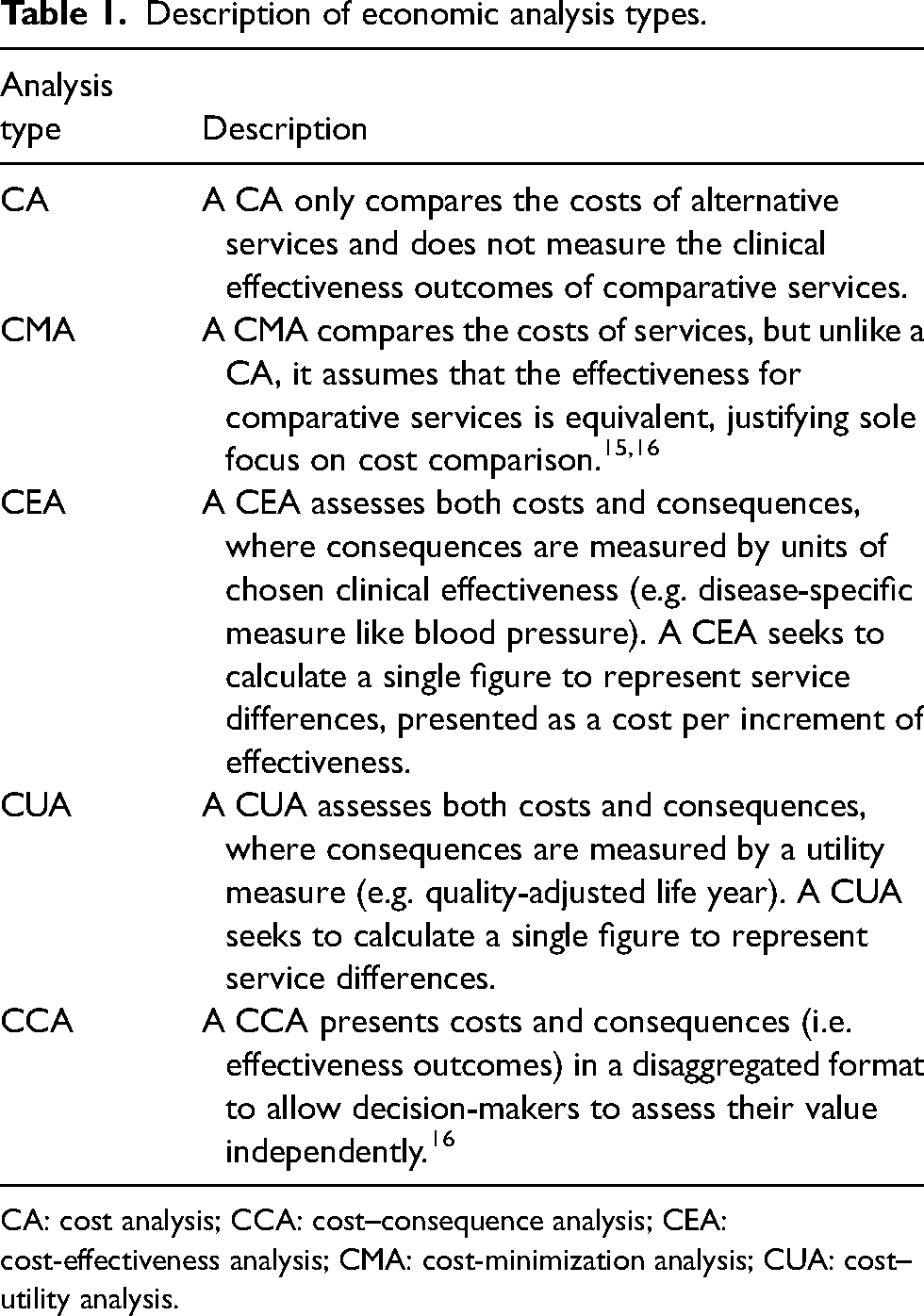
CA: cost analysis; CCA: cost–consequence analysis; CEA: cost-effectiveness analysis; CMA: cost-minimization analysis; CUA: cost–utility analysis.
Quality assessment
The Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist was used to assess the quality of each article. 23 Each article was assigned a value out of 24 points, with higher scores indicating more complete reporting. 23 CHEERS items include economic principles such as perspective, time horizon, discounting, effectiveness measurement, assumptions, and incremental cost and outcomes. 23 Final quality scores were reported as percentages; the denominator was adjusted accordingly if any items were irrelevant to an analysis. All articles were scored by one reviewer (KD), and a random sample (20%) of the articles was cross-checked by another reviewer (CS) for quality assessment.
Results
Study selection
Twenty articles were included in this review. The screening and selection process is summarized in Figure 1.24–43
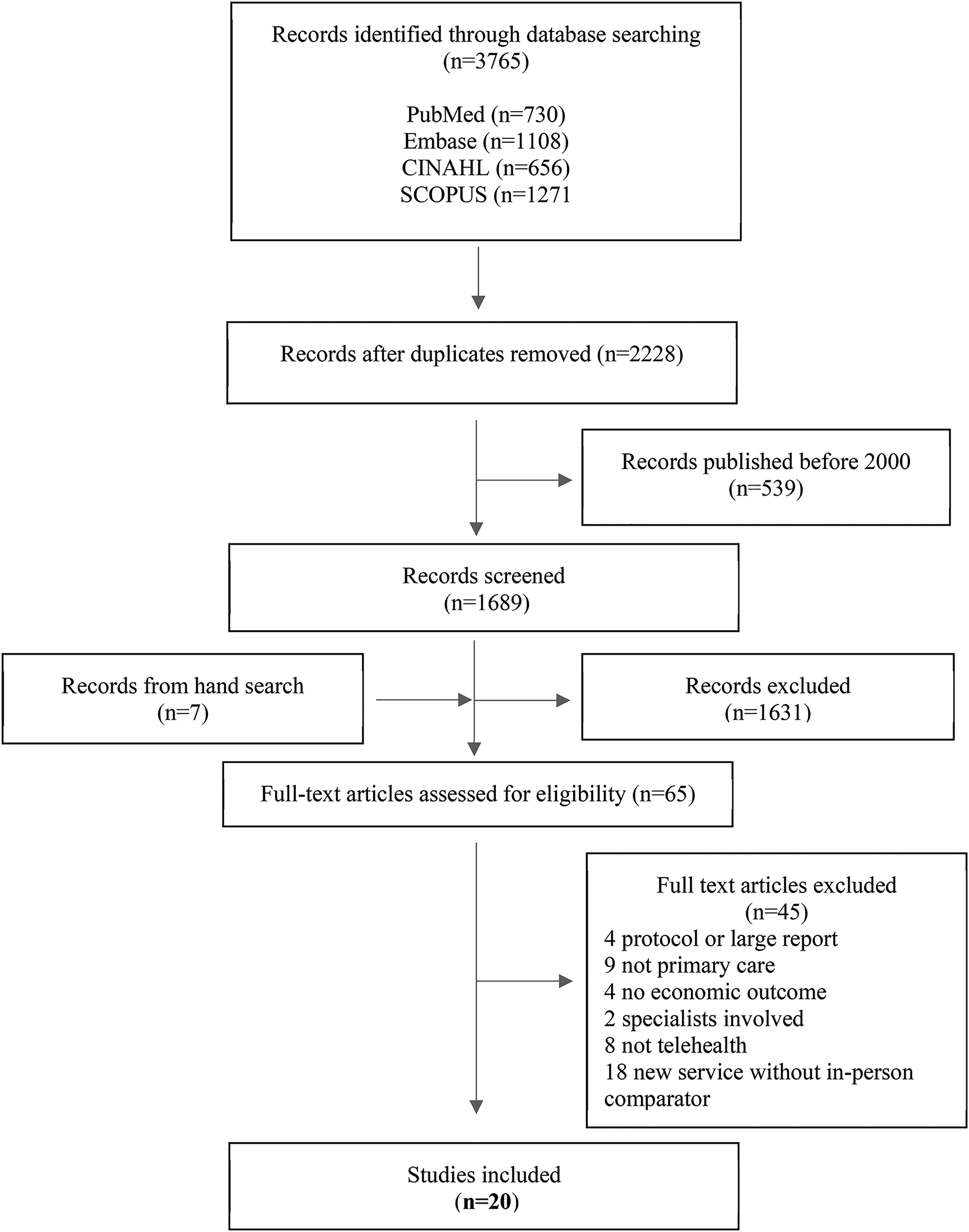
Article identification, screening, and inclusion process. Modeled according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRIMSA) protocol.
Study characteristics
Telehealth was provided to primary care patients with musculoskeletal problems,26,34 asthma,25,35,39 acute respiratory illnesses, 33 depression, 38 diabetes, 41 and other clinical conditions. Studies reflected telehealth in five countries, with most originating in the United Kingdom (50%) (Table 2). Five studies (25%) conducted a CMA, 11 (55%) conducted a CA, and four (20%) assessed costs and effectiveness by conducting one or more methods of a CCA (n = 2), a CUA (n = 2), and a CEA (n = 2). Telehealth services were delivered by nurses,24,25,27,28,30–32,35,37,39,42,43 doctors,24,29,33,36 physiotherapists,26,34 psychologists, 38 and counselors. 40 Clinicians were often reported as clinically experienced,25–28,30,34,35,37,43 and some received telehealth training.24,26,27,39,40
Study characteristics.
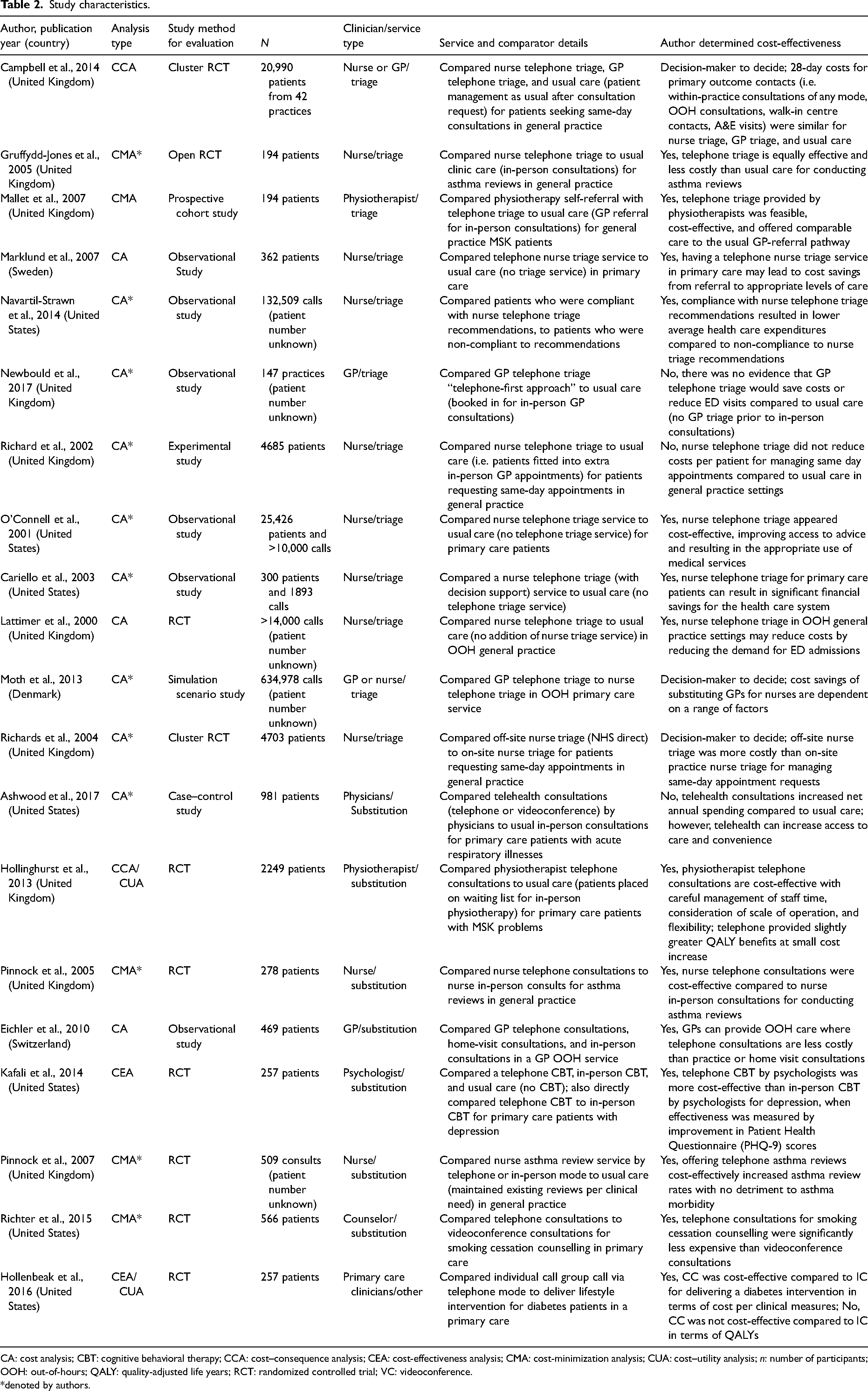
CA: cost analysis; CBT: cognitive behavioral therapy; CCA: cost–consequence analysis; CEA: cost-effectiveness analysis; CMA: cost-minimization analysis; CUA: cost–utility analysis; n: number of participants; OOH: out-of-hours; QALY: quality-adjusted life years; RCT: randomized controlled trial; VC: videoconference.
*denoted by authors.
Studies described triage (n = 12, 60%), substitution (n = 7, 35%), and other telehealth services (n = 1, 5%). Triage services all used telephone to determine prioritized care or provide clinical advice to patients. One triage service compared GP to nurse telephone triage, 42 and one compared off-site nurse (from external agency) to on-site (in-clinic) nurse telephone triage. 43 Decision support software was frequently used to support nurse triage recommendations.24,27,32,37,43 Most substitution services used telephone to substitute in-person care, with only two that used videoconference.33,40 The one “other” telehealth service compared individual telephone calls to group calls. 41 The reported benefits of telehealth were reduced waiting times, reduced travel, increased convenience, and accessible care.24,26,33–35,38
Study quality reporting assessment
There was a wide spread of reporting quality when studies were assessed using the CHEERS checklist. Articles scored an average of 66% (SD = 15%, range 43–91%) on the checklist (Supplementary File S2). Low quality reporting was mostly due to CA studies, with nine scoring <70% and two scoring 70–79%. Lower scores were due to the poor reporting of effectiveness items (not applicable to CAs), perspective, discounting, uncertainty, and heterogeneity. No studies scored 100%; however, four scored between 80% and 89%, and one scored between 90% and 99%.
Economic findings
Telehealth triage services (n = 12)
Effective telehealth triage should direct patients to an appropriate service for their clinical condition or enable them to self-manage their condition without further care. Telehealth triage in primary care may provide economic benefits due to efficiencies gained in service use. Most studies investigated the effect of telephone triage on overall service use, such as emergency department (ED) admissions, which usually resulted in decreased costs to the health system.24,27–32,37 Four studies that examined nurse telephone triage reported that cost savings were due to the redirection of patients intending to use a higher level of care (e.g. ED) to a less costly and lower level of care (e.g. GP). These four studies used stated preference methods to estimate cost savings by comparing the patients’ intended action (as stated by them) to the actual clinician recommendation.27,28,31,32 Another study investigated nurse telephone triage, reporting net yearly savings from reduced ED admissions and GP travel. 37 Conversely, two studies found opposite results, where GP triage did not reduce ED admissions, 29 and cost savings from shorter triage consultations were offset by costs in nursing staff, follow-up, and ED care. 30
Telephone triage enabled the prioritization of workload, diverting inappropriate same-day appointments to future routine appointments. 30 In a CCA study, no cost differences between GP triage, nurse triage, and in-person care were reported for primary care contacts within 28 days 24 ; instead, there was a redistribution of workload from in-person to triage care. 24 Two CMA studies found that telephone triage was cost-effective for asthma and physiotherapy patients, on the assumption that clinical outcomes were equivalent regardless of modality.25,26 This was because of reduced consultation time and reduced missed appointments.25,26 Two studies investigated different aspects of telephone triage, with one reporting that off-site nurses increased costs compared to on-site nurses because of longer consultations, fewer managed calls in a shift, and increased referral to doctors. 43 The other reported that the nurse substitution of GPs may increase costs because of subsequent GP care. 42 Overall, three studies reported findings from a health system perspective,24,25,37 while the remaining studies did not report a perspective (Table 3).
Economic analysis of selected studies.
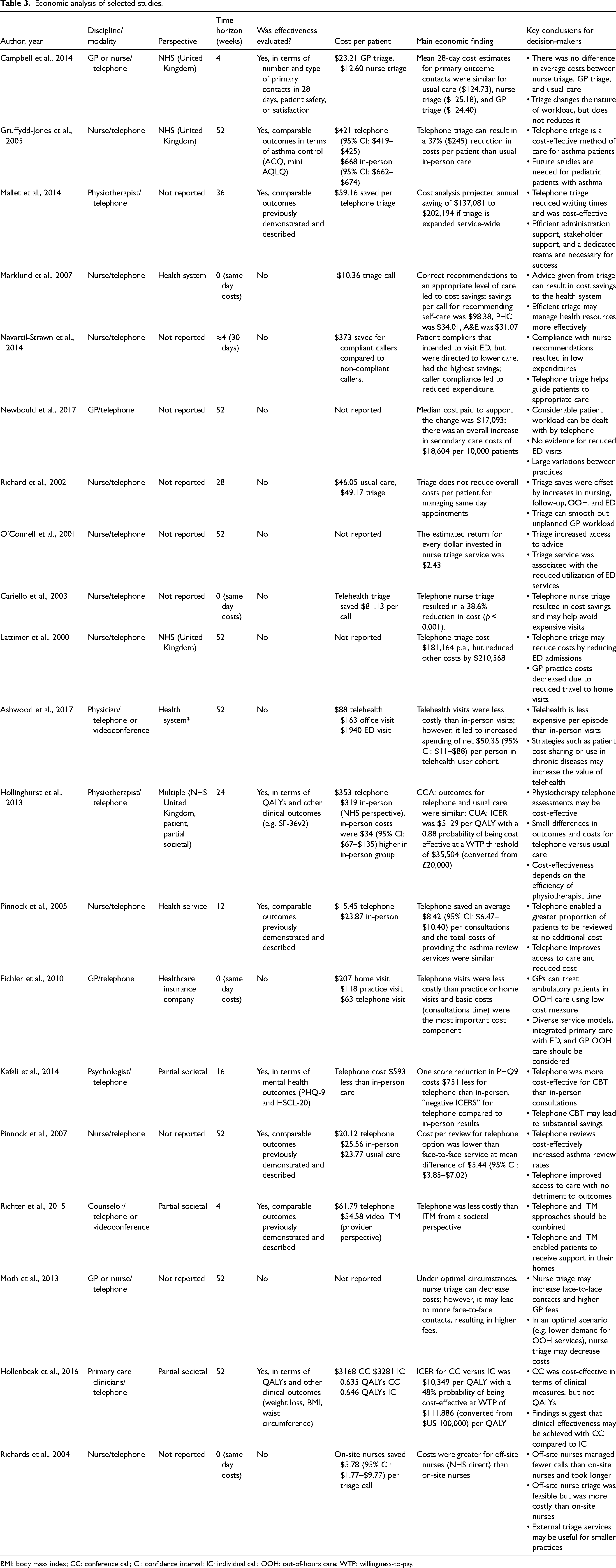
BMI: body mass index; CC: conference call; CI: confidence interval; IC: individual call; OOH: out-of-hours care; WTP: willingness-to-pay.
Telehealth substitution services (n = 7)
If telehealth is used to substitute in-person care, it should aim to produce comparable clinical outcomes or achieve additional benefits (e.g. reduced travel). Telehealth substitution may provide economic benefits if it is used in appropriate clinical scenarios and does not increase overall service use. A CCA/CUA study reported that physiotherapist telephone consultations cost slightly more than in-person consultations with slightly greater QALY benefits, 34 yielding an incremental cost-effectiveness ratio of $5129 per QALY from the health service perspective. 34 In a sensitivity analysis, it was demonstrated that higher savings would be achieved if physiotherapists spent more time on billable telehealth consultations than administrative tasks. 34 A CMA study reported that telephone asthma consultations were cost-effective compared with in-person consultations, from the health service perspective, because of reduced consultation times. 35 Similarly, another CMA study reported that telephone asthma consultations were cost-effective compared with in-person consultations because they were shorter and required less nurse time (no perspective reported). 39 Both CMA studies assumed that asthma-related outcomes were equivalent regardless of modality.
A study comparing home-visit, in-person, and telephone consultations by GPs reported that telephone reduced costs to the service provider. 36 Another study compared telephone cognitive behavioral therapy (CBT) to in-person CBT. Telephone was cost-effective from a partial societal perspective, because of reduced mental health service use, patient travel, and patient waiting time. 38 Telephone was also cost-effective compared with videoconference for a smoking cessation intervention from a partial societal perspective. 40 Higher costs for videoconference were largely due to clinic space costs. 40 One study reported that telephone and videoconference consultations for patients with acute respiratory illnesses increased overall service costs. 33 This was because of telehealth convenience, which resulted in additional health service use. 33 Overall, studies investigating substitution services used three CMAs,35,39,40 two CAs,33,36 one CEA, 38 and one CCA/CUA, 34 with only one study (CA) 33 reporting that telehealth was not cost-effective compared with in-person care (Table 3).
Other telehealth services (n = 1)
Other aspects of telehealth delivery are important to consider for potential avenues for cost savings. One CEA/CUA study compared telephone group calls to individual calls for a diabetes intervention, reporting that a group call was cost-effective from a partial societal perspective (patient gains are factored in) when clinical effectiveness measures were used (CEA). 41 However, when QALYs were used to measure effectiveness (CUA), a group call was no longer cost-effective because of staff and technology costs. 41
Discussion
The cost-effectiveness of telehealth services in primary care settings was found to be context dependent, contingent on changes in overall service use, and dependent on secondary care resource use. Implementation and operational costs (i.e. staff or consultation time) played an important role in determining telehealth cost-effectiveness. Of the 20 included studies, 13 reported telehealth as cost-effective, three reported telehealth as not cost-effective, one reported cost-effectiveness as decided by the decision-maker (CCA), and three reported cost-effectiveness as dependent on how telehealth was delivered (i.e. group vs individual call, nurse- vs GP-triage, and on- vs off-site nurses). These findings should be considered in light of study context, analysis type, and service model delivered. Of the 13 studies that reported cost-effective telehealth services, seven described telephone triage and six described telehealth substitution; six studies reported cost-effectiveness from a health system perspective, two from a partial societal perspective, and five without a perspective.
Integrating telehealth into primary care can be cost-effective for the health system when it reduces overall service use and secondary care resource use (e.g. ED admissions), especially when the same provider is bearing the cost for primary and secondary care services. Telephone triage saves costs if patients are successfully redirected from high-cost to low-cost acute care services, but not when the end result is an increase in service use or high-cost service access following triage. Telephone triage redistributed workload from in-person to telehealth modalities 24 and transferred appointment costs from inappropriate same-day appointments to routine appointments. 30 Therefore, telehealth can help prioritize care and change the nature of clinician workload, rather than affecting costs. Other studies have found that telehealth in primary care reduces secondary care resource use,44–46 and although economic findings were not investigated, an economic impact can be inferred.
The efficient use of clinician time influenced the cost-effectiveness of telehealth in primary care. Telehealth resulted in shorter consultation times,25,30,35,36,39 which can reduce the marginal cost per consultation for the provider if fixed costs are assumed for the service. 47 However, longer consultations can improve patient care and satisfaction. 48 This emphasizes the importance of assessing costs and effectiveness (e.g. CEA) to ensure that economic benefits are achieved without compromising patient care. Provider costs for telehealth are not just reflected in consultation time, but in time spent on set-up and planning, and addressing technical issues. Increased savings were estimated if clinicians spent more time on telehealth consultations than administration tasks 34 or travel. 37 Therefore, telehealth could improve clinician productivity if this time is converted to clinical activities instead,47,49 emphasizing the need for streamlined processes and reliable software.
The cost-effectiveness of telehealth likely depends on the clinical condition of primary care patients. Patients with acute respiratory illnesses found it more convenient to seek advice through telehealth, 33 which resulted in increased health system costs because of increased service use. 33 Therefore, telehealth may not be cost-effective for minor ailments, which can be self-managed. Telehealth was reported as cost-effective for the management of asthma,35,39 musculoskeletal problems,26,34 depression, 38 diabetes, 41 and smoking cessation. 40 Chronic diseases, such as diabetes or asthma, have an immense economic burden on the health system because of costs for disease management and lost productivity from illness and death. Thus, primary care prevention and management are key in reducing long-term costs. 50 Telehealth can facilitate the ongoing care of chronic diseases that are often undertreated 33 and require regular monitoring.51,52 Economic benefits from investment into these services may not be realized immediately as savings are likely gained in the future (due to reduced complications or improved management).
Missed appointments represent a cost burden on the health system by increasing the marginal cost of consultations provided by that service.47,53 Telehealth can reduce failure to attend, 26 thereby decreasing unnecessary costs and ensuring that patients receive timely care, an aspect particularly important for primary care patients seeking advice for the first time. Implementation costs (e.g. infrastructure) can influence telehealth cost-effectiveness in the short term.40,54 Other research has reported that cost savings from telehealth may not be recouped because of implementation or operational costs, 55 although this can be outweighed if service activity increases. 55 This demonstrates that telehealth may benefit from economies of scale, where increasing the scale of production decreases the marginal cost per consultation.34,56–58 Asides from economic benefits, other more tangible telehealth benefits need to be acknowledged. Telehealth can reduce patient waiting times, increase convenience, and deliver more timely care. Considering this, partial societal perspectives often provide a broader cost estimation and more holistic approach to the benefits of telehealth.
Limitations
The conclusions are limited to the findings reported by included studies, where results are dependent on analysis type and reporting quality. Many studies failed to articulate an analysis perspective, making their assertions difficult to interpret. Sensitivity analysis, which measures the effect of fluctuating cost variations, was often not conducted even though this can help identify opportunities for economic improvement. 59 CA studies did not measure effectiveness, so the clinical impact of these services cannot be determined; some CAs used stated preference methods where there is no guarantee that patients will do what they stated. Furthermore, results were grouped by service model description, and not analysis type, because a majority of studies were CAs (i.e. limited CEAs and CUAs). These findings may be less applicable to videoconference, as only two studies investigated this modality. Earlier studies may not accurately reflect present situation, as telehealth costs may be reducing over time from more affordable ICT systems.
Implications for decision-makers
When the costs and effectiveness of telehealth are comparable to in-person care, it is an excellent contender for implementation given the societal benefits. Telehealth is not intended to replace all in-person care, and it is important to consider telehealth in the context of clinical requirements. Telehealth can save costs for the health system if overall service use is decreased, or in-person care is reduced. This knowledge is useful for decision-makers considering provider telehealth reimbursement. 12 However, telehealth implementation should be motivated by benefits outside cost savings, as it enables the delivery of multidisciplinary services and the expansion of primary care services (e.g. nurse triage). 60 The cost-effectiveness and reimbursement of telephone and videoconference consultations are likely to be different. Therefore, it is imperative that the cost-effectiveness of telephone and videoconference consultations is assessed separately to inform future telehealth funding reforms. Owing to the rapid uptake of telehealth since COVID-19,6,9 investigating patient and clinician experiences may further help develop strategies for telehealth sustainability.
Conclusions
Videoconference and telephone consultations in primary care were cost-effective from a health system perspective when used in appropriate clinical situations, when clinician time was used efficiently, and when overall service use was reduced. The benefits of telehealth from a primary care perspective should consider the less tangible benefits, such as timely and accessible patient care, the promotion of multidisciplinary services, and opportunities to expand the capacity of the primary care sector. All these potential benefits are important for decision-makers considering the implementation and reimbursement of an integrated telehealth service.
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X211043380 - Supplemental material for Economic evaluations of videoconference and telephone consultations in primary care: A systematic review
Supplemental material, sj-docx-1-jtt-10.1177_1357633X211043380 for Economic evaluations of videoconference and telephone consultations in primary care: A systematic review by Keshia R De Guzman, Centaine L Snoswell, Liam J Caffery, and Anthony C Smith in Journal of Telemedicine and Telecare
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Australian Government Research Training Program Scholarship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.