
Abstract
Background:
Brain metastases are a common complication in a wide range of cancers but are ubiquitous among patients with lung cancer. Limited data are available on the survival of patients with lung cancer and brain metastases in Indonesia. In this study, we aimed to identify the factors that might contribute to and predict survival in patients with non–small cell lung cancer (NSCLC) that resulted in brain metastases.
Methods:
This retrospective study on patients with NSCLC and brain metastases was conducted using data available from the medical records of the Dharmais National Cancer Hospital, Jakarta, Indonesia. The study outcome was survival time, which was associated with sex, age, smoking status, body mass index, number of brain metastases, tumor location, systemic therapy, and other therapies. Descriptive statistics, median survival, Kaplan-Meier graphs, and Cox regression were analyzed using SPSS version 27.
Results:
We included 111 patients with NSCLC and brain metastases in this study. The median patient age was 58 years. Long survivorship was observed among women (median: 95.4 weeks; P < .0003), patients with epidermal growth factor receptor (EGFR) mutations (median: 41.8 weeks; P < .0492), those who received chemotherapy (median: 58 weeks; P < .000), and those who received a combination of surgery and whole brain radiotherapy (WBRT; median: 64.7 weeks; P = .0174). Multivariate analysis showed consistent results for the following factors: sex, EGFR mutations, systemic therapy, and surgery plus WBRT.
Conclusions:
Female sex and EGFR mutations in patients with NSCLC and brain metastases are associated with a high survival rate. Patients who have NSCLC with brain metastases will benefit from treatment with EGFR tyrosine kinase inhibitors, chemotherapy, and surgery plus WBRT.
Introduction
Cancer deaths are prominently caused by lung cancer, which resulted in a total of 1.6 million deaths worldwide in 2012 and is still the leading cause of cancer mortality. 1 Based on its histopathology, lung cancer can be categorized into non–small cell lung cancer (NSCLC) and small cell lung cancer (SCLC). The main subtypes of NSCLC are pulmonary adenocarcinoma, squamous cell carcinoma (SCC), and large carcinoma. 2 Genetic alterations in epidermal growth factor receptor (EGFR) occur in approximately 20% of patients with lung adenocarcinomas in Western countries and 40% to 60% of patients in East Asia. 3 Brain metastases (BM) that develop from NSCLC are the most important cause of death. Lung cancer is estimated to cause 30 000 deaths annually in the United States. 4 Patients with lung cancer that has not metastasized and those who have localized tumor cells show median survival and 2-year survival rates of 15 to 20 months and 20% to 40%, respectively. Moreover, 5-year survival rates have been reported for only 5% of the patients with lung cancer, and the rates can be very low if the cancer metastasizes. 5
Metastatic brain tumors are one of the most common types of intracranial malignancies in adults. In the United States alone, the incidence of metastatic brain tumors is 150 000 to 170 000 cases per year. 6 Lung cancer is the most common cancer that metastasizes to the brain, as approximately 30% to 60% of patients with lung cancers develop BM; the ratio of the number of patients with BM developed from lung cancers and the number of patients with primary brain tumors is 10:1. 7 The survival rate of patients with untreated BM developed from lung cancer ranges from 1 to 3 months. The cumulative incidence rates of BM that developed within 1 year and 5 years of diagnosis of lung cancer in the patients were 14.8% and 16.3%, respectively. 3
Limited data are available on patients with lung cancer and BM in Indonesia. In addition, most of the patients encountered at our center were at an advanced stage of the disease. In this study, we aimed to identify the factors that might contribute to and predict survivorship among patients with NSCLC that resulted in BM.
Materials and Methods
Study design and sampling
In this study, we used retrospective methods, and all data were retrieved from the medical record databases of the Dharmais National Cancer Hospital, Jakarta, Indonesia. Data collection was completed in July 2022. We collected demographic and clinical information on BM from patients with NSCLC who received care at our center, regardless of the treatment approach. Ethical approval was obtained from the Institutional Review Board of Dharmais National Cancer Hospital, Jakarta, Indonesia (NO 096/KEPK/IV/2022). Patient confidentiality was also maintained. Informed consent was not obtained as we used secondary data in this study, and it was not an interventional study.
Patient population
Irrespective of the treatment strategy used at the Dharmais National Cancer Center between January 2018 and February 2022, all patients with BM were included in this study using the total sampling method. Patients whose follow-up times were less than 4 weeks or those who had a primary tumor other than lung cancer were excluded. After data collection and sorting of patients based on the inclusion and the exclusion criteria, 111 eligible patients were included in this study.
Variables
The outcome of this study was the survival time of patients with NSCLC and BM (weeks). Based on the findings of previous studies, we collected data on possible factors that affect patient survival time, including age, sex, smoking status, body mass index (BMI), EGFR status, number of BM, systemic therapy, other therapies, and tumor location. The patients were divided into 2 age groups, and 50 years was selected as the cut-off age. Patients were grouped according to their BMIs based on the World Health Organization BMI classification for adults. Systemic therapy included targeted therapy using EGFR tyrosine kinase inhibitors (TKIs) and chemotherapy, whereas other therapies included radiotherapy and surgical intervention.
Statistical analysis
The retrieved data were tabulated and analyzed using Windows IBM SPSS Statistics version 27. The survival time data were plotted using Kaplan-Meier curves, and comparative analyses were performed using the log-rank test. The Cox proportional hazards method was used for multivariate analysis to determine the factors contributing to survival time. Follow-up time was defined as weeks from the date of metastasis diagnosis until the date of recorded death or the last clinical visit.
Results
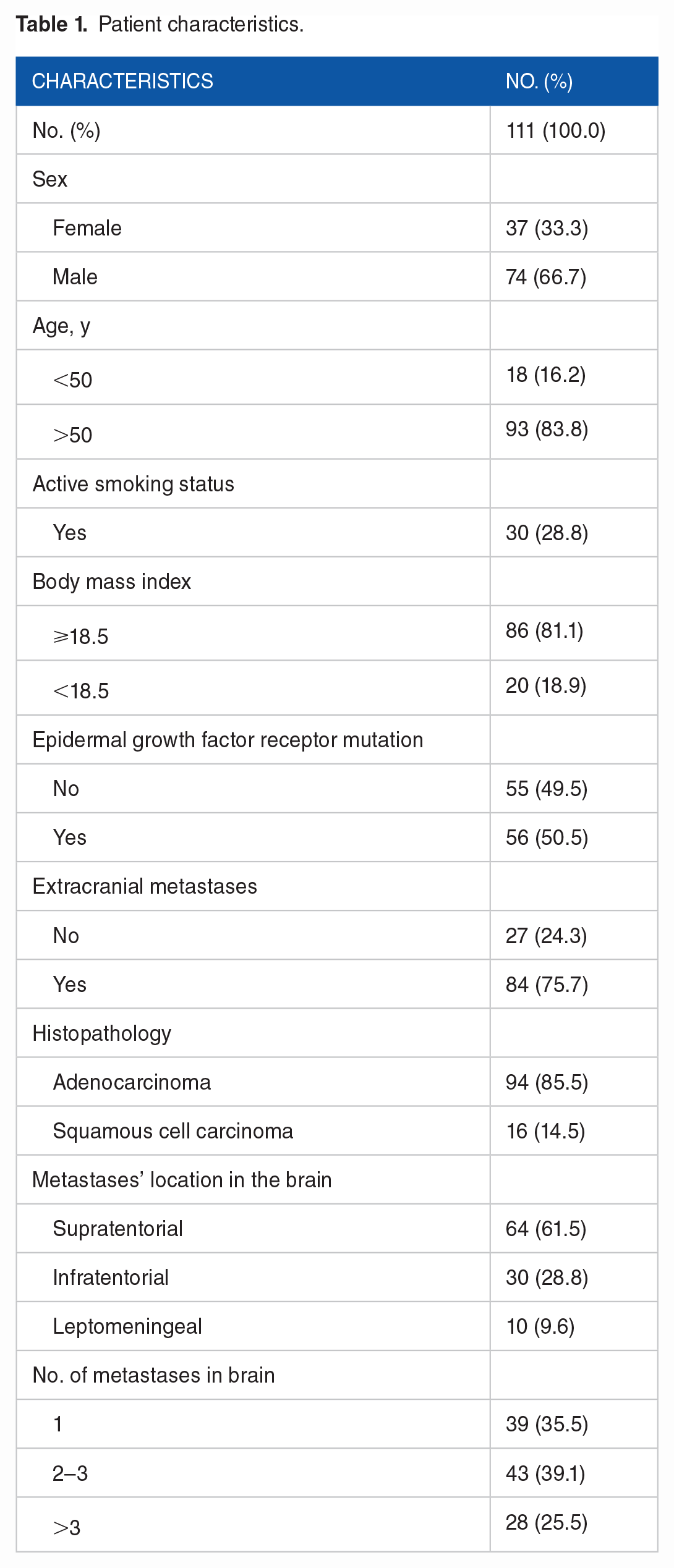
A total of 111 patients who had NSCLC and BM were included in this study. The median age was 58 years (range, 30-80 years), and most participants were men (66.7%); 33.3% of the participants were women. Only 30 participants (28.8%) actively smoked, whereas 71.2% did not smoke. Adenocarcinoma was the most common histopathology found in the samples and affected 85.5% of the patients; most (39.1%) patients had 2 to 3 BM. The characteristics of the participants are summarized in Table 1. As the number of patients who received different kinds of therapies varied, the therapeutic approaches were divided into 2 major groups, namely, groups receiving systemic therapy and other therapies, as described in Table 2. The neurological symptoms experienced by the patients are summarized in Table 3.
Patient characteristics.
Therapies received by participants.

Abbreviations: EGFR, epidermal growth factor receptor; TKI, tyrosine kinase inhibitor; WBRT, whole brain radiotherapy.
Neurological symptoms experienced by participants.

We performed a log-rank test to compare the survival of patients in different sample groups. Median survival was estimated in weeks, and a 95% confidence interval (95% CI) and a P value were used to determine statistical significance. Variables were considered significant if the P value was <.05. The median survival times are described in Table 4. The distribution of survival according to sex (Figure 1), EGFR status (Figure 2), systemic therapy group (Figure 3), and group therapy (Figure 4) is illustrated using Kaplan-Meier curves. Long survivorships were found among women (median: 95.4 weeks; P = .0003), patients with EGFR mutations (median: 41.8 weeks; P = .0492), patients who received chemotherapy (median: 58 weeks; P = .000), and patients who received a combination of craniotomy and whole brain radiotherapy (WBRT; median: 64.7 weeks; P = .0174). In contrast, patients treated with craniotomy alone showed significantly low survival rates (median: 5.4 weeks; P = .0174). Factors such as age, smoking status, BMI, histopathology, tumor location, and number of metastases in the brain did not alter survivorship.
Median survival.

Abbreviations: BMI, body mass index; CI, confidence interval; EGFR, epidermal growth factor receptor; TKI, tyrosine kinase inhibitor; WBRT, whole brain radiotherapy.
Total sample size was 110 because data on survival time were missing for 1 patient.

Kaplan-Meier curves for survival functions according to sex.

Kaplan-Meier curves for survival functions according to EGFR mutation.
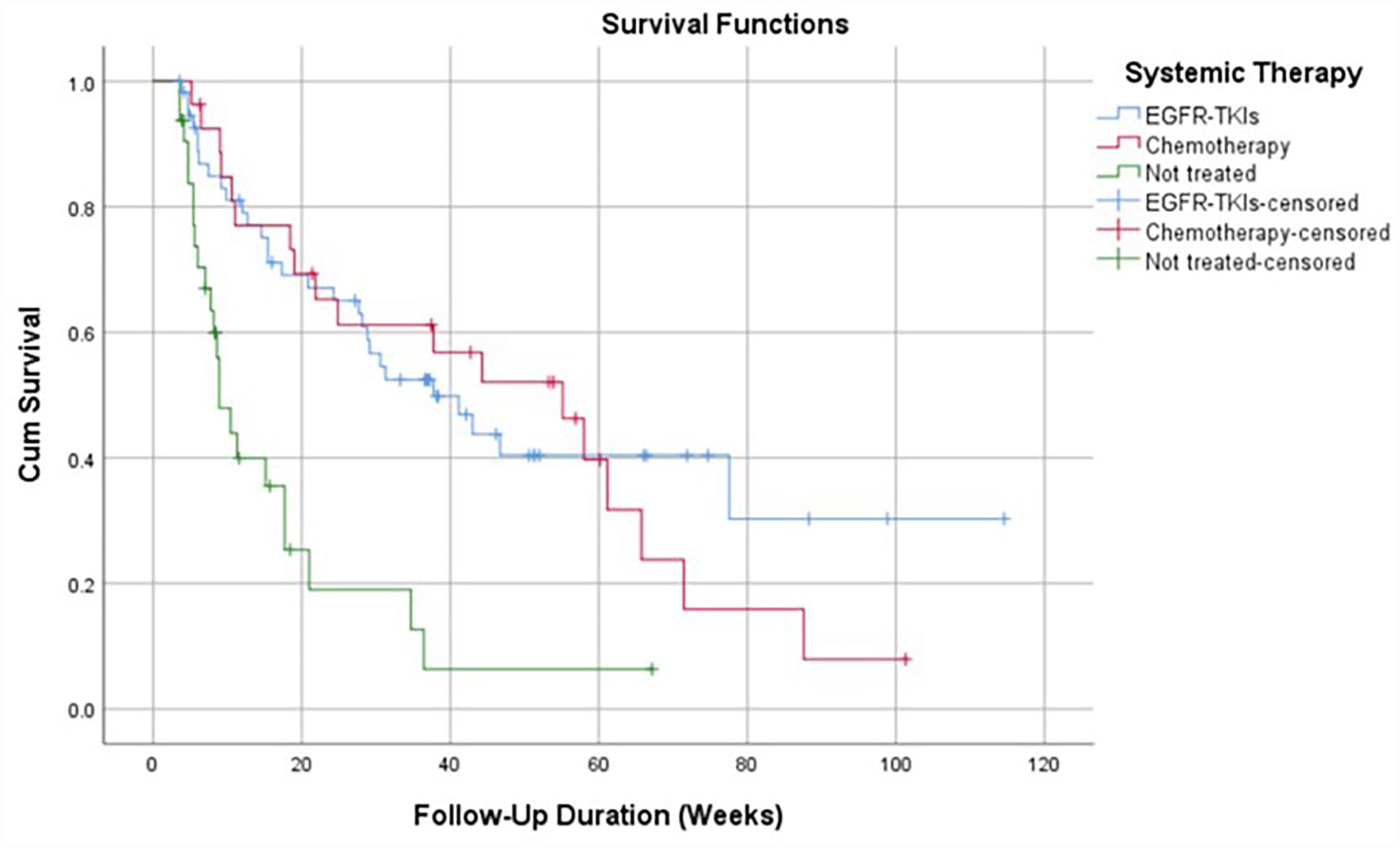
Kaplan-Meier curves for survival functions according to systemic therapy received by patients.

Kaplan-Meier curves for survival functions according to other therapies received by patients.
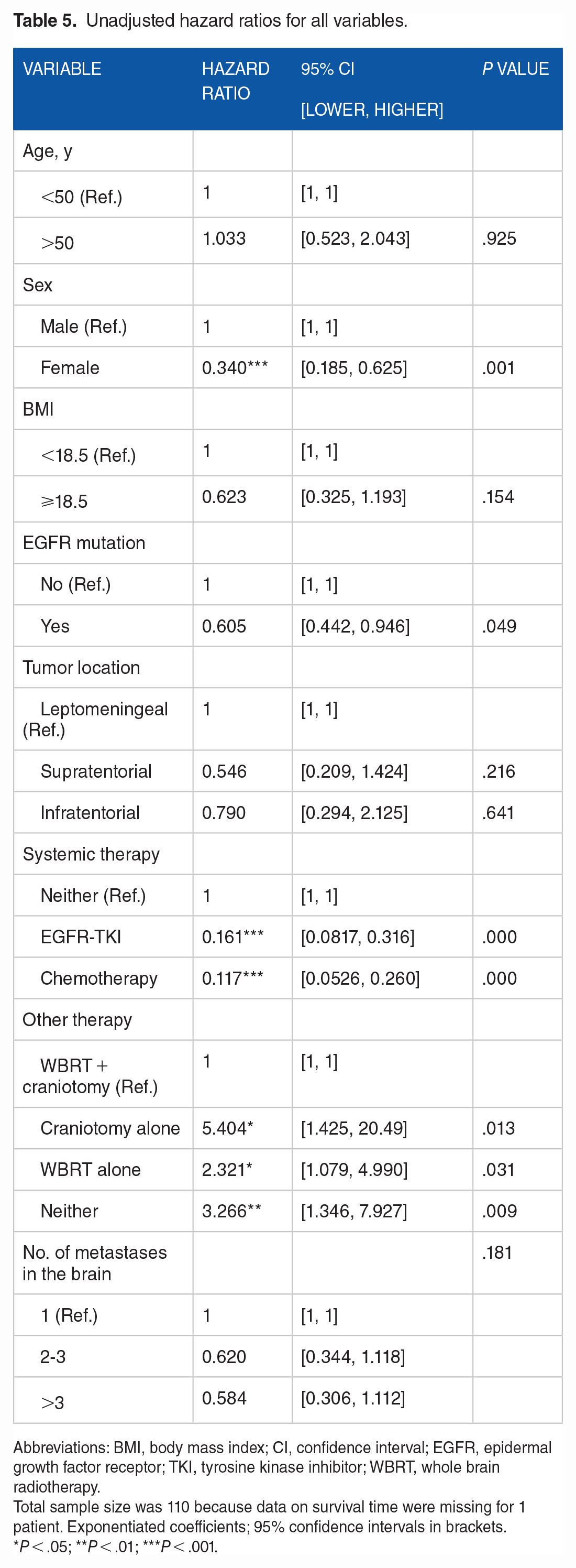
In line with the results of the log-rank test, Cox multivariate regression (Table 5) showed consistent results because it revealed that sex, systemic therapy, and other therapies were factors that significantly altered the 2-year survival rates of patients with metastatic lung cancer. Female patients and patients with EGFR mutations had a high 2-year survival rate, with a hazard ratio (HR) of 0.340 (95% CI: 0.185-0.625; P = .001) and 0.605 (95% CI: 0.442-0.946; P = .049), respectively. Patients who underwent targeted therapies, such as EGFR-TKI therapy and chemotherapy, had a higher 2-year survival rate with an HR of 0.161 (95% CI: 0.082-0.316; P = .000) and 0.117 (95% CI: 0.053-0.260; P = .000), respectively, compared with those in the untreated group. Moreover, patients who did not receive surgical intervention or radiotherapy as a combination therapy had a low survival rate (HR, 3.270; 95% CI: 1.346-7.927; P = .009).
Unadjusted hazard ratios for all variables.
Abbreviations: BMI, body mass index; CI, confidence interval; EGFR, epidermal growth factor receptor; TKI, tyrosine kinase inhibitor; WBRT, whole brain radiotherapy.
Total sample size was 110 because data on survival time were missing for 1 patient. Exponentiated coefficients; 95% confidence intervals in brackets.
P < .05; **P < .01; ***P < .001.
Discussion
Brain metastases are a common complication in several cancers but are mainly found in patients with lung cancer. Approximately 10% of patients with newly diagnosed lung cancer develop advanced-stage disease and BM.6,8 Several factors may contribute to the survival of patients with NSCLC and BM. However, in this retrospective study, we found that female patients with EGFR mutations showed better 2-year survival rates than those in male patients having wild-type EGFR. Similar results were also observed for patients who received EGFR-TKI therapy or chemotherapy and those who were treated with surgical intervention plus radiotherapy or received radiotherapy, as they showed better 2-year survival rates than the survival rates in untreated patients who received neither radiotherapy nor surgical intervention.
Evidence of the predictive value of sex for the development of BM in patients with lung cancer remains controversial. Studies by Arrieta et al 9 in 2009 and Bajard et al 10 in 2004 showed that the effect of sex on BM in patients with lung cancer remains limited. A meta-analysis of the risk factors for BM occurrence and prognosis by Shun et al 11 in 2014 revealed that sex could not predict or be used as a marker for the occurrence of BM and could not determine prognosis. Horinouchi et al 12 and Ding et al 13 found that sex may predict the occurrence of early-stage lung cancer but cannot predict its prognosis, including survival. In contrast to the existing evidence, we found that sex may alter the 2-year survival of a patient with lung cancer BM, as women showed a significantly higher survival rate when compared with that of men (HR: 0.340; 95% CI: 0.185-0.625; P = .001). This result was supported by the Kaplan-Meier curves (Figure 1). The results of a study by Gupta et al 14 in which 70% of the patients had lung cancer showed that female sex was a factor affecting the overall survival of patients with BM.
Patients with NSCLC that led to the development of BM had a higher frequency of EGFR mutations than patients without BM; conversely, among patients with NSCLC and EGFR mutations, the incidence of BM (70%) was higher than that in patients with NSCLC and wild-type EGFR (38%). 15 Studies by Matsumoto et al 16 showed that the frequency of EGFR mutations in patients with lung adenocarcinomas and BM was 63%. Although the difference in frequencies of EGFR mutations and wild-type EGFR was less, similar results were also obtained in our study, which showed that in patients with NSCLC and BM, the frequency of EGFR mutations (56%) was higher than that of wild-type EGFR (55%). In this study, the median survival time of patients with EGFR mutations was longer than that of patients with wild-type EGFR (41.8 vs 23.8 weeks, respectively; P = .0492). The values obtained in our results were much lower than those obtained by Lin et al, 17 where the median survival was 30.9 months (95% CI: 28.2-35.7 months). The reason for the results observed in the previous study was that in the study by Lin et al, 17 all types of metastases in different organs (eg, bone, adrenal, and liver) were analyzed, whereas in our study, we limited the analysis to BM only. These findings indicate that BM are more fatal than metastases to other organs.
In line with the findings of other studies, we also found that patients who were administered systemic therapy, including targeted therapy using EGFR-TKIs or chemotherapy, had a higher 2-year survival rate than those in the untreated groups18,19 with HR values of 0.161 (95% CI: 0.0817-0.316; P = .000) and 0.117 (95% CI: 0.0526-0.260; P = .000), respectively. The Kaplan-Meier curves (Figure 3) support this result. On the basis of a literature review, Myall et al 20 suggested that chemotherapeutic agents show traditionally limited intracranial activity. However, most patients with BM also have concurrent extrathoracic diseases that require systemic therapy. Chemotherapy typically forms the backbone of treatment programs for patients whose tumors lack oncogenic driver mutations. Although several studies did not show a survival benefit caused by the addition of chemotherapy to radiation therapy in patients with NSCLC that resulted in BM and limited extracranial disease, these trials primarily analyzed the effects of chemotherapy, which was administered as a concomitant regimen that is not widely used nowadays for the systemic treatment of NSCLC.21,22 However, studies on platinum-doublet chemotherapy have demonstrated good overall survival in patients who received this therapy.23,24 Pemetrexed is an antimetabolite used in combination with cisplatin or carboplatin for non-squamous cell lung cancer and has shown encouraging intracranial activity. In 2 retrospective phase III trials of metastatic NSCLC, the incidence of brain-only metastases at the time of progression was significantly lower in patients who received pemetrexed than in those who did not receive pemetrexed (3.2% vs 6.6%, respectively). 25 Considering the findings of our study and those of the existing studies, chemotherapy is still recommended for the treatment of patients with NSCLC and BM.
Other evidence suggests that EGFR-TKIs have a promising antitumor effect against BM in patients with NSCLC harboring activating EGFR mutations, and thus, EGFR-TKI therapy increases patient survival. 26 This finding is consistent with those of the present study. Gefitinib and erlotinib are the 2 most frequently used EGFR-TKIs for lung cancer management. In a recently published randomized phase II study conducted by Kim et al, 27 effects of gefitinib versus erlotinib in patients with locally advanced metastatic NSCLC following the failure of previous first-line chemotherapy were analyzed, and both drugs demonstrated comparable clinical activity with no significant difference in the response rate and the progression-free survival (PFS) and an acceptable safety profile. It would be interesting to compare the effects of gefitinib and erlotinib against BM. In the study by Kim et al, 27 no statistical differences in the objective response rates (ORRs), disease control rates (DCRs), PFS, and overall survival (OS) of the gefitinib and erlotinib groups were observed. As a result, the superior or inferior TKI regimen could not be determined.Click or tap here to enter text. Systemic therapy (chemotherapy and targeted therapy) increases the survival of patients with lung cancer and BM.
Surgical resection followed by WBRT has become the standard management practice for selected patients with solitary metachronous BM without extracranial disease. 28 However, controversies regarding an appropriate lung cancer treatment approach for synchronous BM still remain. The available evidence regarding whether craniotomy (surgical intervention) for lung cancer prolongs the overall survival of patients with lung cancer is conflicting. A study involving Taiwanese patients with lung cancer that resulted in BM showed that surgical resection of BM improved overall survival. However, these results were particularly evident in patients with large metastases. 29
Whole brain radiotherapy has been the standard approach for treating BM developed from NSCLC and remains the primary treatment modality for patients with multiple metastases. It improves symptoms with an overall response rate of 70% to 93% and provides local and distant brain control in 60% to 80% of cases. 30 Patchell et al 31 analyzed the effects of WBRT that is provided after surgical resection of BM and showed that surgical resection of BM combined with WBRT provides better results compared with those of WBRT alone in terms of local failures (20% vs 50%, respectively), median survival (40 vs 15 weeks, respectively), length of time before death from neurologic causes (62 vs 26 weeks, respectively), and length of time for which a patient remains functionally independent (38 vs 8 weeks, respectively).
These results are consistent with our findings. Surgical intervention in combination with WBRT is associated with a higher 2-year survival rate than that associated with surgical intervention or WBRT alone. Patients treated with craniotomy alone show significantly lower survival (median: 5.4 weeks; 95% CI: 4.4-4.5) than those treated with WBRT alone (median: 34.6 weeks; 95% CI: 18.3-41.8). The reason behind this observation might be that most of the surgical interventions performed in our study involved only ventriculoperitoneal shunting without tumor removal. Nevertheless, in our study, surgical intervention in combination with WBRT or WBRT alone increased patient survival rates. Patients who did not receive any of these therapies had a low 2-year survival rate, with an HR of 3.266 (95% CI: 1.346-7.927; P = .028).
To our knowledge, this is the first study conducted in Indonesia to evaluate the factors that might contribute to the survival of patients with NSCLC that resulted in BM. Our study was a single-center study and thus provides limited evidence to support our findings. We believe that additional factors might contribute to the survival of patients with lung cancer and BM. Hence, we recommend that a more detailed multicenter study on the factors affecting the survival of patients with lung cancer and BM be conducted in the future.
Conclusions
Female patients with NSCLC harboring EGFR mutations and BM had higher survival rates than male patients and patients harboring wild-type EGFR and BM. Patient survival was not affected by age, BMI, tumor location, or the number of metastases. Patients with NSCLC that resulted in BM might benefit from treatment with EGFR-TKIs, chemotherapy, and a combination of WBRT and surgical intervention.
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of staff in Dharmais National Cancer Center Hospital, Jakarta and to thank Editage for English language editing.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received financial support from the Dharmais National Cancer Center for the publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Institutional Review Board of Dharmais National Cancer Hospital, Jakarta, Indonesia (NO 096/KEPK/IV/2022). Patient confidentiality was maintained. Informed consent was not obtained because this study used secondary data and was not an interventional study.