
Abstract
Background:
Brain metastases are crucial in cancer progression, requiring focused efforts on the screening, early detection, and treatment. However, accurate forecasting the postoperative prognosis of patients with non-small cell lung cancer brain metastasis remains a challenge. This retrospective study aims to discern the factors that influence the prognosis of such patients.
Methods:
A total of 151 cases from Zhejiang Cancer Hospital were collected. Univariate analysis was conducted using Kaplan-Meier and Log-rank test, while multivariate analysis was performed using Cox proportional hazards regression model. Student’s t-test and chi-square test were employed to examine the differences between the long-term survival and the short-term survival groups. Ultimately, a predictive model was constructed using R 4.2.1.
Results:
Univariate analysis identified 12 factors as prognostic factors, showing statistical significance. In multivariate analysis, the primary contributing factors to survival were identified as age, chemotherapy of brain metastases, pathology, surgery of nonsmall cell lung cancer, targeted drugs, and GPA score. Comparing long-term and short-term groups, age, pathology, surgery of lung, targeted therapy, and radiotherapy of brain metastases were statistically differentiating factors. Based on multivariate analysis, we established a clinical predictive model predicting 2-year, 3-year, and 5-year survival rates.
Conclusion:
Younger age, receiving chemotherapy for brain metastases, adenocarcinoma pathology, lung cancer surgery, targeted therapy, and a high GPA score are associated with longer survival. This model predicts the survival period for patients with non-small cell lung cancer brain metastasis after surgery and helps in selecting more effective treatment plans.
Introduction
Brain metastases (BMs), especially non-small cell lung cancer (NSCLC), 1 frequently occur in the advanced stages of solid tumors, with a natural average survival time of 1 to 2 months.2,3 Principal treatment modalities include surgery, chemotherapy, radiotherapy, targeted therapy, and immunotherapy. 4 Surgery is usually the primary choice of treatment for patients with a limited number of intracranial lesions, total lesion volume exceeding the stereotactic radiosurgery (SRT) threshold, symptomatic mass effect or edema, or uncertain histopathological diagnosis. 5 The prognosis of such patients will significantly improve after undergoing surgical treatment. 6 Nevertheless, there is currently no effective means to accurately predict the prognosis of BMs after surgery. 7
This retrospective study aims to investigate factors influencing the prognosis of postoperative brain metastases derive from non-small cell lung cancer (POBMs-NSCLC) and to establish a predictive model to assist in survival prognosis. We aspire to provide valuable insights into the prognosis of POBMs-NSCLC, facilitating medical decision-making to extend patient survival.
Methods
Patients
In this retrospective study, 184 cases of POBMs-NSCLC from Zhejiang Cancer Hospital between 2012 and 2022 were collected. Following the inclusion and exclusion criteria (Table 1), 25 cases were lost to follow-up, 2 cases experienced fatal accidents, and 6 cases exhibited inconsistencies in lung and brain pathology. The outcome events, which serve as endpoints in this study, were recorded as either the last follow-up date or the time of death, with the final follow-up conducted on February 13, 2023. Ultimately, 151 cases met the criteria for inclusion. Within this cohort, all 151 patients received surgical treatment for BMs. Patients with 1 or 2 brain metastatic lesions underwent complete tumor resection, whereas those with more than 2 lesions had the larger tumors removed.
Eligibility criteria.

Statistical analysis
We calculated the overall survival (OS) from the date of the first diagnosis of BMs to the date of death or last follow-up. Differences between survival curves were assessed using the Log-rank test, with significance considered when the P-value was <0.05. Initially, we performed univariate analysis of prognostic factors using the Kaplan-Meier method, followed by multivariate analysis with Cox regression. Subsequently, we categorized patients with a survival period of ⩽5 months into the “short survival group” and those with a survival period of ⩾60 months into the “long survival group.” We then conducted independent sample t-tests and chi-square tests to analyze prognostic factors between the 2 groups. All data analyses were performed using SPSS software for Windows, version 25 (SPSS, Chicago, IL, USA). Finally, we developed a predictive model using R 4.2.1, incorporating independent prognostic factors, and produced relevant nomograms.
Result
Character of patients
Patient baseline characteristics are presented in Table 2. In this study, a total of 151 patients, with an average age of 61.5 years (range: 35-78), were included. Among them, 95 patients (62.91%) were aged 60 or above. There were 109 male patients (72.19%) and 42 female patients (27.81%). Nearly half of the patients exhibited concurrent brain metastases and primary lung tumors. Patients with a consistent histological type of adenocarcinoma between the lung and brain were more than twice as common as those with squamous cell carcinoma. However, 21.85% of the patients still faced challenges in definitively identifying the specific tumor type pathologically. Excluding intracranial metastases, a subset of patients was diagnosed with metastases in extracranial locations, while 107 cases (70.86%) had no definitive evidence of extracranial metastases. As of the most recent follow-up, there were 120 recorded deaths (79.47%), while 31 patients (20.53%) were still alive.
Characteristics of patients.

Character of NSCLC
Table 3 illustrates the status of primary lung tumors. Some patients had undergone examinations at other medical facilities, leading to unavailable details regarding their lung cancer. The majority of patients (86.75%) presented with a single lesion in the lung. Among those with detailed information, nearly 2-thirds had lung nodules measuring less than 4.5 cm in size. We assessed ECOG (Eastern Cooperative Oncology Group Performance Status, a scoring tool used to assess the general health status and capacity of cancer patients.) performance scores based on clinical presentations at the time of lung tumor diagnosis and found that 78.15% of patients had no severe clinical symptoms. Regarding treatment, 52 patients (34.44%) underwent surgery, 57 patients (37.75%) received chemotherapy, and 31 patients (20.53%) had lung radiation therapy. Information about targeted therapy and immunotherapy is detailed in the analysis of BMs.
Characteristics of NSCLC.

Character of BMs
All patients underwent brain surgery as part of the treatment. As indicated in Table 4, at the initial discovery of BMs, 99 cases (65.56%) presented as solitary metastases, while 25.83% had multiple metastatic lesions, exceeding 3 in number. We calculated the GPA scores for the patients at the time of diagnosing BMs and found that 32 cases (21.19%) had lower GPA scores, while 51 cases (33.77%) scored 3.5 or 4 points. In terms of treatment, 54 patients (35.76%) received adjuvant chemotherapy. Although all patients were recommended to receive radiotherapy of BMs, some chose not to pursue it due to financial constraints or other reasons. The radiotherapy included both whole brain radiation therapy (WBRT) and stereotactic radiosurgery (SRS), but the specific radiation therapy regimen for some patients was not available. Furthermore, in alignment with gene mutation status, 62 patients (41.06%) underwent targeted therapy, including first-generation agents such as Erlotinib and Gefitinib, as well as third-generation agents like Osimertinib. Meanwhile, 89 patients (58.94%) did not receive targeted treatment due to the absence of identifiable gene mutations.
Characteristics of BMs.

Survival analysis and prognostic factors
As of the last follow-up, 31 out of 151 patients (20.53%) were still alive. Within the scope of this study, among the 151 patients who underwent surgical treatment, the median OS was 16.5 months. The 1-year, 2-year, 3-year, and 5-year survival rates were 59.60%, 27.81%, 14.57%, and 6.62%, respectively.
Lower age was associated with a significantly increased survival time in univariate analysis [22 months (95% CI: 0-63.46 months) vs 20 months (95% CI: 13.37-26.63 months) vs 15 months (95% CI: 10.74-19.26 months), P = 0.018] (Figure 1A). Patients diagnosed with adenocarcinoma occupied most cases, and the median OS (22 months, 95% CI: 15.37-28.63 months) outperformed squamous carcinoma (13 months, 95% CI: 7.21-18.80 months), while squamous carcinoma surpassed group with unclear pathology (9.5 months, 95% CI: 5.28-13.72 months), P = 0.003 (Figure 1B). With smaller (P = 0.011), solitary (P = 0.021) lung cancer, patients tend to have notably longer OS. Patients with better clinical symptoms and general conditions often have higher KPS [21 months (95% CI: 13.44-28.57 months) vs 14 months (95% CI: 10.25-17.75 months) vs 4 months (95% CI: 2.40-5.60 months), P = 0.038] (Figure 1C) and GPA scores [8 months (95% CI: 6.16-9.84 months) vs 22 months (95% CI: 19.21-24.79 months) vs 14 months (95% CI: 10.25-17.76 months) vs 27 months (95% CI: 12.45-41.55 months), P = 0.000] (Figure 1D), which also indicates longer survival periods. As seen in our previous studies, interval time of NSCLC and BMs had a remarkable impact on OS [14 months (95% CI: 8.88-19.12 months) vs 16 months (95% CI: 11.16-20.84 months) vs 34 months (95% CI: 13.84-54.16 months), P = 0.044] (Figure 1E). Patients who underwent surgery for lung cancer [27 months (95% CI: 15.23-38.78 months) vs 15 months (95% CI: 11.37-18.63 months), P = 0.001] and received radiotherapy [21 months (95% CI: 17.34-24.66 months) vs 8 months (95% CI: 6.58-9.42 months), P = 0.002] or chemotherapy [24 months (95% CI: 18.75-29.25 months) vs 13 months (95% CI: 8.92-17.08 months), P = 0.027] for BMs experienced a noticeable improvement in their survival compared with patients who did not receive such treatments. Furthermore, the diameter of brain metastases also demonstrates differences in OS, even though it was not statistically significant in the multivariate analysis [22 months (95% CI: 16.64-27.36 months) vs 14 months (95% CI: 10.12-17.88 months) vs 19 months (95% CI: 10.95-27.05 months), P = 0.014]. We administered patients with gene mutations targeted therapy, and the analysis indicated that targeted treatment contributed to some extent to the extension of survival [24 months (95% CI: 14.53-33.47 months) vs 19.5 months vs 11.5 months (95% CI: 8.03-14.97 months), P = 0.004] (Figure 1F). Other significant factors can be found in Supplementary Figure.1.
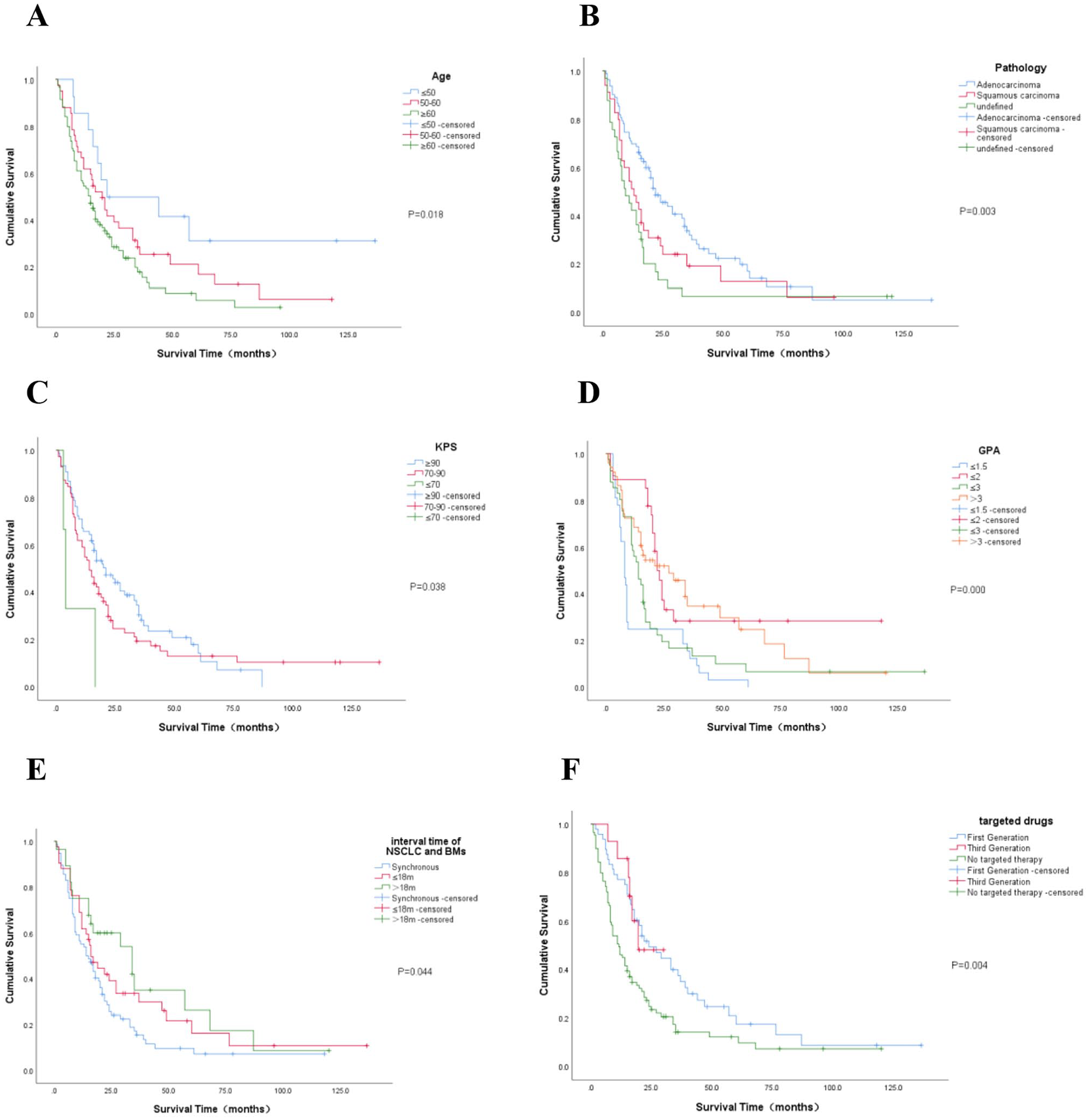
Kaplan-Meier curves are shown for age (A), pathology (B), KPA (C), GPA (D), interval time of NSCLC and BMs (E), and targeted drugs (F). P-values are calculated by Log-Rank test. The horizontal axis represents time (months), while the vertical axis represents survival rate, ranging from 0 to 1.
In a multivariate analysis of the aforementioned 12 factors, the primary contributing factors to OS were identified as age, chemotherapy for BMs, pathology, surgery of NSCLC, targeted drugs, and GPA (Table 5).
Multivariate analysis.

Short and long survival
We categorically defined 28 patients with a survival period less than 5 months as the “short-term survival group,” while the 24 patients with a survival period exceeding 60 months were designated as the “long-term survival group.” We conducted t-tests and chi-squared tests to analyze the differing factors between these 2 groups (Table 6). Similar to the aforementioned survival analysis, we found that age, pathological type, lung cancer surgery, targeted therapy, and brain metastasis radiation therapy were statistically differentiating factors.
t-tests and chi-squared tests of long-term group and short-term group.

Predictive model
Based on the 6 factors obtained above, we established a clinical predictive model and predicted the 2-year, 3-year, and 5-year survival rates for patients after lung cancer brain metastasis surgery (Figure 2). With a C-index of 0.827, it suggests that this model exhibits a strong predictive ability. Taking the 3-year calibration plot as an example, as illustrated in Figure 3. The 2-year and 5-year calibration plots are shown in Supplementary Figures 2 and 3. In this predictive model, we can observe that GPA scores have the most substantial impact on survival prediction, while the use of chemotherapy for BMs provides a relatively smaller benefit.

Predictive model for survival of POBMs-NSCLC. Based on the 6 factors derived from the multi-factor analysis above, we constructed a predictive model using the nomogram. We calculate the total score by summing up the points corresponding to the actual values of each variable for the patient. Based on this score, we can find the corresponding predicted probabilities of 2-year, 3-year, and 5-year survival in the last 3 lines.
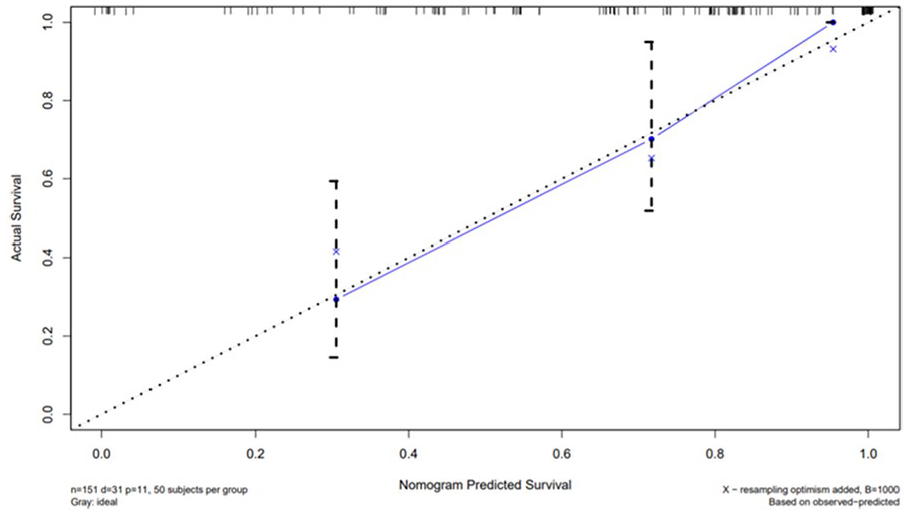
Calibration curve for the 3-year survival rate. The closer the curve is to the diagonal line, the better the performance of the prediction model is, indicating a higher consistency between the predicted probabilities and the actual occurrence probabilities.
Discussion
The NSCLC-BMs, as the most common malignant tumors in neurosurgery, exhibit a gradual increase in incidence with the growing prevalence of NSCLC. Treatment modalities such as radiotherapy, 8 immunotherapy, 9 and other palliative relief methods for terminal-stage malignant tumors have already revealed their significant roles. Although surgical treatment is not typically recommended in the terminal stages of other malignant tumors, it is often the preferred therapeutic approach for NSCLC-BMs when dealing with a limited number of intracranial lesions, total lesion volume surpassing the radiotherapy threshold, the presence of symptomatic quality of life effects or edema, or in patients with uncertain tissue pathology diagnoses.
In a retrospective analysis of a prospective database, Masillamany Sivasanker and colleagues conducted an analysis of patients after surgery of BMs. They found that the median OS of BMs patients depends on factors such as the primary tumor type, age, interval between the primary tumor and brain metastasis, and treatment regimens. 10 Considering that some primary tumor cases are relatively rare, we specifically focus on the postoperative prognosis analysis of patients with BMs from NSCLC. The high incidence and poor prognosis of NSCLC-BMs underscore its significance. Nevertheless, while surgical interventions have demonstrated favorable results, there is currently a notable absence of precise and effective methods for predicting the postoperative prognosis of individuals with brain metastases.
This retrospective study not only concentrated on analyzing the survival of POBMs-NSCLC patients but also thoroughly explored pivotal factors relevant to this specific patient group. The insights gained provide substantial information for potential development of more effective treatment strategies in the future.
This study comprehensively examined various factors affecting the prognosis of POBMs-NSCLC patients, including patient characteristics, primary lung cancer characteristics, brain metastatic cancer features, and treatment approaches. Ultimately, it was discovered that 12 factors—including age, interval time, number of NSCLC, diameter of NSCLC, pathology, surgery of NSCLC, diameter of BMs, KPS, targeted drugs, chemotherapy and radiotherapy of BMs, GPA—had an impact on prognosis and survival. Furthermore, age, pathology, surgery of NSCLC, targeted drugs, GPA, and chemotherapy of BMs turned out to be independent prognostic factors for survival. By comparing and analyzing long-term survival and short-term survival, it was evident that there were significant differences (P < 0.05) in 5 factors between the 2 groups: age, pathology, radiotherapy of BMs, targeted drugs, and surgery of NSCLC. In addition, we developed a straightforward predictive nomogram model to estimate the survival rate of POBMs-NSCLC patients.
Through our analysis, we found that age has consistently been an important factor affecting the survival of POBMs-NSCLC patients. This discovery is consistent with previous research findings, indicating that younger patients tend to have longer survival times compared with older individuals. 11 With the exception of patients with lung as the primary site, studies related to BMs in breast cancer have also confirmed a significant correlation between age and survival period. 12 Moreover, the histological type plays a crucial role. We observed that patients with adenocarcinoma generally have a longer OS compared with other types, while those with tumors that are difficult to accurately categorize under the microscope have the poorest prognosis. One year ago, in a study on BMs conducted by Gupta, it was similarly observed that patients aged 41 to 50 years and with an adenocarcinoma histological subtype experienced a longer survival period. 13 GPA, as a commonly used scoring system for assessing the prognosis of intracranial tumor patients, is primarily employed to predict the survival period of these patients. In our study, higher GPA classification was found to be related to longer survival. Numerous studies have already proved a positive correlation between GPA and survival duration. 14 Epidermal Growth Factor Receptor (EGFR) mutations not only elevate the risk of NSCLC progressing to BMs15-18 but also have an impact on the selection of treatment approaches and patient prognosis. Studies have shown that patients with EGFR mutations diagnosed with BMs often have a longer median survival period compared with those with wild-type EGFR. Specifically, patients with a 19th exon deletion mutation experienced a median survival period twice as long as those with other EGFR mutations or wild-type EGFR. 19 Likewise, research has shown that the median survival period for patients with EGFR mutations is 12.6 months, whereas for patients without EGFR mutations, it is 6.8 months (P = 0.005). 20 This is consistent with our research findings. Further grouping of patients based on the length of survival has provided additional evidence that factors such as age, pathology, and treatment are closely associated with the survival period of patients.
Research has been conducted to establish predictive models for patients with bladder cancer brain metastasis, 21 breast cancer brain metastasis, 22 and colorectal cancer brain metastasis 23 to predict the survival period of these patients. In the context of NSCLC-BMs, J.P. Agarwal and colleagues conducted survival prognosis for patients following WBRT. 24 Regarding survival prediction for post-surgery BMs patients, Hulsbergen AFC built a model to predict 6-month survival after BM resection. 25 However, there is currently a lack of relevant models for predicting long-term survival. Therefore, we established a prediction model to forecast the 2-year, 3-year, 5-year survival of POBMs-NSCLC. It is possible to infer the 2-year, 3-year, and 5-year survival probabilities for a specific patient based on known information from the graph.
However, the retrospective approach of the study comes with its own set of limitations. The limitations of this study include the small sample size, the challenges in obtaining a sufficient amount of completely accurate data in retrospective research. A significant portion of the cases occurred during a period when third-generation targeted therapies were not widely available, and treatment protocols were not standardized. In the future, large-scale prospective studies will be needed to further validate these findings.
Conclusion
Through the analysis and establishment of predictive models as mentioned above, it has been helpful to a certain extent in summarizing the characteristics, treatment, and prognosis of POBMs-NSCLC more effectively. Through this analysis, it has been observed that younger age, undergoing chemotherapy at the time of BMs, adenocarcinoma pathology, undergoing surgery for lung cancer, receiving targeted therapy, and having a higher GPA score are associated with longer OS. In the comparison between the long-term survival group and the short-term survival group, age, pathology, surgery for NSCLC, targeted therapy, and brain metastasis radiotherapy were identified as significant differentiating factors. We have proposed a novel prognostic model applicable to patients with BMs from NSCLC who undergo brain surgery. The model comprises 6 predictive factors and can be used for predicting the 2-year, 3-year, and 5-year survival rates for POBMs-NSCLC.
Supplemental Material
sj-docx-1-onc-10.1177_11795549241304532 – Supplemental material for Prognostic Factors in Postoperative Brain Metastases Derive From Non-small Cell Lung Cancer: A Retrospective Analysis
Supplemental material, sj-docx-1-onc-10.1177_11795549241304532 for Prognostic Factors in Postoperative Brain Metastases Derive From Non-small Cell Lung Cancer: A Retrospective Analysis by Haibin Chen, Liang Sun, Zhi Yang, Yuanyuan Qu, Nanyang Tong, Caixing Sun and Liang Xia in Clinical Medicine Insights: Oncology
Supplemental Material
sj-docx-2-onc-10.1177_11795549241304532 – Supplemental material for Prognostic Factors in Postoperative Brain Metastases Derive From Non-small Cell Lung Cancer: A Retrospective Analysis
Supplemental material, sj-docx-2-onc-10.1177_11795549241304532 for Prognostic Factors in Postoperative Brain Metastases Derive From Non-small Cell Lung Cancer: A Retrospective Analysis by Haibin Chen, Liang Sun, Zhi Yang, Yuanyuan Qu, Nanyang Tong, Caixing Sun and Liang Xia in Clinical Medicine Insights: Oncology
Supplemental Material
sj-docx-3-onc-10.1177_11795549241304532 – Supplemental material for Prognostic Factors in Postoperative Brain Metastases Derive From Non-small Cell Lung Cancer: A Retrospective Analysis
Supplemental material, sj-docx-3-onc-10.1177_11795549241304532 for Prognostic Factors in Postoperative Brain Metastases Derive From Non-small Cell Lung Cancer: A Retrospective Analysis by Haibin Chen, Liang Sun, Zhi Yang, Yuanyuan Qu, Nanyang Tong, Caixing Sun and Liang Xia in Clinical Medicine Insights: Oncology
Footnotes
Acknowledgements
Not applicable.
Author Contributions
Conception/design: LX, CS. Provision of study material or patients: LX, CS. Collection and/or assembly of data: HC, LS, ZY, YQ, NT. Data analysis and interpretation: HC, LS, ZY. Manuscript writing: HC. Final approval of manuscript: All authors.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was supported by the Medical Science and Technology Project of Zhejiang Province (2024KY805).
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent for Publication
Not applicable.
Data Availability
The data are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
We have obtained verbal informed consent from each participant during their medical consultation. We have also submitted the research protocol and the informed consent process to the Ethics Committee of Zhejiang Cancer Hospital and have received the corresponding approval. The approval number is [IRB-2024-272 (IIT)].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.