
Abstract
Background
Graves disease (GD) has increased in prevalence over the past decade in Africa. Despite this, the condition is not well described, especially in sub-Saharan Africa.
Objective
We have described the clinical characteristics and associated factors of GD in a cohort of patients attending a resource-limited setting tertiary hospital.
Methods
Patients were examined thoroughly and systematically tested for the degree of clinical and biochemical thyroid status. Thyroid volume, characteristics, and blood flow were assessed at presentation using ultrasonography. Factors associated with an inability to achieve clinical and biochemical thyroid remission were evaluated using multiple logistic regression analysis.
Results
Overall, 182 patients were studied, 152 (83.5%) were women with a female:male ratio of 5.1:1.0. The mean age at presentation was 39.9 ± 14.7 years with women significantly older than men. Thyroid-associated orbitopathy (TAO) was observed in 56% of the participants and pretibial myxoedema in 6%. About 84% of the participants were hyperthyroid at presentation, 9% were euthyroid, 4% were hypothyroid, and 3% had subclinical hyperthyroidism. Inability to achieve biochemical and clinical remission at 24 months was associated with increased thyroid volume (odds ratio [OR]: 2.35, 95% confidence interval [CI]: 1.85-2.52, P < .001), presence of TAO (OR: 2.15, 95% CI: 2.12-2.33, P < .001), increased FT3/FT4 ratio (OR: 1.33, 95% CI: 1.24-2.56, P = .004), and missed clinic appointment (OR: 5.2, 95% CI: 4.55-7.89, P < .001).
Conclusions
Graves disease among Ghanaians is associated with significant signs at presentation. Inability to achieve remission within the first 24 months is associated with increased thyroid volume, TAO, an increased FT3/FT4 ratio, as well as missed clinic appointment.
Background
Graves disease (GD) is an autoimmune disorder in which activating autoantibodies directed against thyrotropin (TSH) receptor result in the continuous stimulation of thyroid hormone production and release as well as thyroid growth.1,2 The clinical manifestation, although diverse, principally involves hyperthyroidism, ophthalmopathy, and diffuse goitre. 3 Organs other than the thyroid gland may be affected, leading to extrathyroidal manifestations of GD, mainly Graves-associated orbitopathy, observed in ~50% of patients, 4 Graves dermopathy and acropachy, both rare.5,6 Graves disease is believed to result from a complex interaction between genetic susceptibility (such as polymorphisms in various genes including HLA-DR, CTLA-4, CD45, PTPN22, and TSH-R) which constitute 70% of the attributable risk for the disease and environmental factors (including stress, pregnancy, smoking, selenium deficiency, several drugs, irradiation, infections, allergy, and immune reconstitution).7–9
The prevalence of GD is higher in areas of iodine sufficiency constituting over 80% of hyperthyroid cases. 10 The disease peaks in the fourth decade of life, with a significant female bias, up to 10:1 ratio.11–19
Previous studies on the disease have revealed differing patterns regarding characteristics on deferent continents. 20 This study aims to bridge the gap in knowledge on the peculiarity of the disease in Ghana by describing the demography and clinical characteristics of a cohort of 182 patients with GD seen at a tertiary referral centre in the middle belt of Ghana.
Materials and Methods
Participant recruitment
This is a cohort study involving patients enrolled for follow-up visit to the endocrine clinic of Komfo Anokye Teaching Hospital who fulfilled the criteria for the diagnosis of GD (the combination of eye signs, goitre, and any of the characteristic symptoms and signs of hyperthyroidism). These patients were enrolled after standard history, and clinical examination had been performed with a focus on verifying their thyroid status and diagnosing GD. A brief questionnaire on previous thyroid disease; autoimmune thyroid disorders; intake of medications, including amiodarone and nutritional supplements; smoking and alcohol intake habits; accompanying conditions; and family history of thyroid disease was filled out. Smokers were identified by self-report as those who had smoked at least 10 sticks of cigarette per day for 6 months or more or those who smoked daily for 1 year or more regardless of the number of cigarettes smoked per day. 21 Positive alcohol intake status was identified when greater than 14 units of alcohol were consumed per week in the case of a woman and 21 units per week in case of a man. 22 We scanned through folders to identify follow-up visits to ascertain the duration of follow-up visits.
Physical examination
Complete physical examination including body weight and height measurements was taken in duplicates using a combined manual scale and stadiometer (Asimed MB 211 T plus Aparatos Y Sistemas de Medida). Body mass index was calculated as weight in kilogram divided by the square of height in metres (kg/m2). 23 Blood pressure was determined using a manual mercury sphygmomanometer. Hypertension was defined as mean blood pressure ≥140/90 mm Hg and documented antihypertensive therapy. 24 Pulse rate was determined at the radial artery and classified as tachycardia if pulse rate was higher than 100 beats per minute. 25 Ophthalmologic examination was done with the aim of assessing for lid lag, lid retraction, chemosis, exophthalmos, and various manifestations of thyroid-associated orbitopathy (TAO). Thyroid-associated orbitopathy was assessed using the European Group of Graves’ Orbitopathy (EUGOGO) classification that uses various indicators to assess the signs and symptoms of activity and the degree of severity.
Thyroid ultrasonography
Thyroid ultrasonography was performed with the measurement of thyroid volume in millilitre, characteristics, assessment for nodules, and confirmation of high blood flow using Doppler measurements. Thyroid volume was estimated via ultrasonography using a 7.5-MHz linear array transducer (GE Healthcare Bio-Systems, Milwaukee, WI, USA). All examinations were performed and interpreted by the same experienced radiologist. Thyroid volumes were calculated using the volumes of both lobes as follows: lobe (mL) = length × width × depth (mm) × 0.479. Nodules and cystic areas were included in the thyroid volume (reference values: women: 18 mL; men: 25 mL). Parameters for colour Doppler were F. 6.6 MHz, G. 64%, PRF 5.6 KHz, and WF 50 Hz. The angle correction cursor was parallel to the direction of flow, and the Doppler angle was kept at or below 60°. The peak systolic velocity, end diastolic velocity, and mean velocity were obtained. Peak systolic velocity of the inferior thyroid artery of 40 cm/s was considered significantly high and suggestive of GD. Thyroid volume values were obtained by calculating the volumes of both lobes as follows: Lobe (mL) = length × width × depth (mm) × 0.479. Nodules and/or cystic areas were included in the thyroid volume (reference values: women: 18 mL; men: 25 mL).
Laboratory measurements
Approximately, 10 mL of fasting venous samples was collected from each participant into Vacutainer tubes (Becton Dickinson, Rutherford, NJ, USA) and Sequestrene bottles. Samples were manually processed and cryopreserved before transporting to the laboratory for analysis. Samples were aliquoted for measurement of serum-free thyroxine (FT4), free triiodothyronine (FT3), TSH, TSH receptor antibody (TRAb), thyroid peroxidase antibodies (TPOAbs), thyroglobulin antibodies (TGAbs), kidney function tests, and haematological parameters. The TRAb was measured using a receptor assay (DYNOtest TRAK, Thermo Fisher, Berlin, Germany). TPOAb, TGAb, serum FT4, FT3, and TSH were all measured (Cobas e 411 automated immunoassay analyzer; Roche Diagnostics, Indianapolis, IN, USA). The reference range, intra-assay, and inter-assay coefficients of variation for thyroid hormones and antibodies were as follows: TSH: O.25-4.2 IU/mL, <2.2% and <2.3%; FT3: 3.7-10.4 pmol/L, 4.8% and 5.9%; FT4: 7.5-21.1 pmol/L, 2.8%; TPOAb >5.6 U/L, 3.1% and 2.4%; TPOAb >5.6 U/L, 2.1% and 6.1%; TGAb >4.1 U/L, 1.9% and 5.6%; TRAb >3.4 IU, 1.2% and 1.9%, respectively.
Thyroid function was classified as euthyroidism when FT4, FT3, and TSH were within the normal range; hypothyroidism when TSH level was higher than the upper limit of the reference range and FT4 or FT3 is lower than the lower limit of their reference ranges; subclinical hypothyroidism when TSH is greater than the upper limit of the reference range and FT4 and FT3 are within the normal range; hyperthyroidism when TSH level is lower than the upper limit of the reference range and FT4 or FT3 is greater than the upper limit of their reference ranges; subclinical hyperthyroidism when TSH level is below the lower limit of the reference range and FT3 and FT4 are within the normal range.
Ethical approval and consent to participate
The study was approved by the Committee for Human Research Publications and Ethics at the School of Medical Sciences, Kwame Nkrumah University of Science and Technology, and the Komfo Anokye Teaching Hospital, Kumasi. All participants gave an informed consent with those unable to understand or sign the consent excluded.
Statistical analysis
Data were analysed using GraphPad Prism 7 software for Mac OS X and presented as mean (standard deviation), median (interquartile range [IQR]) and n (%), respectively. Data normality assumption was performed by visual inspection of distribution as well as D’Agostino and Pearson Omnibus normality test. Statistical difference between means, medians, and proportions was assessed using Student t tests, Mann-Whitney U tests, and χ2 tests, respectively. Predictors of inability to achieve remission at 24 months after drug therapy were evaluated using multiple logistic regression analysis. Differences were considered statistically significant at P < .05.
Results
Sociodemographic and clinical characteristics of participants
As shown in Table 1, 182 participants were involved in the study, 152 (83.5%) were women with a female:male ratio of 5.1:1.0. The mean age at presentation was 39.9 ± 14.7 years, with men relatively younger than women. Two distinctive peak age ranges at presentation were identified, ie, the 30s and the 50s age groups (Figure 1). About 13 (7.14%) of the participants reported a history of other autoimmune disorders, with the proportion of women significantly higher than men. About 38 (20.9%) presented with a history of thyroid disorder, with women significantly higher than men. Men were relatively heavier than women. The mean pulse rate at presentation was 87.5 ± 20.6 with no significant sex difference. The mean systolic blood pressure and diastolic blood pressure showed no sex differences. In all, 42.9% of the participants had hypertension at the time of diagnosis. As shown in Figure 2, the most prevalent symptoms of participants at presentation were palpitation (86%), goitre (77%), and shortness of breath (77%). Regarding clinical signs, the most frequent presentation was goitre (85%), lig lag or lig retraction or both (79%), and tachycardia (75%) (Figure 3). The mean volume of the thyroid gland at presentation was 45.0 ± 1.8 mL with no sex difference.
Sociodemographic and clinical characteristics of patients with Graves disease in Kumasi.


Age range at presentation for participants.

Symptoms associated with Graves disease in Central Ghana.

Clinical presentation of patients with Graves disease in Central Ghana.
Laboratory results of participants
As shown in Table 2, the white cell count of participants showed no significant sex difference. The mean haemoglobin and urea levels did not show any sex difference. The creatinine levels of men were significantly higher than in women.
Laboratory results of Graves disease patients in Kumasi.
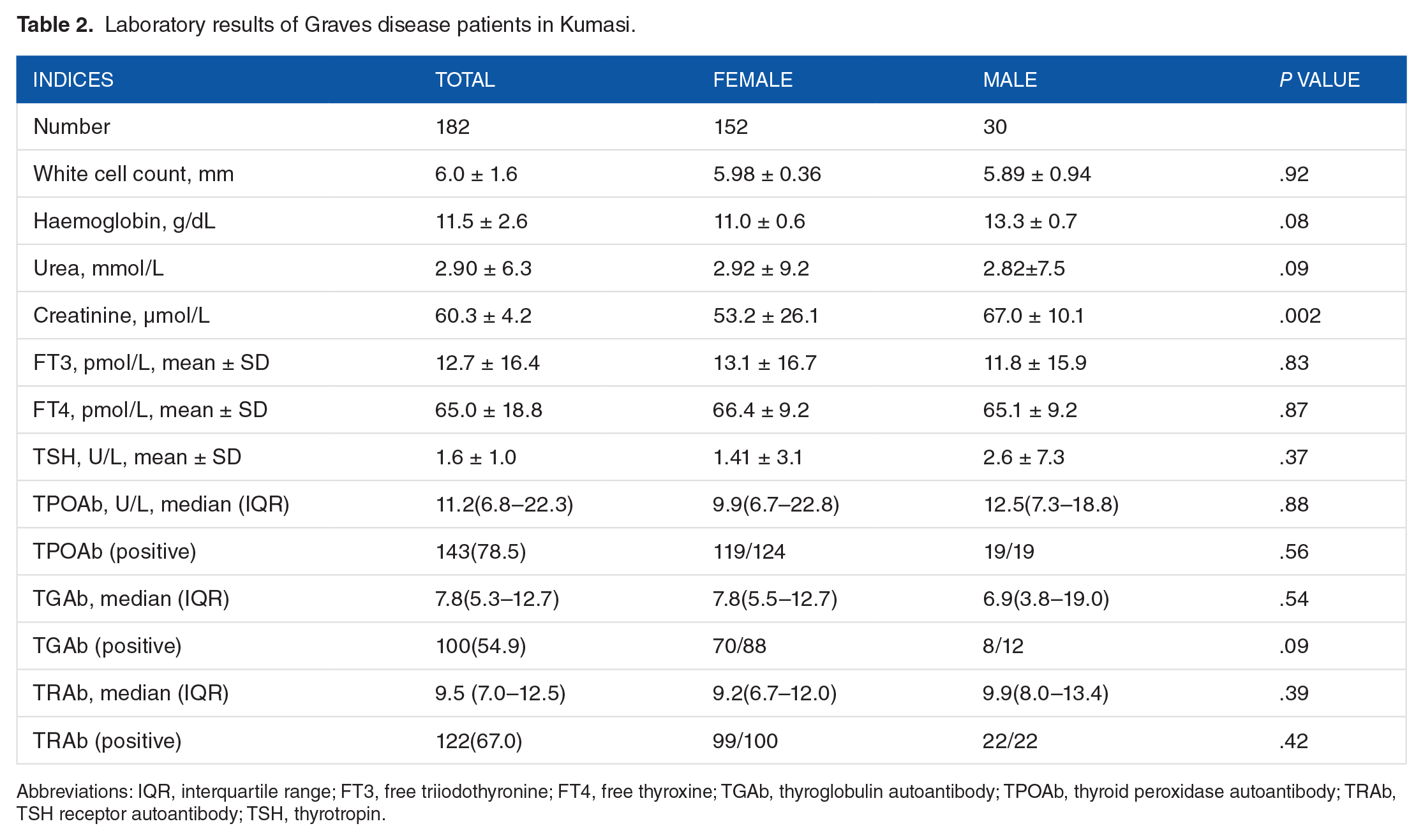
Abbreviations: IQR, interquartile range; FT3, free triiodothyronine; FT4, free thyroxine; TGAb, thyroglobulin autoantibody; TPOAb, thyroid peroxidase autoantibody; TRAb, TSH receptor autoantibody; TSH, thyrotropin.
Thyroid function at presentation
The mean FT3, FT4, and TSH showed no sex difference. The median (IQR) TPOAb level was 11.2 (6.8-22.3) with no significant sex difference. The levels were only tested in 143 (78.5%) of the participants with 96.0% of women testing positive and 100% men testing positive. Thyroglobulin autoantibody was tested in 100 (54.9%) of participants, 70 (79.5%) of women tested positive, and 8 (66.6%) of men tested positive. Thyrotropin receptor autoantibody was tested in 132 (67.0%) of participants. About 99% of women and 100% of men tested positive for TRAb. About 84% of the participants were hyperthyroid at presentation, 9% were euthyroid, 4% had hypothyroidism, and 3% had subclinical hyperthyroidism (Figure 4).

Clinical status of participants at presentation.
Predictors of inability to achieve remission
The results of multiple regression analysis are as shown in Table 3: the presence of thyroid orbitopathy was associated with 2× increased odds of inability to achieve remission at 24 months. Again, each millilitre increase in thyroid volume was associated with 2.32× increased risk of an inability to achieve remission at 24 weeks. Each missed appointment was associated with 50% increased odds of lack of remission at 24 months.
Predictors of inability to achieve remission.

Abbreviations: CI, confidence interval; OR, odds ratio.
Discussion
This is the first study describing the clinical characteristics of patients with GD in Ghana. This study although showing a significant predilection of GD among women compared with men, with a ratio of 5.1:1.0, the sex difference does not quite reach levels seen in Europe and Americas where levels as high as 10:1 have been shown.11,26 There appears a lower female:male ratio among blacks, as a similar study involving patients with GD in Senegal yielded only slightly higher ratio compared with this study. 27 In general, the increased association of GD with the female sex and, in particular, its rarity before puberty and after menopause strongly implicates the role of sex steroids in its causation. 19 Again, the protective role of androgens in the development of autoimmune thyroid disease provides an additional layer of evidence to the role played by female sex hormones in the determination of GD. 28 Female sex hormones, in addition to exerting a strong influence on the immune system and determination of the B-cell repertoire, also favour TH2 T cells and antigen presentation.28,29 Androgens may also actually suppress autoimmune thyroid disease and favour TH1 T cells and CD8+ T cells. However, the fact that the prevalence of the disease does not decline during menopause and a high number of men still develop the disease has brought the influence of X chromosome–related disease. Women with their 2 chromosomes receive twice the susceptibility gene. Evidence of X chromosome–linked disease has been implicated in GD.
The mean age of participants with GD of 39.9 ± 14.7 is slightly higher than seen in other studies. 27 However, the 2 peak age ranges at diagnosis in the 30s and 50s shown in our patients with GD are similar to that seen in other studies.7,27 Overall, the presentation of GD in our setting was largely due to goitre and cardiovascular symptoms as well as hypermetabolic manifestations as those found in other areas of the world, with a few atypical presentations. 30 Also, clinical signs were dominated by cardiovascular and ophthalmologic complications. In all, the clinical presentation of GD as seen in this study bodes well for an area like Ghana where the diagnosis of GD is usually based on clinical signs, often with limited laboratory support and non-existent radioisotope investigation available. Although clinical diagnosis of GD can be made based on signs and symptoms, detailed investigations are needed to plan treatment. Although not routinely tested for in the clinical setting, most participants tested for various thyroid antibodies outlined the utility of thyroid autoantibodies, in that almost all participants who were tested were found to be positive for TRAb as well as TPOAb. This also underlines the autoimmune basis for this disorder. Thyrotropin receptor autoantibody showed the highest sensitivity and specificity for diagnosing the disease.31,32 The increasing sensitivity of TRAb is mainly because of its destructive role in the pathophysiological mechanism involved in the disease. 11
A significant proportion (84%) of patients were hyperthyroid at presentation, highlighting the disease as mainly a hyperthyroid disease state. 33 However, a few of the patients presented with other biochemical thyroid states including euthyroidism. Although this in some instances will confound the diagnosis especially when there is no thyroid imaging available as in our case, it must be highlighted that the disease can sometimes present with various biochemical states including subclinical states. 34 A broad spectrum of biochemical presentation, therefore, exists in these patients. The presence of distinct clinical signs in most of these patients such as Graves orbitopathy with the addition of highly sensitive TRAb assays makes the diagnosis almost always straightforward.
Almost all the patients with hyperthyroidism were started with antithyroid drugs as well as β-blockers, specifically carbimazole with an average time to remission of 8 months. However, a significant proportion of patients could not achieve remission at 24 months. As determined by logistic regression, these patients had a significant association with TAO. This can be explained by the fact that the presence of TAO can sometimes indicate an increased activity of GD often leading to an increased risk of lack of remission especially with other factors at play. 1 An inability to achieve early remission in this cohort of patients was also associated with an increased thyroid volume at presentation similar to that observed in other studies.35,36 An increase in thyroid volume at presentation also signifies increase in the activity of thyroid gland through increase in the stimulation of TSH receptors by TRAb. 36 Additional factors associated with an inability to achieve remission at 24 months in our study cohort included patients with a relatively high FT3/FT4 ratio.27,37 The FT3/FT4 has also been an indicator of thyroid activity. 38 Patients with GD who routinely missed clinic appointments were 5× associated with the inability to achieve remission. 39
This study is limited by the inability of all the participants to undergo thyroid autoantibody testing in the research and the limited number of participants. However, this study has been able to underline the factors associated with an inability to achieve remission in this low-resource setting. In addition, this study provides a useful update on the need for the acquisition of nuclear medicine set-up to provide a useful option for diagnosis and drug therapy for patients. Also, patients with these peculiar characteristics provide a valuable index for stringent treatment and counselling for patients.
Conclusions
In conclusion, GD was seen in a ratio of 5:1 in patients in Ghanaians with a bimodal age of presentation in the 30s and 50s. Inability to achieve remission at 24 months was associated with an increased in thyroid volume at presentation, increased FT3:FT4 ratio, missed clinic appointments, and TAO.
Footnotes
Funding:
O.S-K. funded this study.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
OS-K conceived the study, participated in its design, and drafted the manuscript. FSS contributed to study design, coordinated data collection, and helped with statistical analysis. EOA assisted in conducting the field activities. IK contributed to the study design and manuscript development. OS-K, FSS, EOA, and IK conceived and designed the experiments; wrote the paper; and read and approved the final manuscript. OS-K, EOA, and IK performed the experiments. OS-K and FSS analysed the data. OS-K, FSS, and IK contributed to reagents/materials/analysis tools.
Consent for Publication
All participants in this study consented to information obtained from them for this study to be published.
Ethical Approval and Consent to Participate
The study was approved by the Committee for Human Research Publications and Ethics at the School of Medical Sciences, Kwame Nkrumah University of Science and Technology, and the Komfo Anokye Teaching Hospital, Kumasi. All participants gave an informed consent with those unable to understand or sign the informed consent excluded.