
Abstract
Pineal parenchymal tumor of intermediate differentiation (PPTID) is a rare, primary tumor of the pineal gland. Due to its rarity, there is no consensus on optimal therapeutic strategies or standard characterization of the tumor’s behavior. Here, we report 2 new cases of PPTID and an extensive review of the literature involving the use and extent of radiation therapy. Patient 1 is a 54-year-old male who presented with PPTID and drop metastases in the spinal cord, received cranial spinal irradiation (CSI), and experienced recurrence 3.5 years after treatment. Stereotactic body radiation therapy (SBRT) helped the patient into remission for 9 months. Patient 2 is a 32-year-old male with a local PPTID at presentation who went on to receive surgical resection followed by focused adjuvant radiation therapy to the pineal tumor bed. He then presented 6 years after treatment with extensive disseminated recurrence and died due to leptomeningeal disease (LMD) about 4 years after recurrence. The available literature on PPTID is limited and reported cases of LMD with ongoing follow-up in PPTID are scarce. Our report adds to the current known PPTID cases, contributing to the information available regarding prognosis and treatment response. Although an optimal therapeutic strategy for PPTID still cannot be determined, data from the literature suggest that utilizing radiation therapy in patients with low-risk disease and gross total resections as well as the use of upfront CSI have the potential to improve patient progression and survival outcomes.
Keywords
Introduction
Pineal gland tumors represent only about 4% of all central nervous system (CNS) primary tumors,1,2 which include germ cell tumors, gliomas, and those arising from the pineal parenchyma itself. Pineal parenchymal tumor is further subdivided into 3 groups with the most benign-acting tumors known as pineocytomas (PC: WHO grade 1), the most aggressive-acting tumors known as pineoblastomas (PB: WHO grade 4), 3 and the third group known as pineal parenchymal tumor of intermediate differentiation (PPTID: WHO grade 2 and 3). While the behavior of PC and PB are generally agreed upon, the behavior of PPTID is ambiguous with widely varying aggressiveness. Given the rarity of cases with PPTID, constituting only 10% of all pineal parenchymal tumors, and the historical inability to accurately predict clinical behavior (eg, probability of recurrence and propensity for drop metastasis), there are no consensus guidelines available to direct management of PPTID.
The current standard of care for PC is maximal safe resection alone, and PB often requires the addition of adjuvant radiation therapy (RT), chemotherapy, or a combination thereof after surgery. In contrast, for PPTID, a wide array of therapeutic regimens incorporating RT has been utilized without a clear consensus regarding its role. For example, it is unclear of the role of adjuvant RT in the setting of gross total resection (GTR) vs subtotal resection (STR) or the appropriate field extent, mainly regarding local RT vs cranial spinal irradiation (CSI). Additional complexity is added when considering the utility of chemotherapy or combination chemoradiotherapy (chemoRT) and is compounded by the fact that GTR is sometimes difficult to achieve, given the location of these tumors and the proximity to vital structures.
Herein, we report 2 cases of PPTID treated at our institution. Both patients recurred after years-long periods without evidence of disease progression.
Case presentations
Patient 1 is a 54-year-old male who presented to his primary care physician with gait instability, headaches, arm tremors, and sleep disturbances. He also experienced progressively worsening light-headedness and increasing short-term memory loss for the previous few months. Magnetic resonance (MR) images of the brain demonstrated a 3.7 cm maximum dimension tumor in the pineal region with suspicious nodules in the cerebellum, causing obstructive hydrocephalus (Figure 1A-C). MR images of the spinal cord demonstrated nodular enhancement in the cervical, thoracic (Figure 1D and I), and lumbar spine, which were suspicious for drop metastases. He underwent a third ventriculostomy and biopsy. Pathology revealed morphology consistent with a PPTID and a Ki-67 of 4-5%. Synaptophysin stains were positive in nearly all the sections examined. Prior to CSI, the patient’s short-term memory loss subjectively resolved after recovery from surgery. He subsequently received definitive CSI of 3600 cGy in 20 fractions. This was followed by an 1800 cGy boost in 10 fractions to the pineal gland tumor (5400 cGy in total) and a 360 cGy boost in 2 fractions to drop metastases at the conus medullaris (T12-L2 spinal levels, 3960 cGy in total). Subsequent MR images showed good treatment response, and 9 months after the end of RT, MR images of the brain and spinal cord demonstrated a stable pineal region compatible with post-treatment changes and no evidence of leptomeningeal or cord metastasis. Furthermore, the patient did not experience any apparent high-grade toxicity, such as anorexia or nausea, from CSI treatment and reported minimal change in cognition, including changes in short-term memory. Mini-Mental State Examinations (MMSE) administered at 1 month and 10 months after CSI were both within normal limits, scoring 29 out of a total of 30 at each time point. Patient 1 pre-treatment (A-D, I), post-treatment (E-H, J), and recurrence (K-L) MR images. Prior to CSI, (A) axial T1 post-contrast, (B) axial T2, and (C) sagittal T1 post-contrast MR images demonstrate PPTID occluding the aqueduct of Sylvius, causing obstructive hydrocephalus and enlarging the lateral ventricles. (D) The thoracic spinal cord displayed extensive lesions suspicious of drop metastases, which are outlined in arrows. (I) An axial T1 post-contrast MR image is provided of the circled region in (D) the thoracic spine, which shows a cluster of drop metastases in the thoracic spinal cord. After CSI, (E) axial T1 post-contrast, (F) axial T2, and (G) sagittal T1 post-contrast MR images demonstrated no residual disease and relief from the obstructive hydrocephalus, resulting in smaller lateral ventricles. (H) The thoracic spinal cord post-treatment no longer showed the previously seen lesions. (J) An axial T1 post-contrast MR image is provided at the level of the circled region in (H) the thoracic spine, an area that had previously shown a cluster of drop metastases but now shows no lesions. However, (L) a focus of enhancement on the left lateral aspect of the cervical cord at level C6-7 appeared 3 and a half years after completion of CSI treatment and increased by 3 mm over the course of 3 months. (K) The axial T1 post-contrast MR image is provided at the level of the circled region in (L) the cervical spine. The lesion responded well to SBRT for 9 months (data not shown).
Surveillance imaging showed no evidence of disease for 3 years (Figure 1E-H and J). Unfortunately, on a routine follow-up MR imaging 3.5 years after the completion of treatment, an increased 5.3 mm × 5 mm x 3.5 mm focus of enhancement was seen along the left lateral aspect of the cervical cord at the level of C6-7 vertebrae. A lumbar puncture demonstrated no malignant cells in the cerebral spinal fluid (CSF). Repeat imaging 3 months later demonstrated that the lesion grew to 8.3 mm × 5 mm x 3.6 mm as the only site of progression (Figure 1K–L). Upon review, evidence of this lesion had been present on MR imaging 1 year prior. At the time of discovery, the patient did not have any subjective neurological symptoms. However, as the evidence of disease recurrence was convincing by imaging, the patient underwent stereotactic body radiation therapy (SBRT), receiving 2750 cGy in 5 fractions to the C6-7 spinal lesion. The lesion responded well to SBRT and nearly completely resolved. The patient was subsequently followed closely with surveillance MR imaging and was in remission for 9 months. A brain and spine MRI then showed slightly increased size of the residual enhancing mass at the tectum at the primary site and slightly increased enhancing nodules at C1-2 and possibly T7, suggesting disease progression. Next generation genomic sequencing was attempted but could not be completed due to insufficient tissue. The patient was started on alkylating chemotherapy with procarbazine and CCNU, selected based on previous case reports. He received 3 cycles at the time of this report, though he required a dose reduction and treatment delay after the first cycle due to neutropenia and thrombocytopenia. He also suffered a traumatic fall with rib fracture and hydropneumothorax developed requiring chest tube placement, hospitalization and rehabilitation. After the second cycle of chemotherapy, he developed pleural effusion and hyponatremia requiring a second hospitalization. Of note, at the time of first evidence of disease progression and at subsequent disseminations, the patient received a total of 3 lumbar punctures, but the CSF cytology never showed malignant cells. His disease was stable at the time of this report, but the patient has reported persistent shortness of breath and developed moderate dysmetria.
Patient 2 is a 32-year-old male who presented to his primary care physician with blurry vision. MR images of the brain demonstrated a 3.1 cm maximum dimension pineal lesion obstructing the aqueduct of Sylvius, causing obstructive hydrocephalus (Figure 2A-C). He underwent a right frontal burr hole and third ventriculostomy with endoscopic biopsy followed by a right posterior occipital craniotomy a month later to excise the pineal mass, which was achieved with at least a near-total resection with post-operative MRI brain showing only minimal patchy enhancement in the tumor bed at pineal region. Pathology revealed morphology consistent with a PPTID and a Ki-67 of 2-3%. Mitoses were rare and there was no necrosis. The neoplastic cells were diffusely positive for chromogranin and neuron-specific enolase (NSE). MRI pan-spine at initial diagnosis showed no evidence of disease dissemination, which was confirmed by CSF cytology negative for malignant cells 1 month after craniotomy. He subsequently received focused adjuvant RT of 5400 cGy in 30 fractions to the pineal tumor bed. Surveillance MR images of the brain demonstrated no evidence of disease (Figure 2D-F) but no spine MRI was performed after. Patient 2 pre-treatment (A-C), post-treatment (D-F), and recurrence (G-L) MR images. At time of diagnosis, (A) axial T1 post-contrast, (B) axial T2, and (C) sagittal T1 post-contrast MR images demonstrate PPTID occluding the aqueduct of Sylvius, causing obstructive hydrocephalus and enlarging the lateral ventricles. He underwent a right posterior occipital craniotomy to excise the pineal mass followed by focused adjuvant RT to the pineal tumor bed. For the next 5 years, MR images demonstrated no evidence of disease and relief from the obstructive hydrocephalus, resulting in smaller lateral ventricles, as seen in (D) the axial T1 post-contrast, (E) axial T2, and (F) sagittal T1 post-contrast MR images. Within the year following his last clean MR images, he exhibited recurrence of the PPTID, as seen in (G) the axial T1 post-contrast, (H) axial T2, and (I) sagittal T1 post-contrast MR images, and extensive dissemination of disease (outlined in arrows) in the (I) cervical, (J) thoracic, and (K) lumbar spine. (L) An axial T1 post-contrast image of the largest drop metastasis, which was seen circled in (K) the lumbar spine, is provided.
He presented to his primary care physician, 8 months after his last MR images showing no evidence of disease progression and 6 years after the initial diagnosis/craniotomy, with 3 months of worsening back pain associated with bilateral radiation to the feet. MR images of the brain demonstrated a 1.8 × 1.6 × 1.2 cm contrast-enhancing pineal region mass (Figure 2G-H). Another enhancing mass was seen in the floor of the fourth ventricle, and multifocal enhancing masses were observed along the medulla and upper cervical spinal cord (Figure 2I). Numerous enhancing lesions were present bilaterally in the cerebellum, a small subarachnoid contrast-enhancing lesion was present in the right parieto-occipital sulcus, and an enhancing lesion was present along the left VII/VIII nerve complex. MR images of the spinal cord demonstrated diffuse leptomeningeal disease (LMD), with the largest drop metastasis measuring 2.1 cm at the L3-4 spinal level (Figure 2J-L). Of note, despite the diffuse dissemination and LMD per imaging, CSF cytology was negative for malignant cells. He received salvage RT with CSI with 3960 cGy in 22 fractions to the spine and 3060 cGy in 17 fractions to the whole brain, followed by a 540 cGy boost in 3 fractions to the lumbar spine. He began salvage chemotherapy after CSI with cisplatin. Unfortunately, his disease progressed again, though only in the pineal region (with stable disease in spine), 22 months after salvage CSI. He received palliative RT to the left temporal lobe and posterior fossa lesions and subsequently chemotherapy with temozolomide. However, diffuse LMD progression developed in the brain while on temozolomide. The patient died in only 10 months after the last course of palliative brain RT, 3.5 years after salvage CSI, and about 9.5 years after the initial diagnosis. No detailed neurocognitive studies were performed on this patient, but he remained at high performance status with Eastern Cooperative Oncology Group (ECOG) performance status 0 until half a year prior to his death.
The timelines of both patients can be observed in Figure 3. Patient timelines for (A) patient 1 and (B) patient 2. (A) Patient 1 received CSI therapy, went into remission for 39 months, recurred but was treated successfully with stereotactic body radiation therapy, and is now presently in remission. (B) Patient 2 received a craniotomy followed by focused adjuvant radiation therapy, went into remission for 72 months, recurred with diffuse leptomeningeal disease (LMD) that could not be fully treated by therapy, and died at 120 months.
Literature review/discussion
Patient characteristics from included studies. RT: radiation therapy, CSI: cranial spinal irradiation, WB: whole brain radiation, WVI: whole ventricle irradiation, GTR: gross total resection, STR: subtotal resection, PR: partial resection, NED: no evidence of disease, FNR: French National Registry, LS: Lyon Series, -: unknown, +: chemotherapy a part of treatment.

aThese are the total PPTID patients presented within each study. Some of the studies included non-PPTID tumors and those patients were thus excluded.
bRecurrence data varies in specificity among the studies and as such the available data is what has been reported.
cLu et al. is a systematic review in addition to a 3 patient case series and has thus been listed separately.
dFauchon et al as completed prior to the WHO 2000 PPTID designation and patients are thus presented as grade I-IV pineal parenchymal tumors. Grades II and III have been incorporated into this data.
eMottolese et al incorporates data from 2 distinct patient datasets, the French National Registry (FNR) and the Lyon series (LS).
A more contemporary review of 103 PPTID patients in the National Cancer Database (NCDB) found that surgery with GTR was the only treatment-related prognostic factor, with chemotherapy and RT having no impact on survival. 5 However, the authors of the review do acknowledge that the use of RT should not be ruled out given newer evidence showing an impact on progression-free survival (PFS). 5 Interestingly, the authors also presented 3 patients that had been treated at their institution with adjuvant RT (2 with STR and 1 with GTR), and all 3 were alive without recurrence with follow-up times ranging from 4.1 to 6.3 years. 5 Contrary to the previous works, in 1 of the largest metanalyses heretofore conducted incorporating 29 studies and 127 PPTID patients, Mallick et al found that adjuvant RT significantly improved overall survival (OS) to 252 months compared to 168 months for patients who underwent surgery alone. 6 They further reported that extent of surgery and use of adjuvant chemotherapy did not significantly impact OS. 6
In this review, we have gathered 29 individual reports along with 5 metanalyses/systematic reviews on the use of RT for the treatment of PPTID since the WHO designation in 2000. These studies are presented in Table 1. Most of the patients in these reports were treated with adjuvant RT due to the presence of high-risk features, including STR, biopsy only, grade III disease, or metastases at initial presentation. These high-risk characteristics have long been the most common and accepted reasons for incorporating RT into the treatment regimen for PPTID. For example, 1 study reported a PFS of 72.9 months and OS of 94.1 months in a five-patient case series where 3 patients had a partial resection and 2 patients had biopsy only in the setting of disseminated disease at initial presentation, and all received RT. 7 Another study, involving 6 high-risk patients (2 with biopsies only and 4 with residual disease post-resection) reported a mean OS of 42 months for those who received adjuvant RT. 8 Only 1 of the 4 patients who received adequate radiation dose (>50 Gy) recurred at the time of follow-up and the single recurrence was at 111 months. 8 The lone patient who did not receive RT recurred at 14 months. 8
However, data regarding some patients with GTR and low-grade disease were reported as well, thus providing insight into the impact of RT for patients traditionally thought of as low risk for metastasis or recurrence. For example, Yu et al. 9 wrote 1 of the largest case series with 27 PPTID patients and found that 5-year PFS was improved from 50% (4/8) to 84.2% (16/19) and OS from 62.5% (5/8) to 89.5% (17/19) for those who received adjuvant therapy. In this study, all patients received RT, but 2 patients also received chemotherapy. 9 For high-risk patient specifically, 50% (3/6) who received RT recurred while 100% (3/3) of those who did not receive RT recurred and did so earlier. 9 Of the 11 patients with GTR who received adjuvant RT, none had experienced a recurrence at the time of follow-up, regardless of grade. 9
Another large series from MD Anderson Cancer Center of 17 patients with PPTID found that, out of the 6 patients with GTR (7 are presented but 1 died immediately post-surgery so was not included in the data), 4 out of the 5 who received adjuvant RT did not recur (single recurrence at 16.8 months), and the only patient with GTR who did not receive any RT recurred early at 12.7 months. This patient went on to receive salvage stereotactic radiosurgery (SRS) to the local recurrence area, which produced a durable response and was disease-free at the last follow-up (at 111 months). Interestingly, 75% (9/12) of patients without CSF dissemination at presentation who received RT and 100% (5/5) of those with GTR who received RT were treated with upfront CSI. 10
Pusztaszeri et al. reported on the use of upfront CSI with a pineal boost and chemotherapy in the setting of a grade III PPTID that had underwent biopsy alone. 11 Remarkably, the patient had a complete response and had no evidence of disease (NED) 72 months post-treatment at last follow-up. 11 Another study demonstrated that upfront CSI was utilized for 60% (6/10) of grade II and 75% (6/8) of grade III PPTID patients who received adjuvant therapy, which frequently included chemotherapy, due to high-risk features. 12 Importantly, they showed no difference in the probability of recurrence or death when compared to the lower-risk cohort with better initial prognosis, thus implying a significant advantage for upfront therapy prior to disease dissemination. 12 They also found that neuraxial spread, among tumor grade and extent of resection, were predictive of patient outcome. 12
A number of other studies reported the use of CSI in the more traditional salvage setting, (ie, after metastatic dissemination). Kathpal et al described an interesting case where a patient who recurred with disseminated disease after initial local RT therapy was treated with CSI administered to the specific sites of spinal metastases (ie, C7-T5 and L5 to sacrum). 13 Four months after this salvage CSI, more lesions appeared in his spine from T5-T10 and T12-L3. 13 Tellingly, all these recurrences were outside the salvage CSI field, thus revealing the impact of the extended field radiation. 13 The use of salvage CSI is not unique to this case. PPTIDs have a long-documented history of leptomeningeal spread and dissemination after local-only therapies (ie, local RT or surgery), requiring salvage CSI for treatment to stabilize or cure disease.14,15
In another study, CSI was administered to 2 patients who presented with disseminated disease and underwent biopsy only, while the other 3 patients without dissemination underwent local RT only after STR. 7 Despite having a worse initial prognosis, the mean PFS for the 2 patients who underwent CSI was 83.5 months, while those who underwent local-only RT had a mean PFS of 53 months. 7 Ito et al. 8 corroborated these findings by reporting that all patients with extended local RT (2/6) or CSI (1/6) did not recur, despite the CSI patient having disseminated disease at presentation. 8 Furthermore, the patients who received local RT only and the patient that did not receive any adjuvant therapy experienced recurrent disease, 1 of which was disseminated recurrent disease. 8
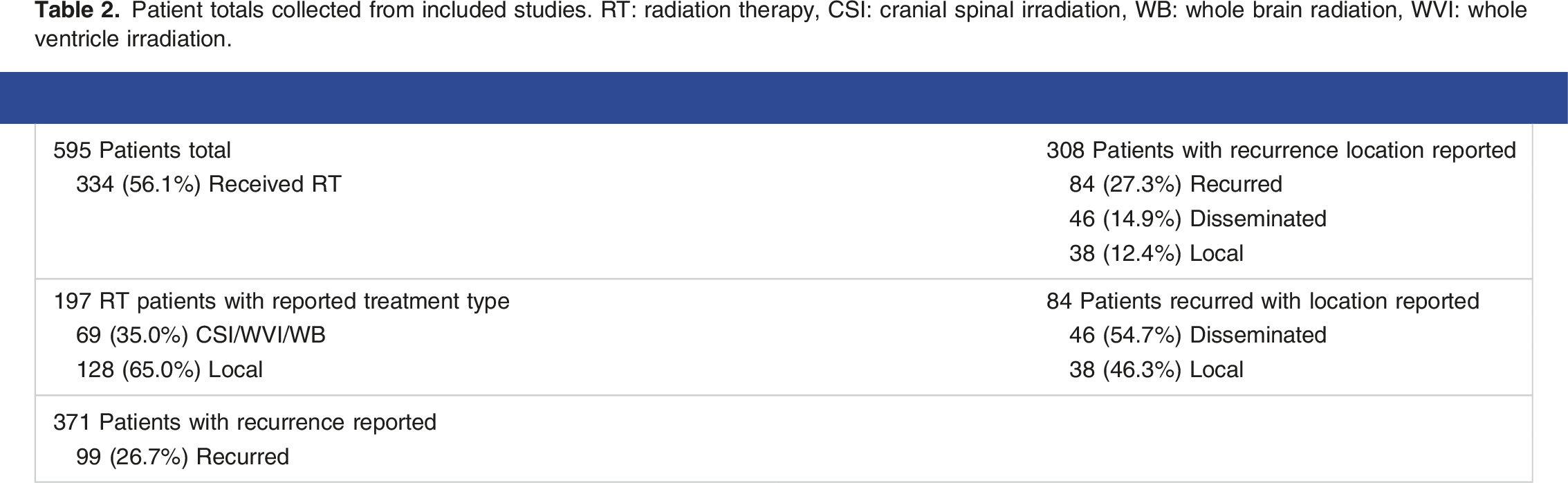
Patient totals collected from included studies. RT: radiation therapy, CSI: cranial spinal irradiation, WB: whole brain radiation, WVI: whole ventricle irradiation.
Result summary
-GTR is the only consistent treatment-related prognostic factor. -Adjuvant RT significantly reduces the risks of recurrence in the setting of localized disease with or without GTR but may not have an impact on survival. However, data indicates potential benefits for PFS and even OS, particularly for patients with low-risk disease (eg, lower than grade 3 PPTID with GTR and no CSF dissemination). -More than 50% of patients at the time of disease progression will have disseminated disease. -Upfront CSI is more frequently offered to patients with high-risk features, such as STR or biopsy only for surgery, grade 3 disease and/or CSF involvement at presentation. However, the value of upfront CSI treatment is questionable, although both our data and reports from the literature review suggest a possibility of achieving long-term disease control (years) if CSI is provided to those even with positive CSF or diffuse dissemination at initial presentation or as a salvage. -The role of chemotherapy is even less defined than that of RT. There is no standard regimen but procarbazine/CCNU/vincristine, or procarbazine/CCNU, or temozolomide is commonly offered to patients with evidence of LMD or diffuse dissemination.
We acknowledge the limitations of this study being retrospective study in nature with low levels of evidence although a thorough review of the literature was performed, and a very limited number of patients from our own institution as well as from the community included.
Conclusions
Our case series contributes to the understanding of the use of RT for PPTID and the potential benefit of CSI therapy for patients with PPTID. However, as reviewed, the literature on this topic is sparse and retrospective by nature, including our case series. Therefore, definitive conclusions should not be made, and systematic prospective studies are needed.
Radiation has traditionally been utilized in the setting of PPTID with negative prognostic features, including STR, biopsy only, and grade III disease. In 1 of the largest and most recent metanalyses to date, Takase et al 2 recommends combination treatment (RT, chemotherapy, or ChemoRT) for grade III disease and those with uncommon characteristics. 2 However, some of the aforementioned studies have shown that grade does not necessarily predict progression or survival outcomes. The data compiled from the literature presented herein implies a possible role for RT in the setting of low-grade disease and GTR. Many of these studies reveal that low-grade PPTID with GTR often do not recur (or recur very late) when treated with upfront RT. Although this observation is made in the retrospective setting, it warrants further clinical investigation to validate the use of upfront RT and assess safety and efficacy.
CSI has often been reserved for patients presenting with metastatic disease or positive CSF samples. However, multiple reports exist of patients (including our patients presented herein) with known metastatic disease having CSF cytology negative for malignant cells,17,18 bringing into question the reliance on this procedure for treatment planning. Additionally, 1 of the historical concerns with CSI is the possibility of treatment toxicity, particularly the acute severe gastrointestinal (GI) toxicities, bone marrow suppression, and the late onset cognitive decline with short-term memory deficits. However, newer technology facilitating highly conformal techniques such as volumetric modulated arc therapy (VMAT) and proton therapy mitigate off-target toxicity, reducing the risk of severe GI toxicities and bone marrow suppression. 19 Notably, neither of our patients had white matter changes or observed neurocognitive decline. Moreover, we observed rapid and severe neurocognitive decline in our patients due to tumor progression, thus arguing for the role of CSI to prevent disease progression upfront. A myriad of reports has been provided in this review detailing the impact of CSI on disseminated/recurrent disease and its success in the upfront setting, prior to any metastasis. These data have elucidated the potential of CSI to produce long periods of PFS. Notably, 1 of the patients presented herein, who initially presented with disseminated disease, received CSI, which provided a complete response and 3.5 years of PFS, which is similar to the PFS after salvage CSI in the second patient, who developed LMD 6 years after previous definitive local RT for the localized disease at the initial presentation.
After summarizing these observations and data, we propose the following to help guide our practice for now pending future updates: (a) it is reasonable to offer patients local adjuvant RT for localized disease at initial presentation regardless of the extent of surgery or grade; (b) it is reasonable to consider the use of CSI only in the setting of diffuse dissemination and/or LMD for PPTID treatment; and (c) it is reasonable to withhold chemotherapy until diffuse dissemination and/or LMD occurs for salvage therapy.
Footnotes
Author contributions
C.L. and C.Z. collected the information for and wrote the case presentations, generated all figures, and prepared the manuscript for submission. J.C. performed and wrote the literature review and generated all tables. M.J.B. and C.Z. provided patient information and critical review of the manuscript. C.Z. conceived the manuscript design. All authors reviewed, revised, and approved the final version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The authors received no financial support for the research, authorship, and publication of this article.
Ethics statement:
Written informed consent was obtained from the individuals or their legal representatives for the publication of the images and data included in this article. Institutional ethical approval is not required for case studies.