
Abstract
Background:
Magnetic resonance imaging (MRI) is often employed as the diagnostic modality of choice in occult and suspected pathological femoral neck fractures. We evaluated the clinical utility of MRI scan in this patient population.
Method:
Retrospective observational analysis of cases with a radiologically occult or suspected metastatic pathological neck of femur fracture.
Results:
From a total of 894 femoral neck fractures treated in our institution, 100 patients had and MRI scan pre-operatively for either occult fracture or suspected fracture secondary metastatic disease. Magnetic resonance imaging confirmed the presence of 13 simple fractures. A total of 14 patients had pathological features suggestive of metastasis, of which 12 were clearly visible on plain radiographs. Surgical plan did not change after MRI for any of these pathological fractures.
Conclusion:
Results of this study demonstrate that an MRI scan had an impact on treatment selection only when a simple but radiographically occult fracture is suspected and but not in the context of suspected metastatic pathological fractures.
Introduction
Hip fractures remain a major public health concern due to an ever-increasing ageing population. The incidence of hip fracture in the United Kingdom is estimated at over 65 000 cases annually in 2017 with an estimated health and social care cost of £1 Billion. 1 A projected trend from the number of proximal femoral fractures in England from 1998 to 2008 collected from Hospital Episode Statistics, showed that by 2033 approximately 100 000 patients annually will require surgery costing £3.6 to 5.6 billion (inflation adjusted). 2 In most cases, proximal femoral fractures are related to the presence of osteoporotic bone disease coupled with a history of a low energy fall. 3 In contrast, a subset of patients demonstrates absence of clear history of injury, atypical radiological features, or past history of malignancy. This leads to suspicions of fractures associated with a malignant lesion in the femoral neck and described as pathological fracture. 4
It has been established that two-thirds of all long-bone pathological fractures occur in the femur, of which almost half involve the proximal femur while about 20% are within the intertrochanteric region. 5 This makes the proximal femur the most commonly affected bone with metastatic disease in the appendicular skeleton. 6 In addition, the incidence of metastatic bone disease has increased because of the longer survival of patients with bone ‘seeking’ cancer. The sensitivity and specificity of magnetic resonance imaging (MRI) in the diagnosis of pathological fractures secondary to malignancy are well established and hence became the modality of choice in such cases.7,8 The use of MRI scan to confirm the diagnosis and prevent potential disastrous outcome of missed fracture has received wide attention in the literature. 9
This study investigated the implication of obtaining an MRI scan to confirm the diagnosis of metastatic disease in a fractured neck of femur which is clearly visible on plain radiographs. In our study, we focused on three principal points. First, review our institution’s practice of confirming the diagnosis by MRI scan in elderly patients with femoral neck fracture either occult on plain radiographs or of suspected oncological nature. Second, the eventuality of finding on MRI scans evidence of oncological lesion on acetabular side. Third, the impact of MRI scans results on surgical treatment plans within this group of patients.
Methods
A retrospective observational analysis of consecutive 104 patients who had MRI scan of the hip over a 26-month period between July 2009 and August 2011 among a total population of 894 hip fractures managed in our institution within this period. Institutional agreement was obtained before the study. Four patients were excluded because they were unable to tolerate the MRI scan due to pain and claustrophobia. The study population comprised 32 male and 68 female patients with a median age of 81 (interquartile range: 70-88) years. All patients had clinical features of neck of femur fracture on initial assessment with loss of straight leg raise, inability to bear weight, groyne or hip pain, and pain on attempted rotation and axial loading of the hip. Figure 1 outlines participants’ demographics and the study flow diagram.
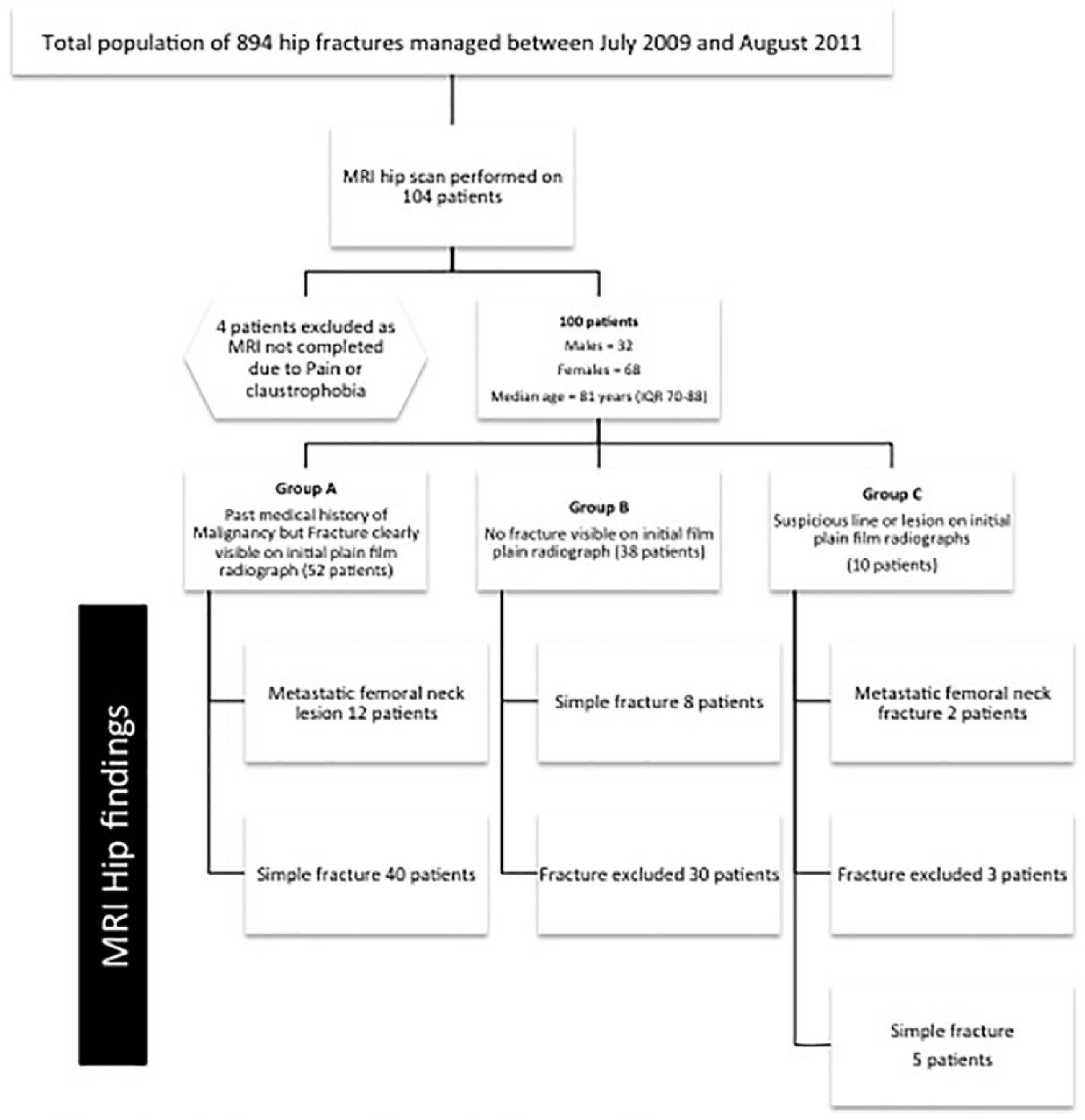
Standards for reporting of diagnostic accuracy (STARD) flow diagram.
The findings of plain radiography, which preceded MRI, were recorded. These comprised fractures clearly visible, no fracture visible, or suspicious line or pathological lesion. All patients had anteroposterior (AP) pelvis X-ray films showing both hips and proximal femora, lateral X-ray films of the affected hip and full length femur AP, and lateral views for patients suspected to have a pathological metastatic fracture clinically or radiologically. The MRI scans were all carried out using the same modality and reported by one of three specialist musculoskeletal radiologists available in our centre. All patients had MRI scanning of both proximal femora and pelvis. All image sections reviewed by the specialist radiologists were obtained on 3 T and 1.5 T scanners with coronal fast spin-echo T1-weighted sequence and coronal short tau inversion recovery (STIR) sequence. Field of view included the entire pelvis and proximal femurs for both views, and no contrast was used. Patients with a positive finding of malignant lesion fracture reported on MRI at the level of the proximal femora had their plain radiographs and MRI scans re-analysed by a musculoskeletal radiologist to determine the presence of malignant lesions in the ipsilateral acetabulum.
The data were extracted from the medical records and an online image archiving system by two independent observers. We performed further analysis of the MRI scans reports which showed a positive metastatic lesion of the proximal femur to look for evidence of malignant lesion on the acetabular side on both plain radiographs and MRI scans. Patients’ records were reviewed to note the treatment plan formulated following the initial plain radiographs and identify changes in definitive treatment plans based on the results of MRI scans.
A consultant orthopaedic surgeon was asked to formulate a surgical plan after reviewing the initial plain radiographs first and then after reviewing the MRI scans for all patients included in this study. Plain radiographs and MRI scans were anonymised and placed in random sequence. Pre- and post-MRI surgical plans were then analysed to assess the impact of obtaining the MRI scans on treatment plans.
Statistical analysis software SAS/STAT® SAS Institute Inc. USA© was used to conduct data collation and analyses. To assess the associations between the study’s variables, results were grouped into binary data classified as a categorical variable. The prevalence of results was calculated in each category and adjusted odds ratios (ORs) with 95% confidence intervals (95% CIs) were calculated. The associated probability estimated using chi-square analyses. Successively, multiple binary logistic regression analysis was performed to estimate OR with 95% CI for the relation of plain radiograph results, MRI results, and surgical treatment plans and adjusted for potential confounders taken into account (age and sex).
Results
Three groups of patients were identified, Group A: fracture clearly visible on plain radiograph plus a past medical history of malignancy, Group B: no fracture visible on plain radiograph, and Group C: suspicious line or lesion on plain radiograph (Table.1). Group A (n = 52) comprised 26 patients with a past history of malignancy. In this group, only 12 patients (23.1%) showed a metastatic femoral neck lesion on MRI and all had previous history of malignancy. In Group B (n = 38), only two patients (5.3%) had a history of malignancy. None of the cases had evidence of metastatic fracture on MRI; however, eight patients (21%) showed a fracture which was not visible on initial plain radiographs. In Group C (n = 10), two patients had a history of malignancy and both cases had evidence of metastatic fracture on MRI. Fractures were excluded in three patients, and the MRI scan confirmed the presence of a simple fracture among five patients. These results are further outlined in Table 2.
History of malignancy and MRI results.

Abbreviation: MRI, magnetic resonance imaging.
X-ray view and MRI results.
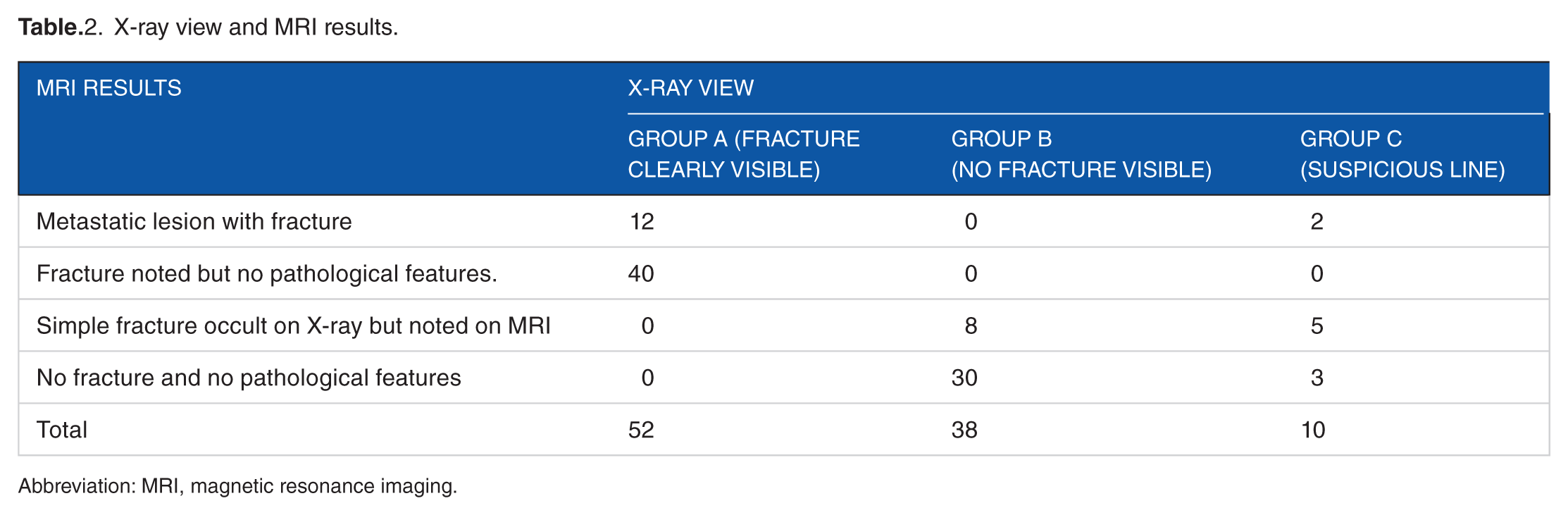
Abbreviation: MRI, magnetic resonance imaging.
The association between past medical history and MRI scan showing evidence of malignant lesion in the proximal femur was statistically significant (OR = 20.26, 95% CI [4.03; 101.91], P value < 0.0003). The association between clear evidence of fracture on the plain radiograph and MRI scan showing evidence of malignancy was also statistically significant (OR = 6.53, 95% CI [1.37; 31.21], P value = 0.0188).
Of the 14 malignant pathological fractures reported, 50% (N = 7) had evidence of malignant lesions in the ipsilateral acetabulum. All the acetabular lesions reported were equally evident on both plain radiograph and subsequent MRI scan. There were no lesions suggestive of primary bone malignancy in the proximal femur.
Analyses of the pre- and post-MRI surgical plans did not demonstrate changes in treatment plans irrespective of MRI findings. Statistically, no significant relation was found between MRI scan showing evidence of malignancy in the proximal femur and change in the surgical treatment plan (OR = 0.60, 95% CI [0.11; 3.34], P value = 0.5604).
Discussion
This study evaluated the clinical utility of MRI scans among 100 consecutive cases in association with the management of femoral neck fractures. Results of this study demonstrate that an MRI scan had an impact on treatment selection only when a simple but radiographically occult fracture is suspected but not in the context of suspected metastatic pathological fractures.
In a previous study by Hossain et al, 7 60% of patients with initially reported normal plain radiographs were later found to have malignant bone lesions. The paradigm governing the utilisation of MRI scan in femoral neck fractures relies therefore on a fine balance between identifying occult fractures and not potentially missing an oncological lesion. In contrast, there is paucity of evidence in the literature supporting the use of computed tomography (CT) of the hip for occult or suspected oncological fractures. Heikal et al 10 reported the identification of 13 neck of femur fracture on CT scan among 65 patients with occult hip fractures on X-rays. In a similar group of patients, the sensitivity of CT scan in occult hip fractures was only 86% with a specificity of 98%. 11 Sadozai et al concluded that MRI scan should be considered when a fracture is suspected but not evident on a standard X-ray view.
In case of suspect fracture but radiographically occult, MRI scan has become a modality of choice with a sensitivity of up to 98% to 100%. 12 In a previous study, 43% of patients with the latter indications had evidence of proximal femoral fracture on MRI scan. The prevalence of metastatic disease detected on MRI scanning for occult fracture in this study was 6% and none required a change in operative management. 8 Similarly, Iwata et al 13 reported 26 of 35 occult hip fractures detected on T1 sequence MRI. These results are echoed in our study where MRI scans performed on patients in groups B and C, identified fractures, not readily evident on initial plain radiographs in 15 of 48 patients. This tool made it possible to finalise a treatment plan for patients.
The rate of metastatic lesions associated with fractures and reported on MRI scans was 14 of 100 cases. A total of 12 of these patients had a previous history of malignancy. All cases were visible on plain radiographs. There were no lesions suggestive of primary bone malignancy in our series. Ramisetty et al 4 in a review of 2223 patients with fracture neck of femur over a 3-year period reported that histological examination of the proximal femur in 27 patients with past history of malignancy and no known bone metastases and eight patients with past history of malignancy and known bone metastases yielded a 15% and 75% positive result of metastatic bony lesion, respectively. In another report, a series of 3700 consecutive proximal femoral fractures, 93 were associated with malignant bone lesions and all of them were metastatic and not primary tumours. 14 A review of the literature equally revealed a negligible incidence of proximal femur primary bone lesion in the elderly patient population.4,15
The initial surgical treatment plan, based on the fracture pattern on initial plain radiographs and clinical indications, for patients with fractured neck of femur associated with metastatic lesion was not changed following the MRI scan. All the patients either had cemented hemiarthroplasty, total hip replacement, or surgical fixation with a long cephalo-medullary nail. This approach was consistent with the British national guidelines for the treatment of metastatic fractures.15-17 The recommendations underline the importance of choosing a surgical treatment modality, which allows early mobilisation and rehabilitation of patients, as well as lasting patient’s life span. In our series, seven patients showed evidence of acetabular lesion present both on the plain radiograph and MRI scans. All the latter cases belonged to Group A, which had clear fracture line on plain X-rays, past medical history of malignancy and evidence of metastatic lesion on MRI scan. These findings had no impact on the surgical treatment plan.
The importance of early surgical intervention on mortality and morbidity in hip fracture has been well documented.18-21 Simunovic et al 22 in a systematic review of 1939 articles reported a significantly lower risk of mortality and lower rates of postoperative pneumonia when surgery is carried out within a period of 24 to 48 hours. In addition, studies looking into causes of delay in surgery outlined that factors such as awaiting medical clearance and the lack of available operative facilities and personnel to be responsible for a large proportion of surgical delays.23,24 Based on available literature, it remains generally accepted that hip fracture surgery should be expedited if medically safe at the earliest point possible.25-27 Our present study adds further support to avoidance of delays, which might be incurred when requesting additional investigations. Regardless of their type, when fractures are clearly visible on plain radiographs, waiting for an MRI provides neither additional diagnostic information nor change in treatment plan.
Conclusion
Clinical utility of MRI in the evaluation and management of acute femoral neck fractures is evident in case of occult changes on initial plain radiographs. Nonetheless, independent from the incidence of oncological hip fractures in this study, the use of MRI scan led to alteration of treatment only when fractures were not clearly visible on initial plain films. In the presence of metastatic lesion associated with a fracture, the use of MRI scanning served only to confirm the diagnosis and had no impact on treatment selection. Diagnostic tools must be tailored to the clinical merit of each case and should not lead to the unnecessary delay of surgical intervention.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
B.B. contributed to study conception and design, acquisition of data, drafting of manuscript, and critical revision. M.A-.T. contributed to the acquisition of data, analysis and interpretation of data, and drafting of manuscript. T.B. contributed to study conception and drafting of manuscript and critical revision.