
Abstract
Introduction:
An essential process affecting the course of type 1 diabetes (DM1) is the appearance and duration of clinical remission. One of the most important factors promoting the occurrence of remission is physical activity, due to increased activity of antioxidants, reduces insulin resistance and improves glucose transport. Maximal oxygen capacity (VO2max) is an objective measure of the body’s aerobic capacity. To assess VO2max, oxygen uptake should be measured directly during the exercise test. The aim of the study was to evaluate the physical capacity in adults with DM1 and its relationship with the occurrence of partial clinical remission (pCR) during 2 years follow-up.
Methods:
The pCR was assessed by the following mathematical formula: A1c (%) + [4 × insulin dose (U/kg/d)]. The result ⩽9 indicates pCR. VO2max was assessed between 6th and 24th month of diabetes duration using an ergospirometer (COSMED K5 System), during an exercise test carried out on a cycloergometer (RAMP incremental exercise test).
Results:
The study group consisted of 32 adults with DM1. People with pCR were proved to have higher VO2max level [36.0 (33.0-41.5) vs 30.9 (26.5-34.4) ml/min/kg, P = .009. Univariate and multivariate regression confirmed a significant association between VO2max and presence of pCR [AOR 1.26 (1.05-1.52), P = .015]. Duration of remission was longer among group with higher VO2max results [15 (9-24) vs 9 (0-12) months, P = .043]. The positive relationship was observed between diabetes duration and VO2max (rs = 0.484, P = .005). Multivariate linear regression confirms a significant association between remission duration and VO2max (ml/min/kg) (β = 0.595, P = .002).
Conclusion:
The higher VO2max, the better chance of partial clinical remission at 2 years of DM1 and longer duration of remission.
Plain Language Summary
Introduction An essential process affecting the course of type 1 diabetes (DM1) is the appearance and duration of clinical remission. One of the most important factors promoting the occurrence of remission is physical activity, due to increased activity of antioxidants, reduces insulin resistance and improves glucose transport. Maximal oxygen capacity (VO2max) is an objective measure of the body’s aerobic capacity. To assess VO2max, oxygen uptake should be measured directly during the exercise test. The aim of the study was to evaluate the physical capacity in adults with DM1 and its relationship with the occurrence of partial clinical remission (pCR) during 2 years follow-up. Methods The pCR was assessed by the following mathematical formula: A1c (%) + [4 × insulin dose (U/kg/d)]. The result ⩽9 indicates pCR. VO2max was assessed between 6th and 24th month of diabetes duration using an ergospirometer (COSMED K5 System), during an exercise test carried out on a cycloergometer (RAMP incremental exercise test). Results The study group consisted of 32 adults with DM1. People with pCR were proved to have higher VO2max level [36.0 (33.0-41.5) vs 30.9 (26.5-34.4) ml/min/kg, P = .009. Univariate and multivariate regression confirmed a significant association between VO2max and presence of pCR [AOR 1.26 (1.05-1.52), P = .015]. Duration of remission was longer among group with higher VO2max results [15 (9-24) vs 9 (0-12) months, P = .043]. The positive relationship was observed between diabetes duration and VO2max (rs = 0.484, P = .005). Multivariate linear regression confirms a significant association between remission duration and VO2max (ml/min/kg) (β = 0.595, P = .002). Conclusions The higher VO2max, the better chance of partial clinical remission at 2 years of DM1 and longer duration of remission.
Keywords
Introduction
Type 1 diabetes mellitus (DM1) is a disorder characterized by destruction of pancreatic β cells, which leads to complete insulin deficiency. Epidemiological research on type 1 diabetes has traditionally focused on the pediatric age group, but recent data in adults has confirmed it to be a disease of all ages with a wide clinical spectrum. There are various etiological factors contributing to the expansion of its incidence on different geographical locations. 1 The life expectancy of DM1 people has increased substantially in comparison with that 3 decades ago due to the availability of exogenous insulin and new technologies, though it is still shorter than that of healthy people. 2 Adults with DM1 experience lower health-related quality of life, are more frequently unemployed and have more sick leave per year in contrast to the general population. 3
During the progression of this disease, some patients with DM1 experience a phase of remission known as honeymoon or partial clinical remission (pCR) that is mainly characterized by satisfactory glycemic control and the transient recovery of islet β cell function. 4 pCR is associated with an increase in insulin sensitivity, associated with a partial reduction in inflammation of the pancreatic islets. All these beneficial changes result in better glycemic control with reduced daily insulin requirements and are associated with a better quality of life with the disease. 5 The improved glycemic control during the pCR calls for an adjustment of the insulin regiment in order to avoid acute events. 6 The remission may be partial or complete, however even participants with complete remission need to stay on a lowered dose of insulin. The occurrence of remission ranges from 15% to 70% depending whether pediatric or adult population is observed with mean value for adults at 40%. 7 In general, the pCR phase begins 3 months after the start of insulin therapy and this phase can last from 6 to 10 months on average,7,8 but also in individual cases up to 13 years. 9 This special and important time is a good model for studying the mechanism of β cell protection, might serve as a proper intervention period for therapy, and may be related to disease prognosis. 4
There are many factors which potentially influence clinical remission, including non-modifiable (age of diagnosis, gender, occurrence of ketoacidosis) and modifiable (body mass index BMI, waist–hip ratio WHR, smoking, physical activity) factors.10 -14 Physical activity, due to increased activity of antioxidants, reduces insulin resistance and improves glucose transport, could have an influence on the prolongation of the remission period. 15 The capacity of the cardiovascular system is especially important for people with DM1 because they are twice more likely to suffer from cardiovascular disabilities than the healthy population. Studies have revealed that regular exercise is related to a decreased risk of mortality and cardiovascular disease (CVD) in patients with DM1.16,17 We also know that lower levels of cardiorespiratory fitness (CRF) are linked to an increased risk of CVD. 18 Our previous study confirmed the association between the occurrence of remission and physical activity in adults with newly diagnosed type 1 diabetes. Our data indicated that physical activity before the diagnosis may be one of the main factors determining the occurrence of remission, which may lead to the reduction diabetes-related complications. 14
It is very important to evaluate the influence of physical capacity in objective way. Most generally, physical capacity (PC) is defined as the ability of the body to undertake various types of physical exertion. Cardiorespiratory fitness and the ability of blood to bind oxygen should be considered to evaluate PC among young people. An important component of PC is reaction to changes in homeostatic processes, which is connected with symptoms of fatigue during and after physical exercises done at increasing intensity. PC is shaped by many factors (age, BMI, genes), but taking up intensive aerobic physical activity is a very important factor promoting the increase in cardiorespiratory fitness. 19 Increasing physical activity is a major mechanism by which cardiorespiratory fitness and strength can be increased. 20 McCarthy et al 21 demonstrated stable blood glucose responses to cardiopulmonary exercise testing (CPET) in people with DM1. Parameter used to describe factual PC and metabolic changes is the maximum oxygen uptake (VO2max). VO2max jointly explains the effects of the work of the cardiovascular and respiratory systems.22,23
Formerly, physical activity was not recommended for children with diabetes due to the risk of hypoglycemia. Recently, the recommendations have changed and a number of beneficial effects have been observed. 24 Gawrecki et al 25 showed that planned high intensity physical effort in men with well-controlled DM1 is metabolically safe.
To confirm hypothesis that physical activity described by an objective parameter is the most important factor which affects pCR, we created Diab1Fit Study (NCT04968171). The aim of the study was to evaluate physical capacity in adults with DM1, its relationship with the occurrence of partial clinical remission (pCR) and remission duration during 2 years follow-up. The study was to verify 2 hypotheses.
1: The greater the physical capacity defined as VO2max at the beginning of DM1, the greater the chance of remission.
2: The greater the physical capacity defined as VO2max at the beginning of DM1, the longer duration of remission.
Methodology
Study design
The study design: a observational, single-center study. The study group consisted of 32 adults with newly diagnosed DM1. Participants were recruited during 2 years (2019-2021). All participants were hospitalized at the diagnosis of diabetes and remain under the care of an outpatient clinic. The inclusion criteria were: age above 18 years old, newly diagnosed DM1—confirmed with DM1 antibodies (to glutamic acid decarboxylase—antiGAD, islet cells—ICA, islet tyrosine phosphatase 2—IA2), whereas the exclusion criteria were: CRP > 5 mg/l, unstable hypo/hyperthyroidism (TSH beyond normal range), other endocrinological disorders, contagious diseases, renal or liver diseases, confirmed COVID 19 infection, pregnancy, antineoplastic therapy in less than 2 years and any psychological or psychiatric disorder. All newly diagnosed participants were treated with intensive insulin therapy using insulin pens from the moment of diagnosis and participated in the same educational program conducted by a specially trained nurse educator, diabetologist, psychologist, and dietician. Intensive insulin therapy is defined as a treatment method requiring multiple daily insulin injections with adapting rapid-acting insulin doses before main meals, with consideration of glucose levels, desired carbohydrate intake, and planned physical activity. The subjects were informed about the purpose of the study and signed a consent form also containing the patient’s consent to the publication of the patient’s data. The study was approved by the local Ethical Committee at the Medical University of Poznan (resolution no 1050/19). We confirm that all methods were performed in accordance with the relevant guidelines and regulations. All the participants completed a standardized questionnaire including details of age, sex, chronic diseases, medicines, family history regarding diabetes and pack-years of cigarette smoking, duration of diabetes, blood glucose self-control, and medical history. Participants underwent a complete physical examination with anthropometric measurements (weight, height, waist, and hip circumference) and blood pressure check. Participants were invited to follow-up visits according to an agreed schedule. The maximum minute oxygen uptake (VO2max) was assessed between 6th and 24th month after diagnosis. We determined the contraindications to the exercise test in accordance with the latest article describing the methods of assessing physical capacity. 26 The scheme of conducting the study is shown in Figure 1.
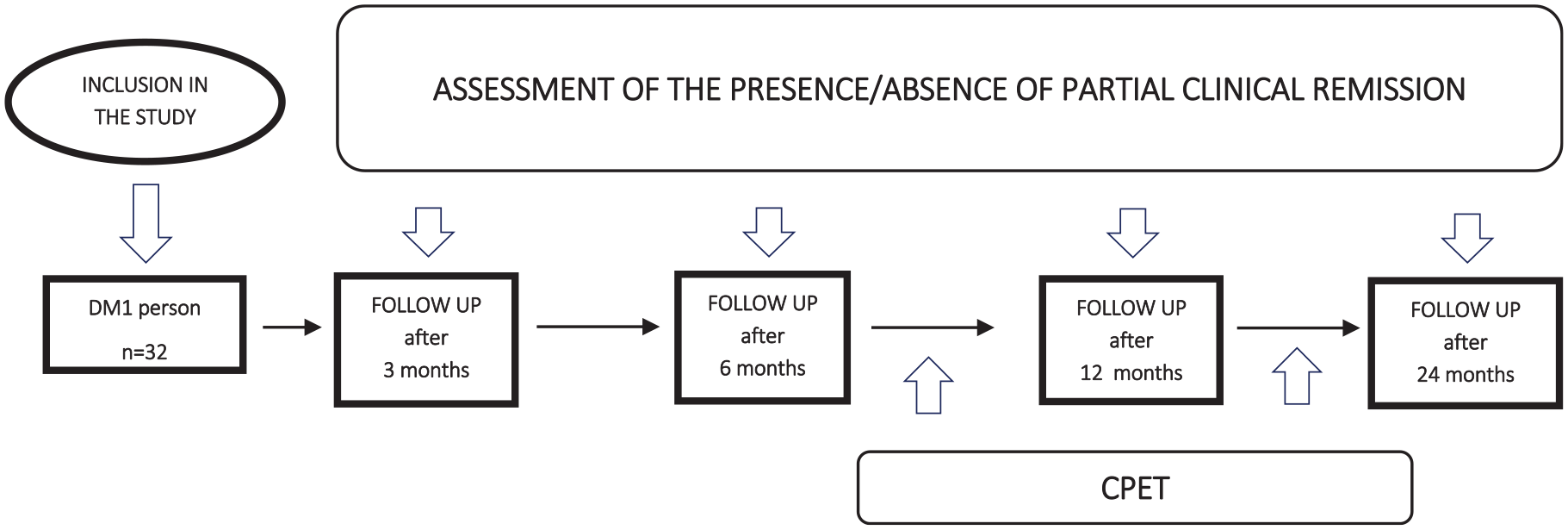
The scheme of conducting the study.
Diabetes mellitus metabolic control
A1c value was measured in whole blood and evaluated by a turbidimetric inhibition immunoassay (Cobas 6000, Roche Diagnostics). From the capillary plasma, we measured the blood glucose level before exercise, at the peak of exercise, and 5 minutes after exercise with a glucometer. A1c measurement was performed at baseline and at each follow-up visit.
Partial Clinical Remission (pCR)
The partial clinical remission was assessed by the following IDAA1c (Insulin Dose Adjusted A1c) index: A1c (%) + [4 × insulin dose (U/kg/d)]. The result ⩽9 indicates pCR. 27 The presence of remission was assessed according to the given formula at each follow-up visit. Then the number of months of pCR was summed up and used for statistical calculations.
Direct measurement of maximum oxygen uptake capacity (VO2max)—cardiopulmonary exercise testing (CPET)
This is not a routine examination, it requires specialized equipment and an experienced and trained team. The maximum minute oxygen uptake (VO2max) was assessed between 6th and 24th month of diabetes duration using an ergospirometer (COSMED K5 System), during an exercise test carried out on a cycloergometer (progressive exercise test). Using a portable spiroergometer (COSMED K5 system), an assessment of cardiovascular and respiratory capacity was made and continuous measurement of parameters (at rest, during exercise to maximum fatigue). After excluding absolute contraindications to physical effort (consultation with a diabetologist and cardiologist), each of the examined persons will perform the maximum effort (until complete fatigue and refusal to continue the effort) on the ERGOLINE cycloergometer according to the RAMP protocol, gradually increasing the load in the range from 10 to 30 W every 1 minute. The decision on the speed of the load increase was made by experienced spiroergometric testers (cardiologists) before starting the test and depended on the subjective assessment of his/her fitness and current physical activity declared by the examined person. However, none of the participants practiced competitive sports, so they all received the same study protocol. During the test, the following was monitored: fatigue (according to the 10-point BORGA scale), arterial blood pressure (RR), heart rate (HR), 12 lead ECGs, blood glucose using strip tests.
Statistical analysis
The statistical analysis was performed using the STATISTICA 13.3 program and MedCalc. The normality of distributions was tested using Kolmogorov-Smirnov’s test with Lilliefors correction. Due to lack of normality, non-parametrical tests were performed. All data are expressed as medians and IQR-interquartile range or percentage of subjects. The value of the cut-off point for pCR is 9, according to the Mortensen’s formula. In this case, the patients were divided into 2 groups, with and without pCR. The Mann-Whitney U and Chi 2 tests were used to assess differences between groups. The univariate and multivariate logistic regression, linear regression, R Spearman correlation were performed. Differences with a probability value < .05 were considered statistically significant.
Results
General characteristic
The study group consisted of 32 adults with newly diagnosed DM1. In study group we assessed 4 women (12.5%) and 28 men (87.5%), aged 27 (22.0-30.5) years and A1c 6.9 (6.1-7.5)%. Characteristic of whole group is shown in Table 1.
Characteristics of the entire study group at the time of the CPET. Data presented as median (IQR)/n(%).

Presence of partial clinical remission
People with partial clinical remission were proved to have higher VO2max level, lower glucose level before exercise and at the top of exercise (Table 2).
Comparison of group with and without partial clinical remission (pCR) at the time of the CPET. Data presented as median (IQR)/n(%).

Significant values are in bold.
Univariate and multivariate regression confirmed a significant association between VO2max and presence of partial clinical remission, independent of age, sex, BMI, and smoking (Table 3).
Univariate and multivariate regression analyses.

AOR (adjusted odds ratios) (CI confidence intervals) were calculated in a multivariate logistic regression and the P-value was calculated using the Wald test (P < .05 was assumed to be significant). The dependent variable was the presence of partial clinical remission calculated according to Mortensen’s formula. Significant values are in bold.
Continuous variable.
Duration of remission
The percentage distribution of remission duration in the study group is shown in Figure 2.

The percentage distribution of remission duration.
Data are divided into group below and above median of maximum minute oxygen uptake (VO2max) per kilogram 34.6 ml/min/kg. The results are shown in Table 4.
Comparison of group below and above median of VO2max [ml/min/kg]. Data presented as median (IQR)/n(%). General data at the time of the CPET.

The positive relationship was observed between remission duration and VO2max (rs = 0.484, P = .005) (Figure 3).

Positive relationship between remission duration and maximum minute oxygen uptake. (rs = 0.484, P = .005).
Multivariate linear regression confirms a significant association between remission duration and VO2max [ml/min/kg] (beta* = 0.595, P = .002), independent of sex, age, smoking and BMI (Table 5).
Multivariate linear regression, dependent variable: duration of remission. R = .582; R2 = 0.338; F(5.26) = 2.659; P < .045; standard error of estimation: 7.443.

Significant values are in bold.
Discussion
The study was designed to assess the physical fitness in adults with DM1 and its relationship with partial clinical remission (pCR) and subsequently duration of remission. We found that better cardiorespiratory fitness defined as VO2max promote pCR and its duration. The relationships were independent of other important factors. There is still lack of information on the impact of cardiorespiratory fitness measured by maximum minute oxygen consumption (VO2max) on the course of diabetes. Our previous study indicate that physical activity before the diagnosis may be one of the main factors determining the occurrence of remission. 14 Therefore, we continued the research using objective indicators of physical capacity in this group of people.
pCR is very important part of natural course of diabetes. It is a crucial time in the course of the disease that has short and long-term implications for the patient, such as a significant reduction in the risk of long-term complications of DM1. pCR is associated with a favorable early lipid phenotype which could translate to reduced long-term cardiovascular disease (CVD) risk in adults. 28 Occurrence of remission in adolescents and young adults with newly diagnosed DM1 is associated with better glycemic control and lower insulin requirements during the first 5 years of follow-up 29 as well as general better metabolic control. 30 Furthermore, Niedzwiecki et al 6 found that DM1 people who entered remission at the beginning of the disease, despite its ending, have higher insulin sensitivity at 7 years after diagnosis of diabetes than nonremitters.
The occurrence of remission phase is based on the immune modulation as well as β-cell rest, and rectification of hyperglycemia is likely to be the cause of this immune change. 31 Some studies show a beneficial effect of immunotherapy on the metabolic compensation of DM1. 32 Physical activity stimulates changes in inflammatory markers which may result in β-cell preservation. Along with its positive effect on insulin-stimulated glucose uptake by enhancing AMP-activated protein kinase activity, physical activity seems to be the factor that affects DM1 in many different way. Regular exercise improved physical fitness33,34 and is associated with a decreased risk of CVD. Physical activity is the main determinants of physical fitness that includes different components, such as aerobic fitness and strength35,36 which are considered important markers of health. 37 Low levels of physical activity and sedentary behavior may explain part of the risk for poor glycemic control in youth with DM1.38,39 Minnock et al compared skeletal muscle adaptations and changes in glycemic control after 12 weeks of combined resistance and aerobic training between people with type 1 diabetes and healthy controls. The training intervention increased aerobic capacity and muscle strength in both healthy and sedentary individuals with type 1 diabetes. After the intervention, improved glycemic control, reduced glycemic fluctuations, and fewer hypoglycemic episodes were noted. Their findings also showed the existence of muscle impairment in type 1 diabetes, however, a positive response to exercise indicates a mild condition, not severe myopathy. 40 Boff et al showed that high-intensity interval training is the best way to improve endothelial dysfunction and physical performance during an 8-week training period. The effect on endothelial function was associated with improved exercise capacity and was independent of changes in glycemic control. Therefore, high-intensity interval training should be recommended as a useful and safe non-pharmacological alternative for improving vascular function in DM1 people. 41 Eckstein et al 42 were able to determine a statistically significant correlation between A1c and VO2max in individuals with DM1—meta-analysis demonstrates an inverse association between physical performance and A1c showing an increase in VO2max with decreasing A1c. The newest data show that serum from non-diabetic and type 1 and type 2 diabetic individuals who underwent an 8 to 12 week program of exercise confers beta cell protection against endoplasmic reticulum stress. This shows unexpected potential to preserve beta cell health by exercise training. 43
Physical capacity (PC) is defined as the ability of the body to undertake various types of physical exertion. Cardiorespiratory fitness and the ability of blood to bind oxygen should be considered to evaluate PC. During exercise, adaptive changes occur in the internal environment of the human body, and after activity, metabolic products are removed as a result of processes related to the efficiency of the cardiorespiratory system.44,45 The parameter used to describe the actual PC and metabolic changes is maximum oxygen uptake (VO2max). VO2max explains the cardiovascular and respiratory effects. 22 This is a direct assessment method and also the most difficult to perform—it requires specialized equipment and an experienced team. Our study shows that better cardiorespiratory fitness defined as VO2max increases the chance of a partial clinical remission. The results are consistent with others showing how important physical activity is. However, our study is fully objective and excludes the influence of incorrect answers in the surveys—we decided to use the method of ergospirometry in order to objectify physical capacity.
Passanisi et al 46 showed that the mean duration of pCR is more than 12 months and age at diagnosis is the only parameter that may influence the length of pCR. The pCR duration significantly increases with age at diagnosis increasing. The effect of physical activity was not considered in this study—neither declared nor objective. ADDRESS-2 (After Diagnosis Diabetes Research Support System-2) study also confirmed that remission was most likely in anyone aged ⩾20 at diagnosis. 8 According to our results more important than age is VO2max. In the literature we found data support the view that regular physical activity may essentially contribute to extending pCR time in pediatric diabetes. However, the activity was assessed as claimed. 47 Our study clearly shows the effect of VO2max on the length of remission. This is the first study to prove the importance of physical fitness at the onset of the disease and its impact on the immediate course of remission duration.
The promotion of clinical remission is important because the occurrence of partial remission of diabetes is associated with a reduced risk of chronic microvascular complications over a 7-year follow-up. 10 Relatively low endogenous insulin secretion is associated with a reduced risk of severe hypoglycemia and microvascular complications. 48
Limitations
The study has several limitations. First, the number of patients is small. We used CPET as the sole method of assessing physical capacity. We did not use other methods of assessing the period of remission. Our results provide the basis for further studies evaluating other parameters from CPET. All this in order to better understand the mechanisms affecting clinical remission and its impact on the course of diabetes.
Conclusions
The higher VO2max, the better chance of partial clinical remission at first 2 years of type 1 diabetes and longer duration of remission. Therefore, the results presented in this study confirmed the importance of physical activity in promoting partial clinical remission and its better effects.