
Abstract
Graves’ disease (GD) is the most common cause of hyperthyroidism in children. A common GD symptom is a goiter. The usual biochemical profile in children with GD is a decreased thyroid hormone stimulating hormone (TSH) level and high free thyroxine (FT4) and free triiodothyronine (FT3) concentrations. The presence of thyroid receptor antibodies (TRAb) is the most important specific immunological sign for diagnosing GD. The treatment choices for pediatric GD are anti-thyroid drugs (ATDs), radioiodine, and thyroidectomy, but the risks and benefits of each modality are different. Management recommendations include the first-line use of a prolonged course of ATDs for at least 3 years and potentially 5 years or more. Rituximab and Teprotumumab are new novel alternative medications for the treatment of adult patients with GD and Graves’ orbitopathy respectively, but evidence of the efficacy and safety of these drugs in pediatric patients with GD is lacking.
Keywords
Introduction
Graves’ disease (GD) was first documented in 1835 by Robert James Graves, and much progress has been made in understanding this condition since then. 1 Goiter is a common symptom of GD, which is often accompanied by laboratory findings of hyperthyroidism. In youngsters, severe ophthalmopathy and dermatologic symptoms are infrequent. Furthermore, GD can also affect several organs, and the disease’s various manifestations extend beyond its local effects on the thyroid gland, showing its systemic, sympathomimetic, and autoimmune and symptoms. 2 Untreated GD has a negative influence on one’s quality of life and can lead to serious cardiovascular and psychological complications.3,4 Although laboratory diagnosis of GD is simple once the disease is detected, physicians must be mindful of the disease’s many diverse and even typical manifestations. 2
Epidemiology
GD is a rare disease in children, accounting for 1% to 5% of all cases detected in all age groups. 5 It can occur at any time during childhood, but it becomes more common with increasing age, culminating during adolescence. 6 The rate of GD in young children in Northern Europe is 0.1 per 100 000 person-years, while it is 3 per 100 000 person-years in adolescents, with a female-to-male ratio of around 5:1. 7
Pathogenesis
GD is thought to be caused by a complex interplay of genetic, environmental, and immunological variables, despite the fact that the pathophysiology remains unknown. TRAb is produced by the immune system of GD patients and binds to TSH receptors on the surface of thyroid follicular cells, causing uncontrolled thyroid activation, follicular cell proliferation, diffuse thyroid enlargement, and excessive thyroid hormone production. 8 GD can run in families, and the disease’s hereditary predisposition is assumed to be polygenic. 9 The human leukocyte antigen (HLA) region on chromosome 6p21, lymphoid protein tyrosine phosphatase (PTPN22), and cytotoxic T lymphocyte antigen 4 (CTLA-4) on chromosome 2q33, each contributing a 1.4- to 4-fold relative risk for GD.10,11 Environmental variables such as drug exposure, smoking, stressful events, infections, and high iodine exposure have all been linked to the development of GD. 12
Clinical Presentation
The majority of children with GD show characteristic pictures of hyperthyroidism, such as tachycardia, goiter, diarrhea, or increased appetite with or without losing weight. However, the symptoms of GD may develop insidiously with multisystem affections. 2 Moodiness and emotional lability, poor exercise tolerance, headache, and poor sleep can all be important symptoms of GD and are initially misinterpreted as usual problems of children and adolescents. 13 School-aged children, particularly adolescents, may be referred for evaluation of impaired concentration capacity, attention-deficit hyperactivity disorder, and poor school performance. 13 Long-term hyperthyroidism is linked to tall stature, accelerated bone maturation, and a reduction in bone mineralization.14,15 Thyroid-associated ophthalmopathy (TAO) is a common extra-thyroid clinical criterion of GD. It is an inflammatory process affecting the eye and orbital tissues with nearly one-third of pediatric GD patients may be associated with TAO. Exophthalmos is the presenting symptom, but oculomotor dysfunction is rare. However, due to excessive sympathomimetic activity, patients may have a pronounced gaze at diagnosis, which fades when the euthyroid condition is restored. 16 These symptoms can be variable with remissions and exacerbations of pediatric GD, which has a negative impact on the quality of life of affected children. 16
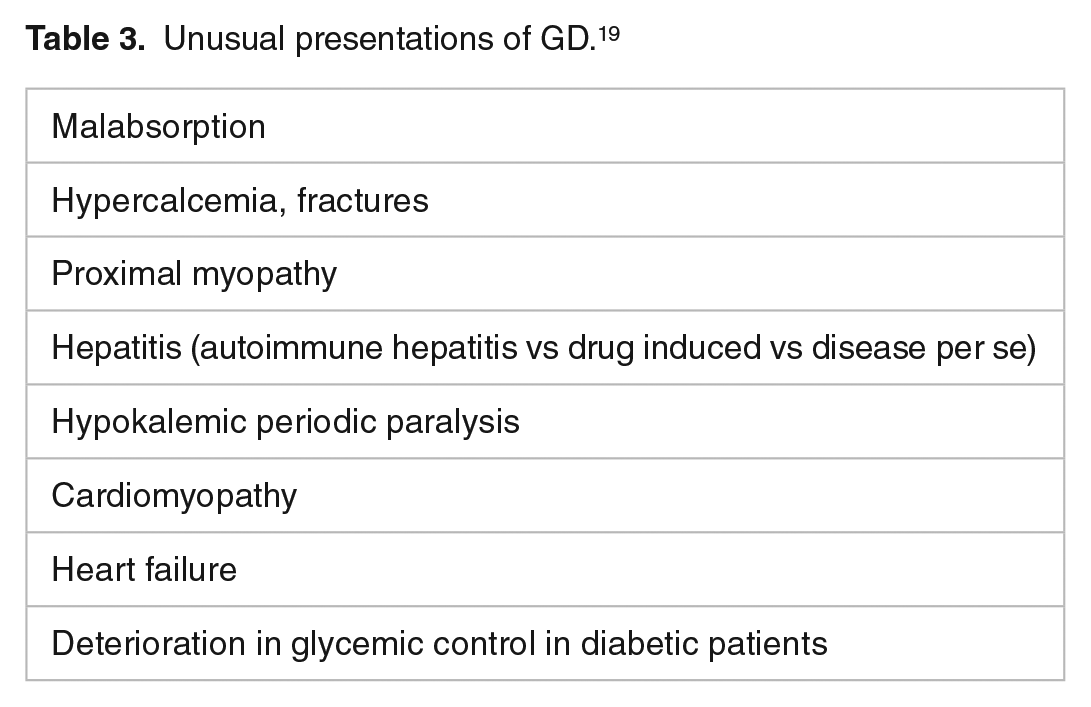
Thyroid storm or crisis is a life-threatening form of thyrotoxicosis in children, with a fatality rate of roughly 10%. The precipitating factors for thyroid storm include undiagnosed GD or previously diagnosed GD with poor compliance to ATDs and exposure to infection or surgery. Hyperthermia, significant tachycardia or tachyarrhythmias, heart failure, anxiety, gastrointestinal disturbance, hepatomegaly, respiratory distress, delirium, and seizures are the presenting symptoms and signs of thyroid storm. Rest, oxygen therapy hydration, sedation, cooling, correction of electrolyte disturbance, cardio-supportive therapy, antibiotics, and ATDs are all used to treat a patient with a thyroid crisis in an intensive care unit. 17 The detailed clinical presentation of GD in children is outlined in Table 1. 2 Identified autoimmune diseases associated with GD are outlined in Table 2. 18 Unusual presentations of GD are outlined in Table 3. 19
Clinical features of GD in children and adolescents. 2

Autoimmune disorders associated with GD. 18

Unusual presentations of GD. 19
Diagnosis
In addition to clinical characteristics, high levels of FT4and free FT3, as well as undetectable TSH levels, can all be used to diagnose GD. However, some individuals may have normal FT4 levels but high FT3 levels, a condition known as T3 toxicosis, which can be seen upon diagnosis or during relapses in the course of the disease. 2 TRAb is a sensitive, specific, and reproducible immunological biomarker for the diagnosis of GD. The TRAb test can also be used to predict the chance of relapse after treatment of ATDs. 20 Antithyroid peroxidase (TPO Ab) and antithyroglobulin (TG Ab) autoantibodies are frequently observed in children with GD and may be useful in confirming autoimmune disease. These antibodies are not specific to GD and may be detected in other autoimmune endocrine illnesses as well. 21 Thyroid ultrasonography is not required to establish the diagnosis of GD; however, it does provide a precise estimate of thyroid size, which is useful in treatment planning. It exhibits hypervascularized thyroid parenchyma that is either normal or hypoechogenic. 4 Thyroid scans are not performed on every patient. It may, however, be required in situations of GD with a negative TRAb. 22 A thyroid scan may be helpful to define the cause of hyperthyroidism in children. In GD, radioactive iodine uptake will be high and diffuse whereas, in a toxic nodule, the uptake will be focal and known as a hot nodule. Toxic multinodular goiter will have heterogeneous uptake. On the other hand, the radioactive iodine uptake in subacute or silent thyroiditis and factitious hyperthyroidism will be low. 6
Differential Diagnosis
Hashimoto’s thyroiditis (HT)
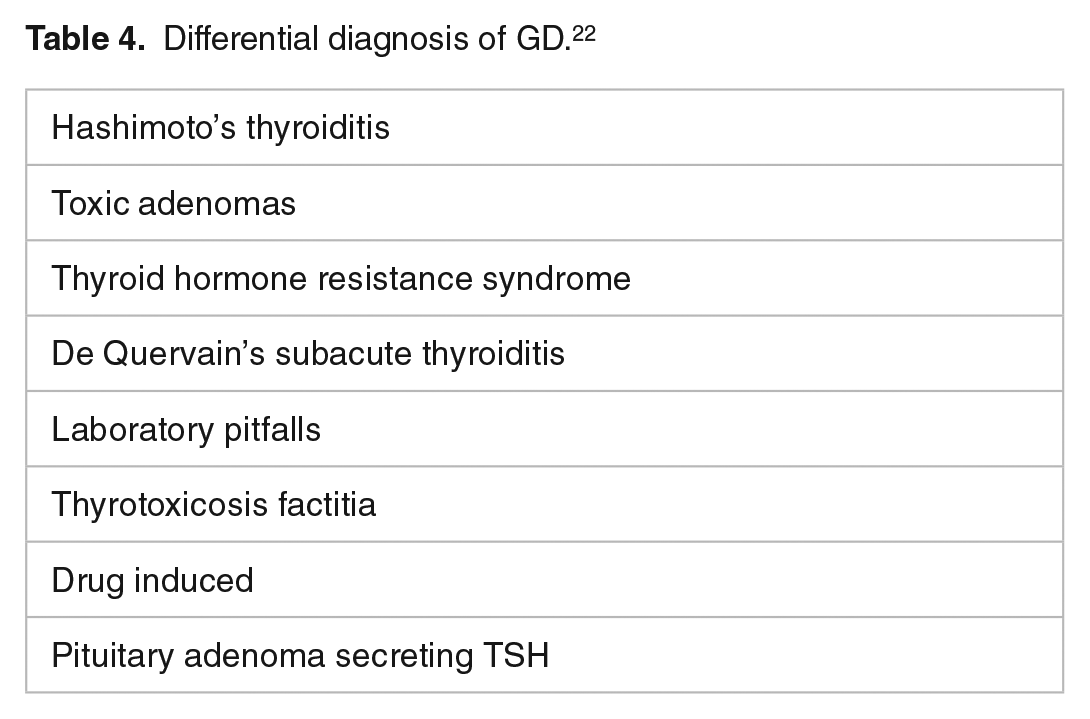
There is a strong relationship between GD and HT Table 4. 22 Hashitoxicosis is a stage in hyperthyroidism found in HT. This stage is prevalent in 5% of children with HT and can last from 1 to 6 months. The presence of TRAb is a critical feature of GD, whereas patients with HT with hyperthyroidism often have TPO Ab but not TRAb. 23
Differential diagnosis of GD. 22
Toxic adenomas
Toxic adenomas are uncommon in children; however, they can be caused by hereditary factors including somatic or germinal TSHR activating mutations 24 or McCune-Albright syndrome. 25 Thyroid ultrasound and scan can aid in the detection of toxic adenomas, which are not associated with TRAb. Surgical intervention is required for treatment. Papillary thyroid tumors have been found in 11% of children with toxic adenomas. 26
Subacute thyroiditis of De Quervain
It is uncommon in children and is characterized by a painful enlarged thyroid that often occurs after an upper respiratory tract infection, as well as elevated thyroid hormone levels and the absence of TRAb. The disease’s natural course is to resolve with no long-term consequences. 27
Laboratory pitfalls
Children treated with biotin for metabolic illnesses may have erroneous laboratory results indicating GD (low TSH, high FT4 and FT3 levels, and presence of TRAb), despite the absence of symptoms. This could be due to laboratory interference caused by the use of a streptavidin-biotin system in the assay, which leads to measurement mistakes and an erroneous diagnosis of GD in these children. 28 This problem can be resolved by repeating the laboratory tests with an alternative assay that is not based on the streptavidin-biotin system.
Thyroid hormone resistance syndrome (THRS)
THRS is a rare autosomal dominant disease caused by mutations in the thyroid hormone receptor (THR) gene. The varied clinical manifestations of THRS (hyper- or hypothyroidism) are explained by differences in tissue response to thyroid hormones. Thyroid function tests in the THRS indicate higher total and free T3 and free T4 levels in the presence of unsuppressed TSH, which can be normal or slightly raised. 29
Others
Treatment
The GD treatment policy varies considerably within and between countries and depends on, the age and preference of the patient, the size of the goiter, the severity of the disease, and local resources. The 3 therapeutic options for pediatric GD are ATDs, radioiodine (RI), and thyroidectomy. 2
Anti-Thyroid Drugs (ATDs)
In most countries, ATDs are the first choice option for the treatment of GD in children and adolescents. 4 The objective of using ATDs in the treatment of GD is to break the vicious cycle of hyperthyroidism and autoimmune aberration. Hyperthyroidism can strengthen autoimmune mechanisms that trigger increased production of TRAb, which in turn leads to more severe hyperthyroidism. Once this cycle is disrupted by ATDs medication, which renders the patient euthyroid, the condition will gradually remit. 31
Thionamides, such as carbimazole (CBZ), methimazole (MMI), and propylthiouracil (PTU) are the most common ATDs. PTU is not recommended for children because hepatotoxicity occurs more frequently in children. 4 MMI is the active metabolite of CBZ; Both drugs restrict thyroid hormone synthesis by interfering with thyroid peroxidase’s iodination of thyroglobulin tyrosine residues, and because CBZ to MMI conversion is virtually complete in the body, their effects and equal doses are assumed to be comparable. 32 It is possible that availability will decide which medicine is used. In the United Kingdom, CBZ is the most often used medication. MMI is more often used in the majority of Europe, Asia, and the United States. 33
Dosages
The beginning dose of ATD dose is between 0.15 and 0.5 mg/kg of MMI or between 0.25 and 0.75 mg/kg of CBZ daily, with a maximum dose of 30 mg/day. Both drugs are given once daily.MMI has a longer half-life and is more effective, which may aid compliance. CBM (or MMI) comes in 5 and 10 mg tablets. 30 Euthyroidism is frequently achieved within 2 to 6 weeks of starting treatment but may extend to months. 22 Thyroid function tests (FT4, FT3, and TSH) are typically monitored on a monthly basis until TSH normalization is achieved (which can take several weeks even if clinical and laboratory euthyroidism is determined by FT4 and FT3). Thyroid function tests can thereafter be done every 3 months. When normal thyroid function is maintained, medication can be gradually reduced to a minimum effective maintenance dose, which in children is usually between 5 and 15 mg/day [dose titration]. 34 Patients with signs of moderate to severe thyroid hormone excess should be started on a beta-blocker (e.g. propranolol or atenolol) in an age- or weight-appropriate dose until they are euthyroid. Patients with bronchial asthma should utilize these -blockers with caution. 4
Treatment timeframe
In children with GD, a longer treatment period is linked to a larger remission rate . Treatment duration should be at least 3 years and potentially 5 years or longer if the likelihood of remission is low based on patient characteristics at presentation. 35 Those patients who are likely to remit when ATDs are stopped will usually be on a low dose of ATDs and have no detectable TRAb. 36 Usually, TRAb declined by a median of 90% after 3 years of ATDs and ATDs should not be stopped if TRAb is high. 35 The likelihood of long-term remission if ATDs were stopped should be discussed regularly with families, and treatment cessation should not usually be in the period prior to educational milestones such as examinations. Overall estimated remission rates for ATDs therapy according to Leger et al 37 were 20%, 37%, 45%, and 49% after 4, 6, 8, and 10 years of follow-up, respectively. Another study conducted by van Lieshout et al 38 reported a remission rate of 24.1%, 31.0%, and 43.7% after treatment durations of 1.5 to 2.5, 2.5 to 5, and 5 to 6 years, respectively. Moreover, Lippe et al 34 reported a median time to remission with ATDs of 4.3 years, and the predicted remission rate was 25% every 2 years. Further, Azizi et al 39 reported a remission rate of 75% among children with GD treated with ATDs for 9 years.
Side effects of ATDs
Patients and families should be counseled about ATDs side effects. The majority of adverse effects occur in the first 3 months with a higher rate in younger children. Severe side effects may be dose-dependent Hyperthyroidism itself may be responsible for mild neutropenia or for a moderate rise in transaminases. 40
Minor side effects such as urticaria, arthralgia, and rashes occur frequently in children, in 5% to 25% of cases. These are transient side effects, with the majority of patients being able to continue treatment Agranulocytosis (even rarer: pancytopenia) complications occurring very rarely (0.2%). 41 An emergency CBC should be performed if symptoms include fever, mouth sores, or pharyngitis. If neutrophil counts are <1000/mm3, ATDs should be discontinued or decreased and may be permanently contraindicated in severe (<500) and persistent neutropenia. Otherwise, treatment may be resumed. Transaminase levels should be estimated before initiating treatment and ATDs should be stopped if the transaminase level is more than 3 times of upper limits of the normal level. Routine monitoring of liver function tests and complete blood count is not necessary since it is rare and not cost-effective. In cases of jaundice, and pruritus, measuring liver enzymes, total and conjugated bilirubin, and alkaline phosphatases is indicated.35,42
Definitive Treatment
In cases where medicinal therapy has failed, definitive treatment is either surgery (total or near-total) thyroidectomy or the use of radioactive iodine. 43 The choice of RAI or total thyroidectomy is a contentious topic and will reflect local opinion and expertise. Each pediatric case warrants multidisciplinary counseling including a thyroid surgeon, pediatric endocrinologist, and nuclear medicine physician specialized in thyroid disease; the choice of definitive treatment will involve shared decision-making with the patient and the parents, focusing on the advantages and disadvantages of each option. 35 Table 5 lists the indications for a radical treatment. 35
Indications for a definitive treatment of GD in children. 35

Surgery
The surgical treatment for GD is a total (or near-total) thyroidectomy followed by thyroid hormone replacement. General anesthesia, recurrent laryngeal nerve palsy, and transient or chronic hypoparathyroidism are dangers of surgery. 44 Most surgeons prefer to operate on a euthyroid patient with a minimally vascular gland. Daily iodide drops (e.g. a saturated solution of potassium iodide [SSKI]) for 10 to 2 weeks can be used to achieve this. 45 Individuals with recurrent hyperthyroidism after surgery may consider RI treatment because the risk of complications is higher with a second operation. 44
Radioiodine
Radioiodine (RI) has been used to treat GD for many years, the goal of RI therapy is to make the patient hypothyroid. RI is not recommended for children under the age of 5 (due to tissue sensitivity to radiation) or for large goiters weighing more than 80 g. 46 To ensure that uptake is not hampered, patients must cease using ATDs 7 days before starting RI therapy and avoid iodine-containing meals in the weeks preceding RI therapy. Patients with substantial eye illnesses should be closely monitored because their condition can worsen. Glucocorticoid cover can help alleviate this deterioration. Short-term side effects of RI (such as temporary sore throat, sialadenitis, and radiation thyroiditis) are uncommon and mainly happen following a high dose. Furthermore, thyroid function might fluctuate after RI, with periods of over and under-activity in the weeks after, necessitating periodic evaluation of thyroid status. The second dosage of RI may be required if individuals are still hyperthyroid 6 months following the first treatment. 47 The theoretical risk of secondary cancer following treatment with RI remains a matter of discussion. Observational studies in pediatric patients treated with RI aiming at hypothyroidism reported no malignancies or fertility problems with a maximum follow-up of nearly 4 decades. 35 In a study conducted by Read’s et al, 48 on 116 patients under 20 years over 36 years follow-up concluded that there was no increased risk of cancer in this population; however, they recommended studies of larger numbers of children before definitive conclusions. Moreover, Lutterman et al 49 conducted a systemic review that include twenty-3 studies evaluating 1283 children and adolescents treated with RI for GD. They reported that RI is a safe definitive treatment option for pediatric GD when aiming at complete thyroid destruction. None of the studies included in the review of Lutterman et al 49 reported non-thyroidal malignancies or leukemia later in life, despite long-term follow-up after RI treatment, up to 27 years in some studies.
New Options for Treatment
The demand for new therapeutic alternatives, combined with an increased understanding of basic immunobiology, has resulted in the development of novel treatments for adults with GD. 35 There are studies describing the clinical course of adult patients receiving biologics like rituximab or TSHR-blocking antibodies (K1-70) as a treatment for GD, however further studies are needed before deciding if these agents are of benefit in pediatric GD. 50 Moreover, teprotumumab was approved by the FDA for the treatment of thyroid-associated ophthalmopathy (TAO) in GD adult patients. Teprotumumab is a human-derived monoclonal antibody against IGF1-R effectively blocking the inflammatory responses of IGF1-R on orbital fibroblasts and providing good benefit in patients with active, moderate-to-severe TAO by reducing proptosis and improving the patient’s quality of life. 51 Indeed, more efforts are needed for the further development of teprotumumab for pediatric use.
Quality of Life (QoL)
QoL was reported to be lower in children with GD than in healthy controls, especially in the psychosocial aspect, it emphasizes the need for additional support for young people with GD, both at school and from a psychological point of view, although more studies on this area are needed. 52
Long-Term Outcome of GD
Several studies have attempted to identify predictors of remission and to define a treatment time limit beyond which remission is unlikely. Despite the fact that no single marker has been identified that provides 100% predictability. Multiple markers have been linked to a reduced risk of obtaining and maintaining remission (Table 6). 53
Predictors of remission of GD in children. 53

Conclusions
GD is the most prevalent cause of hyperthyroidism in children; symptoms can be subtle and heterogeneous, therefore a strong index of suspicion is required. TRAb is the most important immunological marker for diagnosing GD. The remission rate for children with GD who are treated with ATDs for a longer period of time is greater. Novel therapies for GD are available for adult patients with GD, although there is little evidence of their efficacy or safety in pediatric patients with GD.