
Abstract
Purpose:
Right ventricular (RV) dysfunction in acute pulmonary embolism (PE) is a critical determinant of outcome. Obstructive sleep apnea (OSA) is a common comorbidity of PE and might also affect RV function. Therefore, we sought to investigate RV dysfunction in PE patients in proportion to the severity of OSA by evaluating the right-to-left ventricular (RV/LV) diameter ratio on computed tomographic pulmonary angiography (CTPA).
Materials and Methods:
197 PE patients were evaluated for sleep-disordered breathing by portable monitoring and nocturnal polysomnography. RV dilatation was defined as an RV/LV diameter ratio of ⩾ 1.0.
Results:
RV dilatation was significantly more frequent in OSA patients compared to study participants without OSA (66.4% vs 49.1%, P = .036). Elevated troponin I values, indicating myocardial injury due to acute, PE-related RV strain, were significantly more frequent in OSA patients with an apnea-hypopnea index (AHI) ⩾ 15/h compared to those with an AHI < 15/h (62.1% vs 45.8%, P = .035). However, RV dysfunction documented by the RV/LV diameter ratio on CTPA was not significantly associated with the severity of OSA in multivariable regression analysis.
Conclusion:
Patients with moderate or severe OSA might compensate acute, PE-related RV strain better, as they are adapted to repetitive right heart pressure overloads during sleep.
Keywords
Introduction
Obstructive sleep apnea (OSA) is a breathing disorder, which is characterised by recurrent upper-airway obstructions during sleep, resulting in repetitive episodes of hypopnea or apnea. 1 It is known that OSA is an independent risk factor for cardiovascular morbidity and death. 2
Pathophysiologically, OSA is associated with oxygen desaturation, intermittent hypoxia, hypercapnia, intrathoracic pressure swings, and an increase of pulmonary arterial pressure during sleep. 3 All these mechanisms affect right ventricular (RV) function. Decreased right heart performance has been repeatedly described in OSA patients.4 -7 RV function seems to be impaired in proportion to the severity of OSA4,5 and has been shown to be reversible by continuous positive airway pressure (CPAP) therapy.6,7
In acute pulmonary embolism (PE), RV dysfunction is a critical determinant of outcome and is associated with a poor short- and long-term prognosis. 8 Although OSA is a common comorbidity of PE, 9 it is unknown if OSA patients have a higher prevalence of RV dysfunction when presenting with acute PE than patients without relevant sleep disordered breathing (SDB). We therefore sought to investigate signs of RV dysfunction in patients suffering from acute PE according to the presence and the severity of OSA.
Materials and Methods
Study design, imaging tests and clinical data
This observational cohort study was conducted at a tertiary academic teaching hospital, where patients with acute PE were enrolled between July 2011 and March 2016. Data were collected prospectively.
In all patients, the diagnosis of PE was established by multi-detector computed tomographic pulmonary angiography (CTPA), performed using the routine scan protocols of our institution. RV dysfunction was assessed by calculating the right-to-left ventricular (RV/LV) diameter ratio on standard CTPA images. RV/LV ratios were determined in consensus by 2 radiologists with extensive experience in cardiovascular CT using standard axial plane reconstructions. Both readers were blinded towards sleep study results. Maximum RV and LV diameters were defined manually as the maximum distance of the endocardial border of the right or left ventricle from the interventricular septum; thereby, the largest RV and LV diameters were typically observed at different craniocaudal positions of the heart. RV dilatation was defined as a RV/LV diameter ratio of ⩾ 1.0 (Figure 1).
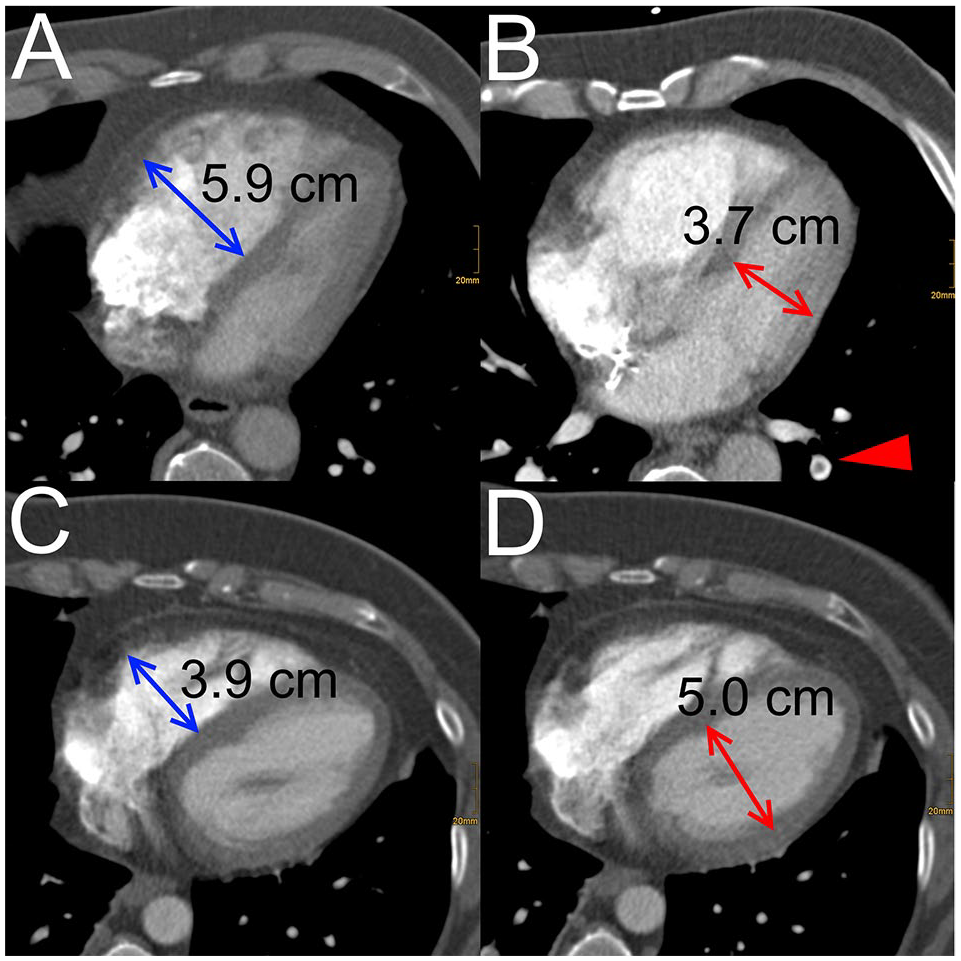
Comparison of a patient with signs of RV dysfunction manifesting as a pathological increase of the RV-LV-ratio: (A) maximal transversal diameter of the right ventricle, (B) maximal transverse diameter of the left ventricle with a patient without signs of RV dysfunction, (C) maximal transversal diameter of the right ventricle and (D) maximal transverse diameter of the left ventricle. In panel (B) parts of the underlying pulmonary embolism can be appreciated in the left lower lobe (red arrow head).
Patients’ histories were taken by study nurses who were blinded for sleep study results and were directed towards comorbidity including concomitant lung diseases (CLD), congestive left heart failure (CHF), cerebrovascular diseases (CVD) and a history of active cancer. Biomarkers indicating ventricular pressure overload [N-terminal pro-brain-type natriuretic peptide (NT-proBNP)] and myocardial injury due to acute RV strain [(troponin I (TNI)] were measured on admission. PE patients were screened for SDB by portable monitoring (PM) during hospitalisation as soon as they became clinically stable for the performance of sleep studies. As we planned to perform nocturnal polysomnography (PSG) in case of a positive PM result, only patients who were suitable for potential over-night PSG were recruited. Subjects under CPAP treatment, severe mental or physical impairment or a life-expectancy of less than 1 year were excluded from the study. Sleep assessment was performed and validated as previously described. 9 All study participants filled out an Epworth Sleepiness Scale (ESS) questionnaire. 10 Nocturnal PSG was performed in all patients with an apnea-hypopnea index (AHI) ⩾ 15/h documented by PM and in all subjects with a PM-AHI < 15/h but evidence of increased daytime sleepiness, defined as an ESS score > 10. 10 In patients who received both PM and PSG, PSG was performed within 30 days after PM and only PSG-derived sleep parameters were analysed. According to international standards, OSA was declared to be mild when the AHI was 5 to 14/h, moderate when the AHI was 15 to 29/h, and severe when the AHI was ⩾ 30/h. 11
Statistical analysis
The statistical analysis was performed using IBM SPSS Statistics version 25. The Shapiro-Wilk test was used to test for the normality of distribution in continuous variables. Continuous variables were given as means ± standard deviations and they were analysed by the T-Test and ANOVA. Categorical variables were specified as amounts (with percentages of total) and their distribution was further analysed by the Chi-Square test. For binary variables logistic regression analysis was performed whereas continuous parameters were tested by linear regression analysis. The level of significance was chosen at α = 0.05 and the probability values were given 2-tailed. In case of multiple testing, the level of significance was adapted using the Bonferroni-adjustment.
Results
The clinical characteristics, the results of the laboratory tests, and the radiological findings of the study population were summarized in Tables 1 and 2. A total of 197 patients could be enrolled. During the recruitment period, 495 patients with acute PE were treated at our department. Out of these 495 patients, 86 died during hospitalisation. From the remaining 409 patients, 59 did not receive CTPA at our institution (either due to high-risk PE, external CTPA diagnosis or renal impairment) and 63 patients were excluded from the trial. Thus, 90 patients were missed for screening due to other reasons during the whole study period. The 30 days mortality rate of the study cohort was 0.5%.
Characteristics of the study cohort depending on the AHI.

Abbreviations: AHI, apnea-hypopnea index; CHF, congestive left heart failure; CLD, concomitant lung disease; CVD, cerebrovascular disease; HR, heart rate; LV, left ventricle; RV, right ventricle; SO2, oxygen saturation; sPESI, simplified pulmonary embolism severity index; TNI, troponin I.
Characteristics according to the severity of obstructive sleep apnea (OSA).

Abbreviations: AHI, apnea-hypopnea index; CHF, congestive left heart failure; CLD, concomitant lung disease; CVD, cerebrovascular disease; HR, heart rate; LV, left ventricle; RV, right ventricle; SO2, oxygen saturation; sPESI, simplified pulmonary embolism severity index; TNI, troponin I.
In case of multiple testing, the level of significance was adapted to α = 0.008 using the Bonferroni-adjustment.
In comparison with patients with no or only mild OSA, subjects with an AHI ⩾ 15/h were significantly older (71 ± 11 years vs 55 ± 18 years, P = <.001). sPESI scores ⩾ 1 and elevated TNI values were significantly more frequent in moderate to severe OSA (86.4% vs 63.4%, P = .001 and 62.1% vs 45.8%, P = .035, respectively), and the frequencies were increasing depending on the severity of OSA. For NT-proBNP levels, a similar trend could be documented, but the differences failed to be significant. Concomitant diseases were equally distributed in all different study subgroups. CHF as comorbidity was very rare in the entire study population (2.0%).
In 61.4% of the entire study cohort the RV/LV diameter ratio was ⩾ 1 on CTPA. RV/LV ratios ⩾ 1 could be identified in 49.1% of PE patients with no OSA, in 70.3% of subjects with mild OSA, in 57.1% of PE patients with moderate OSA and in 65.8% of subjects with an AHI ⩾ 30/h. RV diameters were significantly larger in PE patients with mild or severe OSA compared to study participants with an AHI < 5/h (P = .002 and P = .012, respectively). RV/LV diameter ratios ⩾ 1 were significantly more frequent in OSA patients compared to study participants with an AHI < 5/h (66.4% vs 49.1%, P = .036). However, the AHI was not an independent predictor for the size of the RV (ß = 0.092, P = .230), the RV/LV diameter ratio (ß = −0.013, P = .868), or an RV/LV diameter ratio ⩾ 1 (OR (95% CI) = 1.006 (0.985-1.027), P = .591) when tested in a multivariable regression analysis adjusted for age, gender and comorbidity. Correspondingly, the prevalence of RV/LV diameter ratios ⩾ 1 did not significantly change in proportion to the severity of OSA (Figure 2).
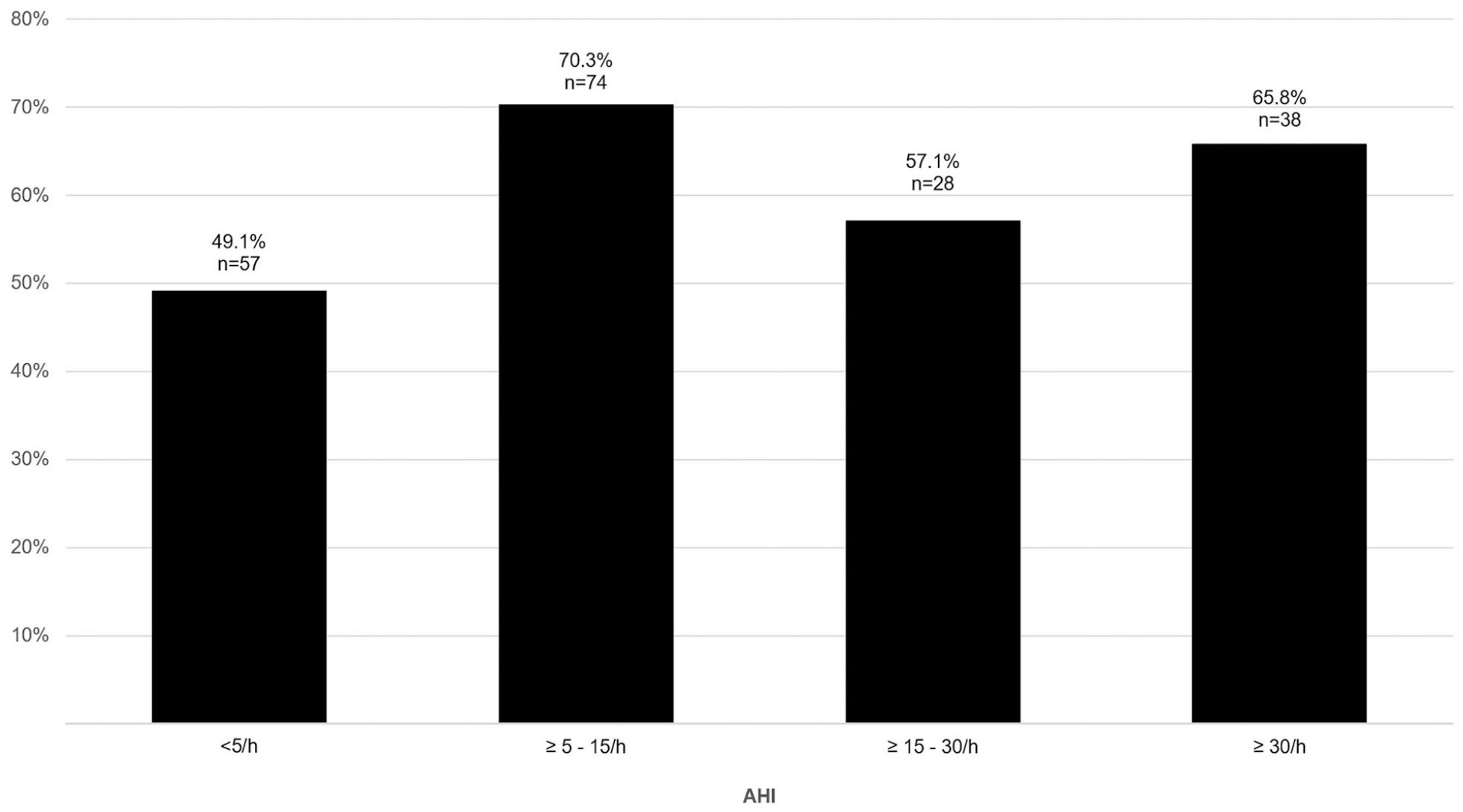
Right-to-left ventricular (RV/LV) diameter ratio ⩾1 according to the AHI.
Discussion
In the present study, we investigated RV dysfunction in patients presenting with acute PE in proportion to the severity of OSA by evaluating the RV/LV diameter ratio on CTPA. We found that RV dilatation was significantly more frequent in PE patients with OSA compared to study participants with an AHI < 5/h. However, RV dysfunction documented by the RV/LV diameter ratio on CTPA was not associated with the severity of OSA.
The RV/LV diameter ratio assessment on CTPA has been proven to be accurate and reproducible in identifying RV dysfunction 12 and has been evaluated to be effective in predicting short-term mortality in acute PE.13,14 Meanwhile, our findings have been confirmed by a recent study. 15
These observations might be explained by several circumstances: on the one hand, it has been postulated that the elevation in pulmonary arterial pressure seems to be generally mild in OSA and severe RV dysfunction only appears in the presence of other underlying diseases, such as CHF with an impaired cardiac reserve, for example Sajkov and McEvoy 3 and Furlan et al. 14 In our study population, such comorbidities were rare, possibly explaining the fact that we didn`t observe any association between the severity of OSA and the prevalence of RV dysfunction.
However, other investigators found the prevalence of pulmonary hypertension (PH) among OSA patients to be between 20% and 40% even in the absence of other known cardiopulmonary disorders, suggesting that episodic sleep apnea and intermittent nocturnal hypoxemia are sufficient to cause PH. 3 In our study, we were able to demonstrate that RV dilatation was significantly more frequent in PE patients with OSA compared to study participants with an AHI < 5/h. In addition, biomarker levels indicating acute RV strain were higher in PE patients suffering from OSA, especially severe OSA. In a mouse model, intermittent hypoxia mimicking OSA results in sustained PH, vascular remodelling and RV hypertrophy. 16 Furthermore, a reduction in pulmonary artery pressure has been reported in OSA patients after initiation of nocturnal CPAP treatment, 17 suggesting a pathophysiological association between these 2 conditions. However, the prevalence of RV dysfunction documented by the RV/LV diameter ratio on CTPA did not increase in proportion to the severity of OSA in our study. A possible explanation for this observation might be that patients with relevant OSA might compensate acute, PE-related RV strain better compared to PE patients without SDB, as they may be adapted to repetitive RV pressure overload during sleep. Intermittent nocturnal hypoxia, oxidative stress, systemic inflammation and sympathetic overactivation may cause PH, resulting in repetitive RV pressure overloads during sleep in OSA patients. 18 Animal studies have shown that the right heart can adapt fairly rapidly to increased RV pressure over the course of a couple of weeks. 19 Thus, PE patients with relevant OSA might compensate acute, PE-related RV strain better compared to PE patients with no or only mild OSA, as they are ‘trained’ for recurrent RV pressure overloads. This theory might even explain the highest prevalence of RV/LV diameter ratios ⩾ 1 in the mild OSA cohort.
Our trial has several strengths like the prospective enrolment, the representative sample size and the high-quality sleep-studies. However, we admit that our study has also some limitations. First, we did not enrol consecutive patients. All our study participants qualified for sleep studies and might therefore be less severely affected by comorbid diseases. This fact might result in a selection bias and explain the very low short-term mortality rate of our study population. Moreover, although the total study population has a representative sample size, our study might be statistically underpowered to analyse possible confounding effects of comorbid diseases on our study results. Second, our CT imaging studies were not correlated with echocardiographic findings. However, earlier studies have shown that the CT assessment of right heart strain in acute PE correlates well with echocardiographic findings. 20 Third, we are not able to report follow-up data like PE recurrence or long-term survival. Thus, we cannot draw any prognostic conclusions from our observations. However, as we have demonstrated in another study that OSA might affect long-term prognosis in acute PE, 21 investigating the RV/LV diameter ratio alone might not be sufficient in predicting survival of OSA patients suffering from acute PE. As the prevalence and severity of OSA is increasing with age, our findings might, at least in part, explain results of another study indicating a lower prognostic value of the RV/LV diameter ratio in elderly patients with acute PE. 22
Conclusion
In summary, RV dilatation was significantly more frequent in PE patients with OSA compared to PE patients without SDB. However, RV dysfunction documented by the RV/LV diameter ratio on CTPA was not associated with the severity of OSA. We conclude that patients with moderate or severe OSA might compensate acute, PE-related RV strain better, as they are adapted to repetitive right heart pressure overloads during sleep.
Footnotes
Acknowledgements
We are very grateful to Mrs. Yvonne Eglinger for proof reading the manuscript.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ contributions
Availability of data and material
Data are available upon reasonable request from the corresponding author.
Ethics approval and consent to participate and for publication
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was conducted with the approval of the Institution’s Ethics Committee (project number 080-11 with an amendment BKF 2017-73). All patients gave written informed consent to participate in the trial and for the publication of the study results.