
Abstract
The COVID-19 crisis rapidly introduced telemedicine as the predominate modality to deliver healthcare however this change has not received attention in primary care settings and the health-related impacts are unknown. The study’s objective was to explore the effects of physician-led synchronous telemedicine compared to face-to-face care delivered in the primary care setting on healthcare system use and attributes of primary care as reported in recent studies. We performed a comprehensive literature search in five databases (MEDLINE, Embase, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, PsycInfo) and critical appraisal using the Joanna Briggs Institute tools. Of 6,247 studies identified, 157 studies underwent full text review, and 19 studies were included. Most studies were conducted in the U.S. (78.9%) and used video and telephone telemedicine (57.9%). An outcome-based qualitative description and narrative synthesis showed similar or fewer emergency department visits, hospital visits, and prescribing, and fewer diagnostic tests and imaging for telemedicine visits compared to face-to-face care. Our systematic review fills a gap in the literature on telemedicine in primary care settings however our results need to be interpreted cautiously given studies’ susceptibility to selection bias, confounding, and limited applicability to other health systems and time periods.
Introduction
Telemedicine is the delivery of remote healthcare by providers to patients using digital tools and is a subcomponent of telehealth. The World Health Organization defines telemedicine as “the delivery of healthcare services where distance is a critical factor, by all healthcare professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries all in the interests of advancing the health of individuals and their communities” (World Health Organization, 2022, November 9). The global widespread implementation of telemedicine coincided with the emergence of the COVID-19 crisis which varied depending on the context of local public health measures, reimbursement models and health systems (Bhaskar, 2020). Despite the disruption in the delivery of care due to the COVID-19 pandemic, a more hybrid vision of healthcare was cultivated with the emergence of telemedicine having the advantages of more timely access to providers, at-home patient monitoring for chronic conditions, reduced patient travel and wait times, and increased convenience for patients to seek medical care earlier and potentially circumvent delays in diagnosis and treatment (Petrazzuoli, 2021; Temesgen, 2020).
Primary care is the context of most health service delivery around the world. Strong primary care systems benefit population health and promote a more equitable distribution of health by embodying the service delivery attributes of first contact care, person-focused care, care over time, comprehensiveness, and coordination (Mangin, 2016; Starfield, 2005). The recent shift in the delivery of primary care from face-to-face care to telemedicine was substantial due to the emergence of the COVID-19 pandemic. To illustrate, comparing the pre-pandemic period to the pandemic period, telemedicine in primary care comprised 1.2% versus 71.1% of all visits (Glazier, 2021). Given the widespread adoption of telemedicine provision in primary care and its ongoing integration into current health practices, it is important that changes embedded in the delivery of primary care be studied to examine the impact on patients and determine whether care continues to exemplify the service delivery attributes that have been shown to benefit population health. The reported drawbacks of a more digital model of care include barriers to accessing care due to social and economic contexts, reduced quality of care, and exacerbation of existing health inequalities (Abrams, 2020; Mishra, 2023; Petrazzuoli, 2021; Rashid, 2020).
There has been a growing body of literature examining the clinical effectiveness of digital tools used in the remote delivery of healthcare however an evidence gap remains in the context of telemedicine and primary care. A recent systematic review of 38 meta-analyses concluded that telehealth is equivalent to or more clinically effective than usual care, however the findings were not applicable to primary care since the review focused on specialized areas of medicine (e.g., endocrinology, psychology, neurology, pulmonary), biomedical-based outcome measures and assessment tools, and included heterogeneous telehealth interventions (Snoswell, 2021a). Another recent systematic review by Snoswell et al. (2021a) identified 24 meta-analyses and concluded that telehealth did not increase mortality rates, however the review was narrowly focused on a single endpoint in advanced diseases (e.g., chronic heart failure, stroke, chronic obstructive disease exacerbations) and findings were largely driven by earlier disease detection using remote monitoring (Snoswell, 2021b). Despite informing the evidence base on digital tools used in the remote delivery of healthcare, previous systematic reviews lack applicability to the healthcare experiences of primary care physicians. Specifically, delivering care to patients in real-time (e.g., synchronous care), addressing the holistic nature of patient care, and focusing on generalist areas of medicine. Additionally, previous systematic reviews have not examined key person-centred outcomes relevant to the primary care setting such as quality of life, patient satisfaction, and patient-provider communication (Mangin, 2016). Notably, the review of reviews conducted by Ekeland (2010) summarized findings from 80 systematic reviews (Ekeland, 2010). The authors demonstrated that the evidence base for telemedicine is heterogeneous, with an equal number of studies showing its effectiveness as well as mixed results. This review, which assembled a vast amount of evidence on telemedicine was conducted at a time prior to the surge of telemedicine globally, did not provide an outcome-based synthesis to facilitate uptake of findings, and was too broad in the telemedicine interventions considered to be relevant to the primary care setting. Consequently, more focused reviews are needed to help uncover the impacts of telemedicine on patients in the primary care setting.
To fill this gap in the literature, we undertook a systematic review to identify and synthesize relevant studies on physician-led synchronous telemedicine compared to face-to-face care in primary care settings. The objective of this systematic review was to explore the effects of telemedicine delivered in the primary care setting on healthcare system use and attributes of primary care as reported in recent studies. The impetus of this work was to efficiently assemble the evidence on the outcomes of telemedicine in primary care at a time of easing restrictions and lessening of community lockdowns, and the potential for a future hybrid model of care. The findings of this review would help to inform the impacts of the pandemic on patients and the health system, which at the time were unknown.
Methods
We followed the items outlined in the PRISMA Reporting Guideline for Systematic Reviews (Page, 2021) and best practices for the conduct of systematic reviews of interventions (The Cochrane Collaboration, 2023). The systematic review protocol was registered on the PROSPERO website (CRD4202232505) (National Institute for Health and Care Research, 2023).
Search Strategy
Relevant published studies were identified by performing a literature search in five databases including MEDLINE, Embase, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, and PsycInfo covering the search years of Jan 1, 2019, to June 2, 2023. The publication date range was selected to capture recent studies with relevant use of telemedicine in the primary care setting (Glazier, 2021). The search terms were developed in consultation with McMaster Library Services (Supplemental Materials, Appendix 1). Studies were imported into Covidence and duplicate records were automatically removed.
Study Selection and Inclusion Criteria
Study selection followed a multi-stage process. In the first stage, potential studies for inclusion were screened based on title and abstract by one reviewer (JS or LY) using Covidence after a sample of 30 studies were reviewed to ensure consistency among reviewers with an agreement score of >80% (Shea, 2017; The Cochrane Collaboration, 2023). In the second stage, all full-text articles were assessed by two independent reviewers (JS and LY) and reasons for exclusion were documented in Covidence. Disagreements in the selection of studies for inclusion were resolved by discussion among reviewers and when needed, studies were reviewed by a third reviewer (KB) for any persistent disagreements. The bibliographies of relevant grey literature, review articles, and included articles were examined for additional potentially relevant papers. Eligible published studies were quantitative studies of any design, conducted in primary care/generalist areas of medicine, focused on physician-led synchronous telemedicine by videoconferencing and/or telephone, and reported on at least one outcome of interest. Outcomes were conceptualized under the broad umbrella of healthcare system use which included the components of clinical care commonly encountered in the primary care setting of symptom and disease management, diagnostic tests and imaging, prescribing practices, and healthcare use measured by the number of hospitalizations, emergency department visits, and outpatient follow up visits. All results compatible with each outcome domain were abstracted. The attributes of primary care were also considered as outcome domains. Studies were excluded if they fell outside of primary care (e.g., stroke, nephrology, neurology, oncology, surgical and other specialties), were based in inpatient/congregate care settings or veterans care, were based on commercial direct-to-consumer telemedicine, were not published in English, did not have full-texts available, and were not of a suitable publication type (e.g., conference abstracts, protocols).
Data Collection and Synthesis
Data from full-text articles meeting the inclusion criteria were collected by one reviewer and data audited by a second reviewer. We abstracted the following study characteristics: author, year of publication, country, study design, patient population, number of patients and/or visits (total and by care modality), and type of telemedicine (videoconferencing and/or phone). Telemedicine was often reported as ‘telehealth’ or ‘virtual care’ among included studies, therefore data collected in tables and in the supplemental materials reflect the terminology used in the original study. For studies with relevant outcome data, we abstracted quantitative data including means or medians, standard deviations, percentages, adjusted estimates and their corresponding confidence intervals, and p-values comparing telemedicine to face-to-face care. A meta-analysis was not performed due to the heterogeneity of included studies. We report a qualitative description and narrative synthesis of the results by outcome for included studies.
Risk of Bias Assessment
Individual studies were assessed for risk of bias using the Joanna Briggs Institute (JBI) quantitative critical appraisal tools (Barker, 2023). Two reviewers (JS and LY) independently performed the risk of bias assessment and any disagreements were resolved by discussion.
Results
Overview of Included Studies
A total of 6,247 citations were identified by the literature search, of which a total of 157 studies underwent full-text review. An additional relevant citation from the grey literature was identified (Canadian Agency for Drugs and Technologies in Health, 2022), which contributed one study, and a previous relevant systematic review was identified (Bakhit, 2021), which contributed one study. As shown in Figure 1, there were 19 studies which met the inclusion criteria. Most excluded studies failed to meet the inclusion criteria for the intervention (e.g., physician-led, synchronous care) (Supplemental Materials, Appendix 2). PRISMA Flow Chart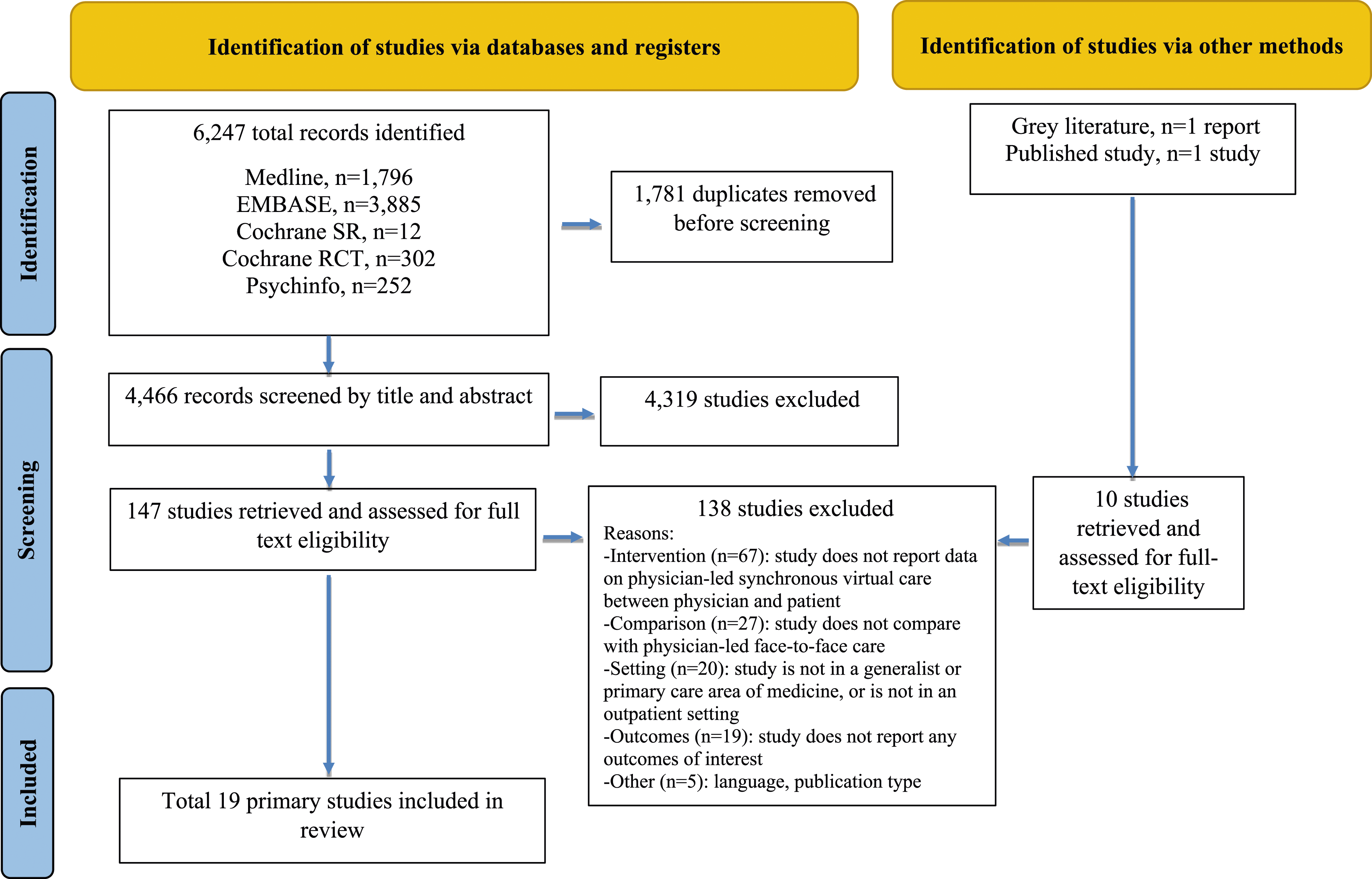
Study Characteristics
Summary of Study Characteristics (n = 19 Studies)
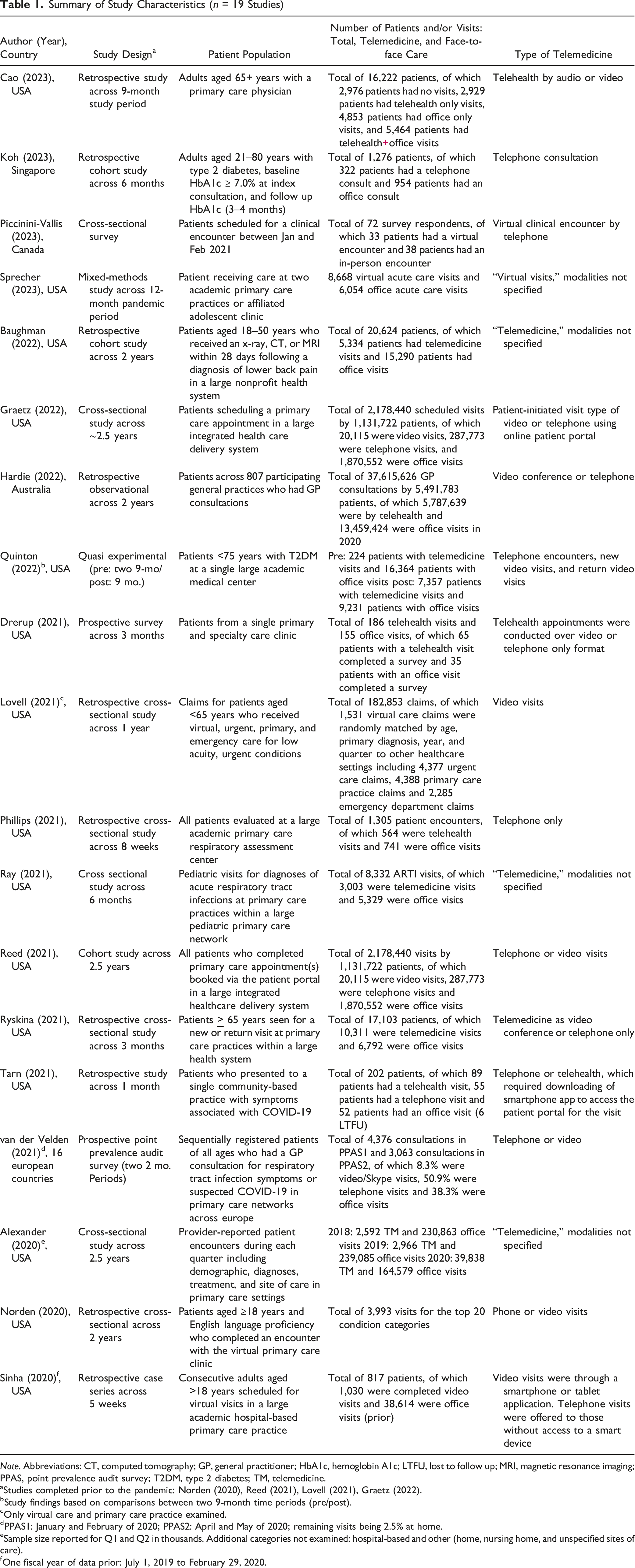
Note. Abbreviations: CT, computed tomography; GP, general practitioner; HbA1c, hemoglobin A1c; LTFU, lost to follow up; MRI, magnetic resonance imaging; PPAS, point prevalence audit survey; T2DM, type 2 diabetes; TM, telemedicine.
aStudies completed prior to the pandemic: Norden (2020), Reed (2021), Lovell (2021), Graetz (2022).
bStudy findings based on comparisons between two 9-month time periods (pre/post).
cOnly virtual care and primary care practice examined.
dPPAS1: January and February of 2020; PPAS2: April and May of 2020; remaining visits being 2.5% at home.
eSample size reported for Q1 and Q2 in thousands. Additional categories not examined: hospital-based and other (home, nursing home, and unspecified sites of care).
fOne fiscal year of data prior: July 1, 2019 to February 29, 2020.
Healthcare System Use
Summary of Findings by Outcome
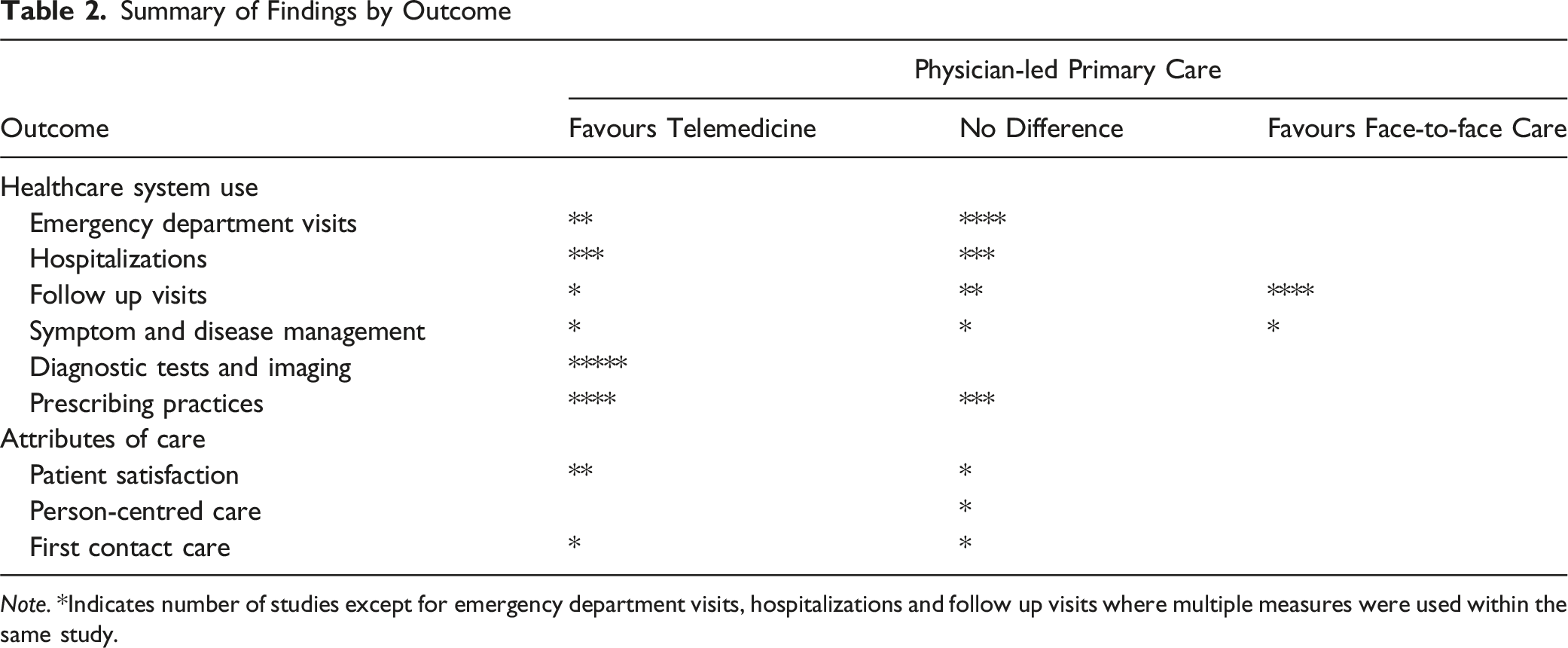
Note. *Indicates number of studies except for emergency department visits, hospitalizations and follow up visits where multiple measures were used within the same study.
There were heterogeneous study designs and findings from three studies that examined symptom and disease management. Among those studies, one study showed no difference in diabetes care when measured by changes in HbA1c (Koh, 2023); one study provided a pre/post pandemic comparison of telemedicine to face-to-face care which indirectly showed the benefits of telemedicine for diabetes management (Quinton, 2022); and one study showed primary care telemedicine visits were less likely to have blood pressure and cholesterol assessments (Alexander, 2020). Five studies examined diagnostic tests and imaging and the overall trend was consistent in showing fewer diagnostic tests and imaging after a primary care telemedicine visit. Notably, in the study by Norden (2020) which accounted for 19 health conditions, the reverse was shown in a subset of patients, whereby more images were ordered after a primary care telemedicine visit for the specific diagnosis of arthropathies and related disorders and spinal disorders (Norden, 2020). Prescribing was examined in seven studies that included different patient populations. Slightly more studies (4 of 7 studies) showed fewer prescriptions with a primary care telemedicine visit while the remaining studies (3 of 7 studies) showed no difference in prescribing practices between care modalities. In one study, overall there were no differences, however in a subset of patients, a primary care telemedicine visit was more likely to lead to prescribing central nervous system drugs for anxiety disorders and face-to-face care was more likely to lead to prescribing medications for otitis media, spinal disorders, and arthropathies and related disorders (Norden, 2020).
Attributes of Primary Care
There were three studies that examined patient satisfaction or experience using surveys on a small sample of patients. Findings suggested that patients were satisfied with primary care telemedicine visits overall and in specific domains of care including concern and explanations provided by the physician (Sinha, 2020; Sprecher, 2023), however findings also showed no differences for similar evaluation metrics used in a separate study (e.g., doctor listened to concerns, convenience, care explained, patient-physician communication), and less patient satisfaction for the metrics of staff friendliness and amount of time with doctor (Drerup, 2021). Only one study used a validated measure of person-centred care (Patient-Perceived Patient-Centredness Questionnaire) and showed no differences in total scores and scores for ‘healthcare process’ (e.g., provider explanation and understanding, goals for treatment aligned, patient satisfaction) and ‘roles’ (e.g., patient and provider roles in care). However, primary care telemedicine visits scored higher on ‘context and relationship’ (e.g., provider-patient relationship in terms of trust, caring, compassion, listening, comfort, knowledge about family life, respecting beliefs and values) (Piccinini-Vallis, 2023; Ryan, 2019). There were two studies that examined appointment timing, a measure of first contact care. One study showed primary care telemedicine visits were more likely to occur one day after scheduling (Graetz, 2022), whereas no difference was found between care modalities in the amount of time required to receive a follow up consultation after receiving a test result (Hardie, 2022).
Discussion
When included studies were synthesized by outcome, the results of the systematic review highlight trends that warrant further exploration for physician-led synchronous telemedicine compared to face-to-face care in primary care. Owing to an evidence base which was heterogeneous, based on observational studies, and determined to be of high risk of bias, we are unable to provide definite conclusions. Notable trends may suggest fewer or a similar number of emergency department visits, hospital visits, and prescribing, and fewer diagnostic tests and imaging for patients who received a primary care telemedicine visit compared to patients who received face-to-face care. There were too few studies for the remaining outcomes to identify consistent patterns. Overall, results need to be interpreted cautiously given the retrospective nature of the majority of included studies and susceptibility to selection bias and confounding.
The largest number of studies examined the outcome of healthcare use and showed an overall trend of telemedicine not leading to more acute care such as emergency department visits or subsequent hospitalizations. Our results are consistent with previous studies. A recent population-based study that compared telemedicine to in-person care using several provider types and accounting for patient baseline factors showed that telemedicine was less likely to be followed by emergency department visits, hospitalizations, and intensive care unit admissions at seven and thirty days (Mondoux, 2023). In another recent study examining the extent of telemedicine, results showed that primary care physicians who provided 80–100% of patient care by telephone or video had fewer emergency department visits compared to primary care physicians who provided less than 20% of patient care by telemedicine (Kiran, 2023). Similarly, another recent study showed no change in emergency department visits per 1% increase in the proportion of telemedicine provided by primary care physicians (Chami, 2023). However, our synthesis had conflicting results with previous work by Mondoux (2023) which showed telemedicine visits were less likely to have in-person primary care revisits (Mondoux, 2023). Our synthesis showed the reverse in a subset of studies. This inconsistency is likely owing to differences in study design and analysis whereby the previous study included matching and statistical adjustment to create more comparable groups and also used discrete definitions of follow up visits. Future studies that can improve on the use of routinely collected health data and observational designs would help to minimize heterogeneity across studies. Our review taken with other studies cited suggest future work may involve performing a cost analysis from a healthcare system perspective and studying telemedicine’s impacts across different health conditions encountered in primary care (Norden, 2020).
In this systematic review, several studies suggested a trend of telemedicine not leading to more prescribing of antibiotics or other types of medications, however findings were mixed depending on the health condition. One study identified that central nervous system drugs for anxiety disorders were more often prescribed in relation to a primary care telemedicine visit whereas for health conditions more suitable to an in-person assessment (e.g., otitis media), we observed more prescribing for face-to-face care. These findings are consistent with emerging evidence on synchronous telemedicine mental health care (Lo, 2022, September 19) and the context of care delivery in primary care settings, where initial triage by providers is based on perceived ability to identify acute illness and clarify indications for treatment which may influence one modality over another. Similarly, a patient’s self-triage or self-assessment of their condition based on acuity or severity may influence their preferred care modality. The inability of included studies to account for these selection biases is a notable limitation, however the way in which patients and providers prioritize care has been identified as an indication of the appropriateness of telemedicine, a key metric of its future viability (Mondoux, 2023; Report of the Virtual Care Task Force, 2022). For the outcome of diagnostic tests and imaging, included studies showed an overall trend of fewer investigations with telemedicine. This finding was consistent in a small set of diverse studies and requires further investigation to tease out whether the results represent a benefit (or harm) to patients or the healthcare system. Fewer diagnostic tests and imaging could be interpreted in many ways, for example, findings may indicate that non-essential services were delayed given the pandemic-related lockdowns or findings may represent a trend towards the more appropriate use of limited resources (Choosing Wisely Canada, 2021, January 6) as the included studies were conducted over different time periods of pre-pandemic and pandemic. There were only three or fewer studies that examined disease and symptom management, patient satisfaction, person-centred care, and first contact care. With too few studies to identify consistent patterns, these areas warrant future focus, especially as it relates to concerns of telemedicine including timely access, maintaining continuity of care, technology barriers, health equity, and the importance of the patient-provider relationship (Hawe, 2023; Lapointe-Shaw, 2023; Litchfield, 2021; Parker, 2021).
A majority of included studies were conducted in the United States at a point in time when telemedicine was emerging in response to the pandemic and therefore were pragmatic in nature and based on routinely collected health data from the EMR or other administrative data sources. Therefore, the limitations of this systematic review include the uncertain applicability of study findings to other healthcare systems and time periods outside of the pandemic. Additionally, few included studies accounted for patient level differences between groups and studies were susceptible to selection bias whereby patient participation with a specific clinical site or health system may have varied based on condition severity, need for care requiring a physician, choice and motivation to seek care, or other patient- and provider-level factors related to care access (Casey, 2016; Cowie, 2017; Mc Cord, 2019). In addition, findings from this review do not reveal how the public engaged with their local public health measures or the multitude of personal reasons, views or beliefs as to why some patients might have sought care during the pandemic period of restricted mobility, or not. Consequently, our evidence base is only suggestive, and uncertainty remains as to whether equivalent or better healthcare system outcomes are achieved with a primary care telemedicine visit compared to face-to-face care.
The focus of this systematic review on primary care physicians excluded the interprofessional nature of primary care teams involving nurses, nurse practitioners, pharmacists, social workers, and other allied health professionals and is therefore limited in having a narrow scope. While our systematic review was based upon a model of care whereby 80% of primary care is provided by family physicians (Lapointe-Shaw, 2023), future work may be positioned to build upon our evidence base to include studies that consider interprofessional or team-based models of care (e.g., family health teams) which additionally encompass providers such as physician assistants, nurse practitioners and allied health professionals. However, the impetus of this work was to efficiently assemble the evidence on the healthcare system outcomes of telemedicine in the primary care setting as restrictions for telemedicine and lockdowns were being lifted, and the health-related impacts of the pandemic in the primary care setting were unknown at the time.
Given that the body of evidence was based largely on observational studies which included heterogeneous designs and analyses, we did not perform a formal assessment using the GRADE framework (Balshem, 2011). Our systematic review did not reveal discrepancies in regard to patient numbers by care modality or by the year the study was conducted and published. Therefore, the focused nature of our systematic review allowed us to complete an efficient outcome-based synthesis of relevant literature and was conducted using a large, comprehensive literature search.
Our review is unable to address the outcomes of telemedicine currently. There are several additional unanswered questions that could be better addressed using more diverse study designs beyond EMR-based retrospective observational studies. Future work involves examining multidisciplinary teams in relation to telemedicine which is becoming more common but not the norm in many countries and jurisdictions around the world. Future work includes developing a better understanding of who receives telemedicine and why; what types of care can be effectively and safely provided by telemedicine versus face-to-face and for which health conditions; examining renumeration paid for telemedicine compared to face-to-face care as part of any cost analysis; and studying primary care outcomes relevant to patients and the healthcare system so that advances in the delivery and receipt of care in the primary care setting continue to be realized.
Conclusion
The COVID-19 pandemic led to substantial change in healthcare delivery and access where health systems worldwide pivoted to telemedicine overnight. Primary care is the cornerstone of health systems globally, and while telemedicine has remained beyond the pandemic, there has been little evidence on the impact of those changes on relevant primary care outcomes. Our work has identified several shortcomings in the methods used among included studies, however our synthesis provides a foundation for future work on telemedicine in primary care settings. Future outcome-based research and synthesis are needed across all relevant outcomes in primary care settings and should include measures beyond patient satisfaction to begin to understand more in-depth the delivery and impact of primary care in this new digital model of care. It will be paramount to identify which attributes of primary care, patient characteristics, and patient clinical care are most vulnerable to the changes in the delivery of primary care. This knowledge can help to support a future, increasingly hybrid version of primary care.
Supplemental Material
Supplemental Material - Physician-Led Synchronous Telemedicine Compared to Face-To-Face Care in Primary Care: A Systematic Review
Supplemental Material for Physician-Led Synchronous Telemedicine Compared to Face-To-Face Care in Primary Care: A Systematic Review by Keyna Bracken, Jennifer Salerno, and Ling Yang in Evaluation & the Health Professions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by McMaster University, Department of Family Medicine, Pilot Project Funding Program.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.