
Abstract
Background
Critical illness is a life-threatening condition impacting millions of patients globally each year. Critically ill patients often need to be transported within the hospital during their care and the safety and efficiency of transportation are key for good health outcomes. There is a lack of knowledge about the processes and safety of intra-hospital patient transport in low-resourced health care settings.
Objective
This study aimed to understand health workers’ experiences of the process and the safety of intra-hospital transportation of critically ill patients in Tanzania.
Methods
Qualitative in-depth interviews were conducted with 15 health workers involved in the care and transportation of critically ill patients in five Tanzanian hospitals. Purposive sampling identified participants. Data were analysed using thematic analysis, guided by the Donabedian quality of care framework.
Results
Three themes of health workers’ experiences of patient transportation were identified, the first two related to structures and the third to processes: (i) the design and organisation of hospitals did not facilitate the initiation and conduct of quick, short and safe transport for critically ill patients; (ii) hospitals lacked resources for safe, effective transportation of critically ill patients; (iii) there were weaknesses in the preparation for, conduct of, and handover of information concerning the transportation of critically ill patients. Health workers in Tanzania faced substantial challenges in ensuring safe transportation due to hospital infrastructure limitations, resource shortages, and inadequate processes.
Conclusion
We conclude that the transport of critically ill patients is overlooked in hospital services in Tanzania, despite the importance of safe intra-hospital transportation in preventing deaths. Feasible solutions to these challenges are necessary for reducing high mortality and morbidity among critically ill patients.
Introduction
Critical illness is ‘a state of ill health with a high risk of imminent death if care is not provided’. 1 Critical illness is a large global challenge, affecting an estimated 45 million adults each year. 2 In-hospital mortality rates due to critical illness are estimated to be between 18 and 82% within 30 days of hospital admission,3–6 with many of these deaths being potentially preventable. 7
Critically ill patients are cared for in all parts of hospitals 8 and frequently require transporting between units. 9 Transportation is needed to obtain care unavailable at the initial location, 10 with critically ill patients needing to be moved between imaging units, laboratories, operating rooms, emergency units (EUs), intensive care units (ICUs), high dependency units (HDUs) and general wards.11,12 The condition of critically ill patients remains life-threatening during transportation, and provision of safe, effective intra-hospital patient transportation is vital for continuous care. 13
Several studies describe the risks of intra-hospital transportation.10,14 Frequent team-related issues, patient management problems, and equipment failures have been reported.15–17 Previously a neglected topic, the safety of intra-hospital transportation has recently received greater attention,10,13 with an emphasis on the need for appropriate equipment, trained staff, and the development of specific protocols. 17 However, there is still a lack of knowledge about transportation in low-resourced settings, and a lack of specific focus on the transportation of critically ill patients. 16 This study aims to describe health workers’ experiences of the process and the safety of intra-hospital transportation of critically ill patients in Tanzania.
Methods
Study design
We employed a qualitative descriptive design to study health workers’ experiences of the process and safety of intra-hospital transport of critically ill patients. 18 Our methodological approach was based on the Donabedian framework; widely used in health systems research to assess the quality of care and identify measures for improvement. The framework offers a way of understanding the interactions between structure, process and outcomes. Our focus was on analysing health workers’ experiences to identify the structures and processes relevant to patient outcomes; our study did not include measurement of those outcomes.
Study setting
Tanzania is a lower-middle income country in East Africa with a population of 66 million. Health services are decentralized; the Ministry of Health is responsible for policy and oversight, while much of the management and service delivery is delegated to local government. Services can be categorized according to the following levels: local village dispensaries, ward-level health centres, district hospitals, regional referral hospitals, zonal and national hospitals. Advanced critical care services are limited and mainly concentrated at regional and national hospitals; district-level hospitals often lack specialized staff and equipment.
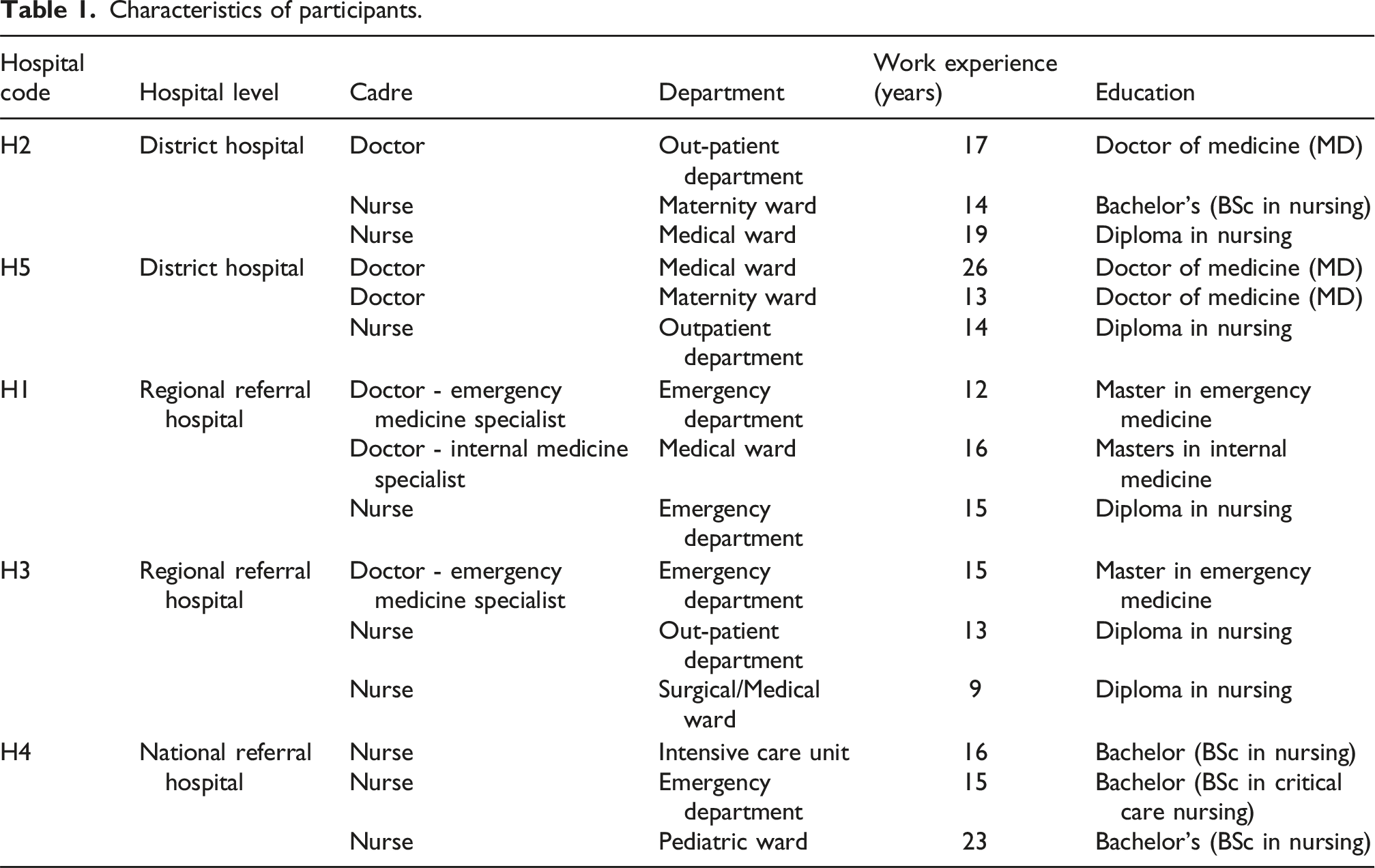
This study was part of the ‘Provision of Essential Treatment in Critical Illness’ project investigating the care of critically ill patients in Tanzania. We used purposive sampling for hospital sites and participants within sites, to gain varying perspectives. 19 Hospital sites were purposively sampled to represent different levels in the health system and patient volumes, from hospitals where there were pre-existing relationships with the hospitals and ease of access during the COVID-19 pandemic. We included five hospitals; two at district, two at regional and one at tertiary level. Hospitals H2 and H5, with 156 and 120 beds respectively, were smaller district hospitals serving semi-urban populations, providing general inpatient and outpatient services located in several buildings around courtyards and linked by short outdoor walkways. Hospital H1, with 280 beds, was a regional referral facility in an urban area. It offered some specialized services and was arranged in multiple buildings connected by outdoor, covered walkways. Hospital H3, with 360 beds, was a busy regional referral hospital in an urban setting, managing 1500 to 1800 patients daily across several multi-storey buildings containing the clinical departments and support services. Hospital H4 was a large referral and teaching hospital with 1500 beds organized in specialized units in several multi-storey buildings.
Participants and recruitments
Characteristics of participants.
Data collection
Semi-structured interviews were conducted between October 2020 and June 2022 by two qualitative researchers (EM and JM). The interviews were conducted in person in the local language, Swahili, and lasted between 45 and 60 min. Interviews were audio recorded, transcribed verbatim and translated into English. A bilingual researcher, EM, checked translations against the audio recorded interviews.
Data analysis
We applied a thematic approach21,22 to code, analyze and interpret the data using abductive analysis 23 which guided iterative reflections between the data and the Donabedian quality of care framework with a focus on ‘structures’ and ‘processes’. 24 We categorized standardized operating procedures (SOPs) and written guidelines as “structures”: the physical and organizational resources available to transport patients, which also included staffing levels, medicines, and equipment. We categorized the actions taken to provide care to patients (in this case observing vital signs, moving patients and providing treatment) as processes.
The translated transcripts were managed in NVivo-12 qualitative data software and read several times by JM and EM for familiarization before undertaking coding. Consistency of codes was ensured through one researcher randomly selecting and analyzing 5 of 15 (33%) of the transcripts by the other researcher as guided by the approach suggested by Sarantakos, 25 discrepancies were discussed, and standards set to guide the rest of the coding process. Similar codes were grouped into categories and then themes which were revised as new codes and categories emerged. As part of sense-checking the categories and themes, the researchers communicated preliminary findings with health workers at the institutions and adjusted interpretations as required. In the final phase, the results were refined through a review done by a clinical expert (TB) who considered the relevance and applicability of the identified categories and themes to clinical settings.
Ethics
The study was granted ethical approval by the Tanzanian National Institute for Medical Research (NIMR/HQ/R.8a/Vol. IX/3537), Ifakara Health Institute (IHI/IRB/No. IHI/IRB/No: 51 –2020), and the London School of Hygiene and Tropical Medicine (REF 22 866).
Results
Summary of findings.
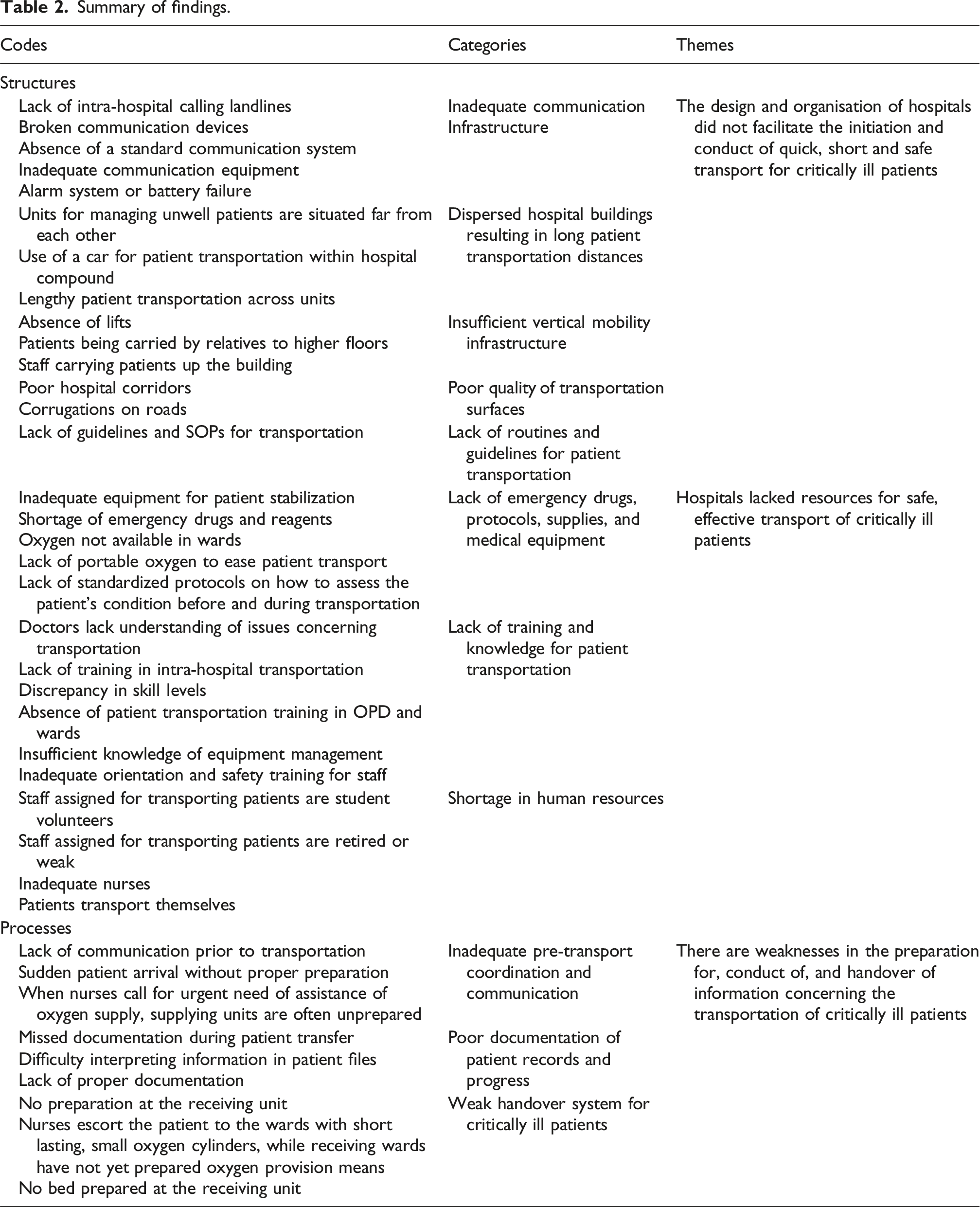
Structures: Design and organisation of hospitals
We found that the design and organisation of hospitals did not facilitate the initiation and conduct of quick, short and safe transport for critically ill patients. When transporting patients, health workers expressed difficulties due to inadequate communication infrastructure and physical design (including dispersal over a large site, multiple floors, and inadequate flooring). The hospitals in this study lacked adequate and functional communication equipment to facilitate coordination required for the initiation of safe transportation, which hindered communication between departments. There was a lack of working landlines, failed alarm systems, and those that existed were often non-functional due to a lack of maintenance or missing parts, as participants explained: “There are no landlines that maybe you could call to inform them we have a critically ill patient who needs oxygen so prepare the cylinder.’’ Doctor, H3 “Some communication devices are broken, and in some of the departments there is no phone charging cable.” Nurse, H3. “Previously there was an alarm in the labour room, but I think it has problems or the battery died.” Nurse, H2
Participants also reported that the construction of hospitals did not consider the logistical feasibility of transporting patients. Care stations were too distant, with departments scattered across the premises without considering their related duties. In some extreme cases, patients had to rely on ambulances or private cars for transport within the hospital site, causing unnecessary delays, long transportation times, and discomfort (for example patients with fractures, bleeding wounds, or a painful condition). These factors increased risks to patients, as described here: “Our hospital is so dispersed there are point of care which you need to have transport - a car - to move a patient within the hospital, this causes delays of care especially when you have a critically ill patient, it is a big challenge.” Doctor, H1 “So, you know it involves taking a patient out of an oxygen cylinder carrying him/her down to a car, and then taking him/her out to the car again then taking the patient out to the cylinder again all way back to the ward.” Doctor, H1
Hospitals had insufficient infrastructure to move patients across different levels. Critical departments were often located on higher floors, but with no lifts, leading to manual patient transportation, which was both undignified and risky. Patients were carried upstairs by relatives or hospital staff, placing a burden on all parties involved and compromising patient safety: “OPD [outpatient department] is located on the second floor and there is no lift, the only means is for a patient to be carried like a piece of luggage.’’ Nurse, H1 “A patient may stay there even for 15 minutes until you get assistance to carry the patient up” Nurse, H4
The hospitals in this study had poor quality patient transportation surfaces: corridors and roads were uneven and had corrugations, leading to complications during patient transport, such as disconnection of tubes and equipment. This posed a risk to the stability of equipment and tubes, jeopardizing patient care and safety: “You can’t find any road like this, there are corrugations and an inserted tube may come out from the patient and after arriving you may have to restart inserting tubes [e.g., intravenous cannulas], and do resuscitation again in the ward.” Nurse, H5
Structures: Lack of resources
Health workers described a lack of the resources needed to facilitate safe patient transportation including drugs, medical equipment and other supplies such as portable oxygen. Health workers identified specific gaps in resources: “There are emergency drugs, that you think at the regional hospital level they should be available, sometimes they are missing for weeks. It may reach a point you are being told that reagents are not available, you cannot do anything, and there is no money”. Doctor, H1 “There is a challenge with diazepam it can be there today and tomorrow it is out of stock. There is a time the patient should buy.” Nurse, H3 “We expect nurses will do those ABC [Airway, Breathing, Circulation] and hand to me a patient who is stable, but the challenge is there is not enough equipment to be able to stabilize the patient.” Doctor, H1
There was also a lack of training, with staff having had little or no training about patient transportation. Training that was available was considered to be superficial and only available for a small number of staff, creating a skills discrepancy among health workers. Some nurses reported feeling ill-equipped, and that they had insufficient knowledge about how to manage the equipment used for patient transportation: “The issue is also a discrepancy in the level of skill.” Nurse, H2 “I think there is a need for training (on intra-hospital patient transportation) because we are doing other things just by praying that God helps me”. Nurse, H3
Additionally, hospitals faced a shortage of personnel dedicated to patient transportation, relying on intern students, relatives and non-medical staff to handle critical patient transport. In some hospitals, staff who were not physically fit were assigned the duty of transporting patients. These factors raised concerns about the adequacy of the workforce in ensuring safe and efficient transport of critically ill patients: “Yes, they have assigned these students who are volunteering to transport patients.” Nurse, H5 “During the night is worse, most of the time patients they are moved by their relatives” Nurse, H2 “They assign those old and weak staff to stay there at OPD and EMD to transport patients. I can say they (hospital administration) believe that any person can escort the patient.” Nurse, H4
Hospitals lacked standardized guidelines for intra-hospital patient transportation, leading to inconsistent practices among nurses. The absence of clear protocols resulted in uncertainty regarding pre-and post-transport preparations, decision-making processes, and necessary actions during transportation, further compromising patient safety. “We don't have SOPs [standard operating procedures] for critically ill patients at our ward.” Nurse, H1 “There is no guideline to guide health workers when the blood oxygen level drops by a certain degree from baseline.” Nurse, H2
Overall, structural weaknesses in hospital design, resources, and staffing posed barriers to safe and effective transport of critically ill patients.
Processes: Preparation for, conduct of, and handover of information
Weaknesses were identified in the preparation for, conduct of, and handover of information concerning the transportation of critically ill patients. Participants identified weaknesses of unclear routines and coordination between departments. Health workers pointed out the challenges of poor preparation, execution, and handover procedures for critically ill patients, including insufficient coordination, communication, and documentation of medical records. They noted that these issues contributed to disruptions, delays, and compromised patient care continuity within hospitals: “So mostly we are getting patients from OPD and sometimes in very unstable conditions.” Nurse, H1 “You may just suddenly find the patient is already at the stairs, there and nurses calling for oxygen, which puts the patient’s life at risk.” Nurse, H4
Health workers reported challenges in interpreting information on patients’ files due to poor documentation or a lack of documentation accompanying patients. Documentation of patient transfers was often missing, and a reliance on verbal communication, leading to discrepancies between verbal information and written records. This lack of clarity and organization made it challenging for participants to ensure the accurate transfer of information, potentially compromising patient care: “Suppose in the theatre they tell you a patient lost a lot of blood, but you might find that is not documented in the file to what extent was the bleeding” Nurse, H2 “The way vital sign is taken; the nurse may fail to interpret them in detail and document” Doctor, H3 “Depends on who is on duty, others will just come and give you verbal information, and sometimes what is written in the form and what you are being told is different.” Nurse, H1
Participants noted challenges in the handover of transported patients. Receiving units were not well prepared for the arrival of patients, which affected care continuity. In some instances, nurses escorted patients with small oxygen cylinders expecting the receiving unit to have oxygen, but this had not been communicated in advance. At other times, patients arrived to occupied or unprepared beds at the receiving units. The absence of standardized routes and practices for patient handover created confusion and inefficiencies, compromising patient care and safety: “Also, they may ask you to take the patient but when you arrive there you find them not ready, they haven’t prepared themselves and you escorted the patient with a small cylinder knowing that this amount will be sufficient to transfer the patient from here to the ward when you find they are not prepared you will have to struggle, that is a challenge, most of the time you will face those challenges inwards.” Nurse, H1 “For this every ward with its power! It depends on which department the patient has been taken to, if is from EMD and is in critical condition and has been taken to ICU there is continuity of care because we are all speaking the same language, but if has been taken from EMD to ward six, for example, and is in the critical condition these are two different languages.” Nurse, H5
The lack of standardized pre-transport processes led to variation in patient transport practices, resulting in unstable conditions during transit and worsening patient health upon arrival.
Overall, we found that the transport of critically ill patients was overlooked in hospital services. It was striking that health workers’ experiences were overwhelmingly focused on challenges; they did not describe any positive experiences around patient transportation.
Discussion
Health workers’ accounts of transporting critically ill patients within Tanzanian hospitals showed considerable challenges with structures and processes. These can be summarized as related to: the design and organization of hospitals; a lack of resources; and weaknesses in the preparation for, conduct of, and handover of information concerning the transportation of critically ill patients.
Our study adds to the existing literature by providing qualitative insights into intra-hospital transportation challenges from the perspective of health workers in low-resource settings. While previous research has primarily focused on high-income settings and on clinical outcomes or equipment issues during transport,14,26 there has been limited exploration of the structures and processes in these contexts. By examining the experiences of Tanzanian health workers, we show how structural challenges, such as hospital design and resource gaps, and weaknesses in processes, can impact patient transport and hence safety. Here, we consider the consequences of these structures and processes in terms of the potential for poor patient outcomes, and some potential improvements that could mitigate the risks to patient safety.
Poorly organized and poorly executed patient transport can significantly contribute to morbidity and mortality, 27 with adverse effects occurring in up to 70% of transportations. 26 Hospital design is key in facilitating safe transportation of critically ill patients.28,29 When hospital units and buildings are far apart and lack communication infrastructures to facilitate transportation, as found in our study and other settings,28–30 responses during emergency communication can be delayed 31 and patient outcomes can be compromised. 32 Inadequate design extends to hospital layouts, such as elevator-dependent vertical designs which may worsen complications by causing transport delays, and substandard quality of patient transportation surfaces such as uneven floors. This has been associated with compromised safety and comfort, particularly for orthopedic patients using traction or splinting devices.33,34
Understanding why critically ill patients require intra-hospital transfer is important when addressing transport challenges. Transfers often arise because essential care services such as intensive monitoring, specialized diagnostics, or treatments are located in different parts of the hospital. Changes in the use of hospital space, such as positioning HDUs, EUs, and ICUs close together, 35 could minimize delays due to space constraints and congestion, and shorten intra-hospital transfer times. Adopting alternative care models (e.g. emergency rooms) can also reduce the need for transportation and help improve patient outcomes. 36 Additionally, patients may need escalation of care when deterioration occurs in wards. Improving early recognition of patient deterioration, enhancing bedside care capacity, and optimizing hospital layout to co-locate key services could reduce the frequency and urgency of transportation.
We found, in common with a previous study, 26 a lack of routines and guidelines for transporting critically ill patients, including specified personnel and equipment. This poses risks and challenges for health care providers and patients. 37 The transport of these patients should be performed in compliance with evidence-based medical recommendations, 38 in particular, the transport of patients with contagious diseases. 39 Protocols and guidelines for patient transfers across all health care facilities 40 have been proposed to mitigate complications and unplanned outcomes. 41
During patient transportation, complications may occur, with up to one-third of cases being equipment related. 26 Our study found hospitals lacked resources for safe, effective transport of critically ill patients. Inadequate resources hinder the ability to provide timely care, thus increasing the risk of patient complications during transportation. 40 Studies report that using appropriate equipment and staff can minimize complications and ensure optimal benefit to the patient.42,26 It has been suggested 43 that a minimum of two people, one of them a nurse who is trained at caring for critically ill patients, should accompany critically ill patients when being transported.
The use of innovative transport modes (e.g., specialized stretchers or carts equipped with necessary medical equipment) to facilitate safe and efficient transportation of critically ill patients while ensuring continuous care, has shown promising results in reducing adverse events, shortening transport time and improving transport efficiency. 39 While many of the challenges found in our study reflected broader contextual constraints such as chronic shortages of equipment, supplies, and infrastructure limitations that require national-level investment, 44 some areas may be more manageable by local improvement. For example, hospitals can provide low-cost equipment such as portable oxygen and improve internal communication systems (such as functional phones or alarms). While a lack of resources for essential emergency and critical care has been found in hospital wards in Tanzania, these resources are low-cost and cost-effective for the care of critically ill patients. 45
Other resources that are needed include training and standardization of processes. We found health workers lacked training and knowledge about patient transportation, this has also been the case elsewhere. 46 Specific training to health workers about patient transportation could improve patient outcomes.47,48 Standardization of intra-facility transport practices can also ensure patient safety and improve the quality of care during transport. 49
Beyond the structures and resources for the transportation of critically ill patients, we found that the processes were also sub-optimal – for pre-transport coordination and communication, documentation in patient medical records, and in handover to other health workers. This finding echoes similar observations in other settings.50,51 Team coordination, communications, and resource availability are vital should an emergency or an unexpected situation occur during transportation. 40 Communication and collaboration with other health care providers in the receiving destination should be undertaken prior to transportation 40 and the receiving team should confirm their readiness for receiving the patient before the transportation commences.40,41 Inadequate communication, documentation and handover can lead to misunderstandings, errors, and delays, all of which can have severe consequences for patient safety. These issues can lead to potential risks and adverse events during transport. To address these concerns, studies have highlighted the importance of implementing educational programmes for health workers involved in intra-hospital transport. 50
Apart from the immediate safety risks, our findings also highlight concerns about the dignity and personhood of critically ill patients during transport. Health workers’ descriptions of patients being carried “like luggage” or transported by non-medical staff and relatives point to practices that can undermine the respectful and humane treatment of patients at their most vulnerable. While resource shortages and infrastructural gaps certainly shape these practices, they may also reflect underlying norms and attitudes that deprioritize patient dignity during critical moments or when they are unable to advocate for themselves. Addressing the safety of intra-hospital transport must therefore go hand in hand with ensuring that critically ill patients are seen and treated as individuals deserving of respect, agency, and compassionate care, even when systems are under pressure.
The strengths of this study are: the qualitative methodology that allowed an exploration of health workers’ perspectives, the purposive sampling which ensured the inclusion of a diverse range of participants and sites, and the sense-checking process which validated the findings and informed our understanding of the potential implications for improvements to structures and processes. Limitations included the small number of hospitals included, which whilst conducive to study logistics, limits the translatability of findings to broader populations or contexts. Additionally, while in-depth interviews provide rich insights, they may not fully capture the broader organizational or systemic factors influencing intra-hospital transportation, potentially emphasizing individual perspectives over contextual elements.
Overall, our findings show that improving both hospital structures and work processes could have the potential to make patient transport safer. Better communication systems, enough essential supplies, clearer guidelines, shorter transport routes, and training for staff are simple and low-cost ways to reduce risks. Improved routines, handover coordination and targeted staff training, could be feasible even within existing resource limits. In addition, reallocation of existing resources could overcome some of the resource constraints – it is often described that the care of critically ill patients is a neglected part of hospital systems 52 and resources could be reallocated to their transportation from less prioritized parts of the system. These lessons could be transferable to other hospitals in low-resource settings facing similar problems.
Conclusion
To achieve good outcomes for critically ill patients, ensuring safe and effective intra-hospital transportation is key. As one participant told us: “critically ill patients are not just luggage”. Advanced, high-cost interventions are not necessarily required, it can be sufficient to ensure that the fundamental care of critical illness, as outlined in the recent global Essential Emergency and Critical Care (EECC) consensus, 7 is consistently provided to all critically ill patients throughout their stay in the hospital, including during transportation. Improving key areas such as establishing safe routines, ensuring availability of essential supplies, implementing the EECC processes, developing a reliable communications infrastructure, and strengthening basic handover protocols could be effective. Streamlining patient transportation through clear protocols would enhance efficiency and safety, while aligning practices with EECC principles would facilitate continuity of care and address the patients’ most urgent needs.
Footnotes
Acknowledgments
The authors also wish to express their appreciation to the administration and staff of all five hospitals for their support during the data collection process. Additionally, the authors are thankful to all the study participants for their contributions to the data collected during the study.
Ethical consideration
The study was granted ethical approval by the Tanzanian National Institute for Medical Research (NIMR/HQ/R.8a/Vol. IX/3537), Ifakara Health Institute (IHI/IRB/No. IHI/IRB/No: 51 –2020), and London School of Hygiene and Tropical Medicine (REF 22 866). All participants gave consent for their participation.
Authors’ contributions
JMa and EM conceptualized and designed the study, acquired and analyzed the data, and developed the first draft of the manuscript. TB conceptualized and designed the study and analyzed the data. KK contributed to acquisition of data. TW, KK, OO, COS, JO, ME and JMc contributed to the design and analysis. All the authors interpreted the findings, critically revised the manuscript and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Welcome Trust [221571/Z/20/Z], as part of the ‘Innovation in low-and middle-income countries’ Flagship.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.