
Abstract
Spontaneous pneumomediastinum (SPM) is the presence of air in the mediastinal interstices in the absence of any surgical or medical procedure, chest trauma, or mechanical ventilation. SPM can occur during vigorous Valsalva maneuvers, such as weight lifting, coughing fits, hyperemesis gravidarum, and so on, or during inhalation of illicit substances or toxic agents, as a result of an abrupt increase in pressure in the tracheal tree. Preexisting underlying lung disease may be a contributing factor. In the present case, we report for the first time an SPM due to accidental overexposure to paint thinner in a 15-year-old male from a low-income rural family. He was offered a job painting the inside of a house, which he accepted to earn some money for the family household. However, due to his inexperience, he overdosed on a can of paint with thinner. About 2 h after starting work, he began to feel increasingly severe chest pain and had to be rushed to the local level one basic hospital by his parents. Physical examination revealed subcutaneous emphysema over the supraclavicular area and crackles in the precordial area. Chest radiographs showed a pneumomediastinum. In retrospect, the patient denied coughing or sneezing attacks after exposure. He was transferred to a regional tertiary hospital for further diagnostic evaluation to rule out airway/esophageal perforation. Chest computed tomography confirmed underlying SPM and subcutaneous emphysema. The oesophagogram and bronchoscopy were unremarkable. SPM, possibly secondary to overexposure to thinner vapors, a hydrocarbon-based compound, was the final diagnosis. The patient was discharged asymptomatic on day 5.
Keywords
Introduction
Spontaneous pneumomediastinum (SPM) is defined as the presence of air in the mediastinal interstices in the absence of any surgical or medical procedure, chest trauma, or mechanical ventilation. 1 The first series of cases of SPM was reported in 1939 by Haman. 2 Years later, in 1944, a pathophysiological explanation for what has since been referred to as Maklin's effect was provided by Macklin and Macklin. 3 According to these authors, centripetal alveolar air infiltration along the connective tissue sheath surrounding the great vessels and bronchi into the mediastinal space would occur upon rupture of the marginal alveoli due to a sudden increase in intrathoracic pressure (ie, Valsalva maneuver or mechanical ventilation). Air infiltration may reach more distant anatomical sites, causing periorbital emphysema 4 or epidural pneumatosis. 5 SPM may occasionally be associated with pneumothorax. 6
A variety of etiological factors, ranging from weightlifting 7 to hyperemesis gravidarum, 8 can cause a sudden increase in intrathoracic pressure, leading to SPM. Similarly, various underlying pulmonary conditions have been identified as predisposing to alveolar rupture, either of infectious origin, such as Pneumocystis jirovecii pneumonia 9 with or without HIV infection or COVID-19 pneumonitis, 10 or of noninfectious origin. The latter subset comprises bronchial asthma, 11 pneumoconiosis, 12 or lung involvement accompanying dermatomyositis. 13
More recently, the inhalation of toxicants 14 and illicit substances 15 has been increasingly identified as a cause of SPM. There is a growing list of chemical agents that are recognized as being capable of producing SPM. In the present case, we have included a new one in the list. We report, for the first time, the development of SPM after a brief acute overexposure to paint thinner in a 15-year-old adolescent. This case is relevant because paint thinners are widely used in painting. This report aimed to draw the attention of primary care physicians and specialists to this diagnostic possibility in patients exposed to this hydrocarbon compound.
Case Report
A 15-year-old boy was referred from Sucúa Hospital, Morona Santiago Province, to Vicente Corral Moscoso Hospital, Cuenca City, Ecuador with retrosternal pain associated with subcutaneous emphysema in the right supraclavicular region. The patient was the eldest son in a low-income rural family and, according to his parents, was offered a job painting a house interior, which he accepted as an opportunity to earn money. He was inexperienced and apparently added an excessive amount of diluent to the paint. Approximately 2 h after starting to paint, the patient began to feel increasing retrosternal chest pain to the point that he left the job site and returned home. His parents rushed him to a local hospital. The patient had a hyposthenic body habit and no history of preexisting respiratory diseases, such as bronchial asthma or recurrent respiratory infections, and was in good general health. The patient was evaluated in the emergency room. He denied any coughing or sneezing attacks. No signs of respiratory distress were observed, except for chest pain. The patient was afebrile and had normal oxygen saturation as measured using a pulse oximeter. Physical examination revealed subcutaneous emphysema in both supraclavicular regions. Normal vesicular breath sounds were observed in both lung fields. Precordial crackles could be heard over the precordium synchronous with the heartbeat (Hamman's sign). Chest radiography revealed a pneumomediastinum (Figure 1). The patient was then transferred to a level-3 specialty hospital, where he was admitted for further evaluation and follow-up. Chest computed tomography (CT) confirmed the findings of the chest radiography (Figure 2). No contrast extravasation from the esophageal lumen or stomach was observed on esophagography. Endoscopy revealed no mucosal lesions in the esophagus or stomach. No foreign bodies were noted. Spontaneous SPM was diagnosed, possibly due to overexposure to paint solvents. The patient was maintained on NPO (the Latin abbreviation of “Nil per os” [Nothing by mouth]) with continuous oxygen, broad-spectrum antibiotics, and nonsteroidal anti-inflammatory drugs for the first 3 days. His evolution was favorable, with complete resolution of the pneumomediastinum over the next 3 days, along with remission of chest pain and findings on heart auscultation. The patient was discharged asymptomatic on day 5.
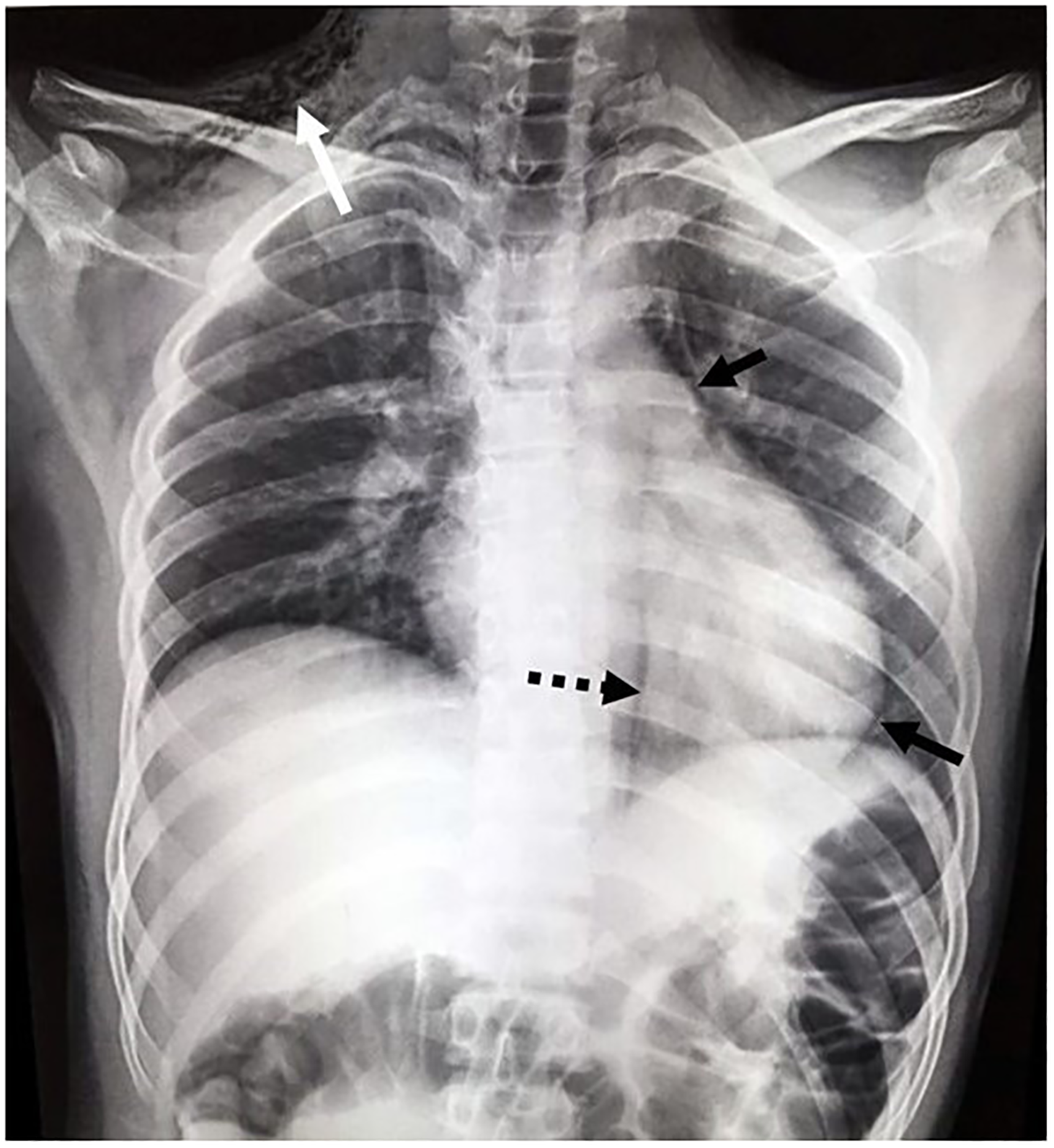
Patient chest radiograph showing pneumomediastinum (dotted black arrow) with pneumopericardium (solid black arrows) and subcutaneous emphysema in the right supraclavicular fossa (white arrow).

Chest computed tomography (CT). (A) Axial section at the level of the sternal manubrium showing subcutaneous emphysema in the left supraclavicular fossa (arrow). (B) Axial section corroborating the presence of air in the mediastinum (dotted white arrow). (C) Sagittal view showing the extent of subcutaneous emphysema.
Discussion
Inhalation of illicit drugs such as cocaine, 15 mephedrone, 16 ecstasy, 17 crack cocaine, 18 and vaporized methamphetamine, 19 accidental exposure to inhaled toxicants such as bromine 20 and chlorine, 21 and the recreational use of nitrous oxide (nitric oxide [NO]) 14 have been reported to produce SPM.
The pathomechanism of SPM may vary depending on the substances involved. In the case of cocaine, it is believed that the forceful Valsalva maneuver performed by cocaine users after deep nasal inhalation of the drug may lead to barotrauma, resulting in alveolar rupture and air infiltration into the posterior mediastinum. 15 The same mechanism would probably apply to ecstasy (methylenedioxymethamphetamine), which is usually taken orally or rectally. However, ecstasy can also be crushed and snorted, requiring a vigorous Valsalva maneuver for deep inhalation. 17 As with cocaine, this can lead to barotrauma and SPM. In contrast, NO inhalation, which is used recreationally for its euphoric effects, has been linked to SPM through a different mechanism. 14 NO is produced by the combustion of certain tissues or cellulose. Owing to its insolubility in water, it cannot be removed by the protective mucus layer of the upper respiratory tract. As a result, it quickly reaches the alveolar space and causes an abrupt expansion of the entire tracheobronchial tree due to the exchange of small amounts of nitrogen with much larger amounts of NO from the blood. 22 NO-induced injury has been observed to occur up to 72 h after exposure. Accidental inhalation injury from bromine and chlorine gas, which are potent airway irritants, may ultimately lead to SPM due to severe coughing, bronchospasm, and chemical pneumonitis.20,21 Both agents can also cause other serious systemic toxic effects.
Paint diluents or thinners consist of methanol, acetone, aromatic (benzene, naphthalene, toluene, and xylene), and aliphatic (turpentine) hydrocarbons. Similar to NO, hydrocarbons have low viscosity, low surface tension, and high volatility, and are insoluble in water. Therefore, they are not removed by the mucous layer lining the upper airways and can easily flow into the alveoli. The toxicity of hydrocarbons has been well documented. 23 They primarily cause pneumonitis, which is the most common adverse effect. 24 Furthermore, hydrocarbons can cross the alveolar barrier and cause multiple organ toxicity, particularly cardiovascular, neurological, and gastrointestinal toxicity. Fatalities have been reported among painters exposed to high concentrations of paint thinner while working in poorly ventilated areas.24,25 However, to the best of our knowledge, after an exhaustive literature review, we have not found any cases of SPM because of or in relation to excessive exposure to paint thinner vapors. It is likely that the alveolar rupture and subsequent development of SPM and subcutaneous emphysema in this case were triggered by inhaled diluent fume pneumonitis along with an increase in respiratory effort due to chest pain and anxiety. Thoracic pain due to the SPM was an alarm signal for the patient to leave the workplace and seek medical help. Otherwise, prolonged overexposure to paint thinner fumes can result in severe symptoms of organ toxicity. Paint thinner inhalation in search of euphoric effects and the use of illicit substances were ruled out in the present case.
Some authors 26 have suggested that an extensive workup is unnecessary in these cases, especially in young patients. In a previous study, none of the 49 patients underwent bronchoscopy; only 17% underwent esophagography, and 22% were managed on an outpatient basis. However, we did not share this perspective. We believe that hospitalization should be considered on a case-by-case basis, depending on the cause of the SPM. It has been reported that hydrocarbon aspiration can cause serious complications, such as necrotizing pneumonitis, atelectasis, and lung abscess formation, 27 not to mention the risk of mediastinitis secondary to pneumomediastinum. 28 Therefore, in the present case, it was decided that the most prudent course of action would be to admit the patient to the hospital for at least 5 days for observation, appropriate diagnostic assessment, and parenteral antibiotic administration.
Conclusion
This case should alert primary care providers and the public that exposure to paint thinners, hydrocarbon-based chemical compounds widely used in homes and enclosed spaces, can cause SPM if misused. It is not too speculative to assume that similar cases might have been underreported to date, largely because of the self-limiting nature of SPM.
Footnotes
Acknowledgments
None.
Author contribution(s)
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
Not applicable.
Consent for Publication
Written informed consent to publish anonymized patient data was obtained from the patient's mother in the presence of a CEISH staff member.
Ethical Approval
The Ethics Committee for Human Research of the Catholic University of Cuenca (CEISH-UCACUE), according to the local regulations for approval and oversight (CEISH) published in the Official Registry of the Ministry of Health of Ecuador, issued a waiver (CEISH-UCACUE-070) stating that this clinical case report is exempt from evaluation by this committee.