
Abstract
Introduction:
Klippel–Trenaunay syndrome (KTS) is a rare congenital vascular disorder defined by the triad of capillary malformation, venous or lymphatic anomalies, and soft tissue or bony hypertrophy. Pediatric presentations pose distinct challenges because clinical manifestations evolve with growth, and early phenotypes may not reliably predict long-term morbidity. In early childhood, accurate flow phenotyping and anticipatory surveillance are therefore central to management.
Case Presentation:
A 4-year-old girl presented with an extensive port-wine stain involving nearly half of the right buttock, progressive hypertrophy of the right lower limb, and superficial varicosities. Limb circumference differed by 3.5 cm at the thigh and 2.8 cm at the calf compared with the contralateral side. Doppler ultrasonography demonstrated superficial venous ectasia with preserved deep venous flow and no evidence of arteriovenous shunting. Magnetic resonance venography confirmed superficial venous malformations confined to the right lower limb without pelvic or visceral involvement. Radiographs revealed cortical thickening and bony overgrowth of the right foot, and scanogram analysis demonstrated a 1.2 cm limb-length discrepancy. Conservative management with compression therapy, orthopedic surveillance, and regular dermatologic follow-up was initiated. At 6 months, the child remained asymptomatic, functionally active, and without progression of hypertrophy.
Discussion:
This case illustrates the diagnostic and management considerations of KTS in early childhood, emphasizing differentiation from high-flow vascular syndromes, justification of imaging strategies, and the importance of growth-adapted surveillance and family counseling. Emerging targeted therapies may offer future options for progressive disease.
Conclusion:
Early recognition, structured monitoring, and multidisciplinary care are essential in pediatric KTS. Conservative management is effective when paired with defined surveillance strategies and caregiver-centered education.
Keywords
Introduction
Klippel–Trenaunay syndrome (KTS) is an uncommon congenital vascular malformation syndrome first described in 1900, characterized by the triad of capillary malformations, venous or lymphatic anomalies, and hypertrophy of soft tissue and bone. 1 It is estimated to occur in 3 to 5 per 100 000 live births, although the true incidence may be higher because of underrecognition in milder phenotypes. 2 Most cases are sporadic, with no gender or ethnic predilection. 3
Pathogenetically, KTS belongs to the PIK3CA-related overgrowth spectrum (PROS) caused by somatic mosaic mutations in the PIK3CA gene.4,5 Dysregulated activation of the PI3K–AKT–mTOR signaling cascade leads to aberrant angiogenesis and segmental overgrowth of tissues.6,7 Clinical severity is highly variable, ranging from subtle cosmetic disfigurement to disabling hypertrophy and chronic venous insufficiency. 1 Clinically, this variability forces decision-making under uncertainty, particularly in preschool children where growth trajectories can amplify limb discrepancy and venous hypertension over time. 8 The mosaic nature of the underlying genetic alteration results in temporally evolving and anatomically heterogeneous manifestations, making early phenotypic classification inherently challenging.
Cutaneous manifestations typically present as port-wine stains, most frequently localized to the pelvis or extremities. 9 Venous anomalies include superficial varicosities, deep venous hypoplasia, and persistence of embryonic veins, predisposing to thrombosis and venous hypertension. 10 Skeletal involvement often results in limb-length discrepancy, joint deformity, and gait disturbance. 11 Progressive complications include recurrent cellulitis, lymphedema, chronic pain, hemorrhage, and rarely visceral vascular malformations. 12 Importantly, many of these complications emerge gradually and may not be clinically apparent during early childhood, despite the presence of established anatomic abnormalities.
Diagnosis is primarily clinical, but imaging plays a key role in characterizing vascular anatomy and excluding mimics such as Parkes Weber syndrome, where high-flow arteriovenous shunts are present. 13 Distinguishing low-flow combined vascular malformations from high-flow arteriovenous processes is particularly critical in pediatric patients, as misclassification may lead to inappropriate investigations or premature interventions with long-term consequences. Management is individualized and multidisciplinary, centered on conservative measures such as compression therapy and orthopedic monitoring. In recent years, targeted agents including alpelisib and sirolimus have shown promise in PROS-related phenotypes.14,15 However, the timing and indication for such therapies in early childhood remain areas of active clinical deliberation, reinforcing the need for careful longitudinal assessment rather than reflexive escalation.
Beyond diagnosis, pediatric KTS presents distinct challenges related to surveillance and family counseling. Surveillance strategies must account for growth-dependent progression of limb asymmetry, venous disease evolution, and delayed onset of complications, necessitating structured, anticipatory monitoring rather than symptom-driven follow-up. Concurrently, caregivers must be guided through uncertainty regarding prognosis, adherence to conservative measures, and recognition of early warning signs that warrant reassessment. These counseling demands are integral to effective management but are infrequently detailed in case-based literature.
Following the CARE guidelines (for CAse REports), 16 we report a pediatric patient with complete clinical triad of KTS and describe the challenges of diagnosis, surveillance, and family counseling in early childhood. By detailing the clinical reasoning underlying diagnostic evaluation, imaging selection, and follow-up planning, this report aims to contextualize early pediatric KTS management within a growth-sensitive and multidisciplinary framework.
Case Presentation
A 4-year-old girl, born to healthy non-consanguineous parents following an uncomplicated pregnancy and vaginal delivery, was referred to dermatology for evaluation of a reddish lesion on the right buttock. The lesion had been present since birth and had gradually darkened in color. Parents also noted progressive enlargement of the right leg compared with the left, which became increasingly evident after the age of 2 years. There was no history of recurrent infections, abnormal bleeding, seizures, or gastrointestinal bleeding. Growth and developmental milestones were appropriate for age. A practical challenge reported by caregivers was distinguishing benign “birthmark change” from disease progression, which influenced timing of specialist referral. There was no family history of vascular malformations, overgrowth syndromes, or congenital limb asymmetry, reducing the likelihood of an inherited vascular disorder.
On examination, an erythematous, blanchable capillary malformation consistent with a port-wine stain was observed, covering approximately half of the right buttock surface (Figure 1A). The lesion demonstrated homogeneous coloration without nodularity, ulceration, or overlying skin atrophy, and no associated warmth was appreciable on palpation. The right lower limb was hypertrophied, with a circumference difference of 3.5 cm at mid-thigh and 2.8 cm at mid-calf compared with the left. Superficial varicosities were evident along the posterior thigh and calf (Figure 1B). The right foot demonstrated bony overgrowth with broadening of the metatarsal region and toes (Figure 1C). The overlying skin was intact, with no ulceration or lymphorrhea. Gait was normal and there was no functional impairment. Peripheral pulses were symmetrical and no bruits or thrills were detected. Systemic examination was otherwise unremarkable. The absence of local hyperthermia, thrill, or audible bruit was clinically relevant in lowering suspicion for an underlying high-flow arteriovenous process, although this could not be excluded on examination alone given the patient’s age.

Clinical features of Klippel–Trenaunay syndrome in a 4-year-old female (black arrows): (A) faint port-wine stain on the right buttock, (B) hypertrophy and superficial varicosities of the right lower limb, and (C) bony hypertrophy of the right foot.
Laboratory investigations including complete blood count, coagulation profile, and renal and liver function tests were within normal limits. Baseline coagulation assessment was obtained to exclude occult consumptive coagulopathy, which may complicate extensive vascular malformations even in the absence of overt bleeding. 17 Doppler ultrasonography revealed superficial venous ectasia with preserved flow in the deep venous system and no evidence of arteriovenous shunting. Magnetic resonance venography confirmed superficial venous malformations confined to the right lower limb without pelvic or visceral extension. Importantly, deep venous patency was preserved, and no dilated feeding arteries or early venous filling were identified, supporting a low-flow vascular phenotype. Plain radiographs of the right leg and foot demonstrated cortical thickening and bony overgrowth. A scanogram documented a limb-length discrepancy of 1.2 cm, with the right limb longer than the left. In the diagnostic pathway, the key uncertainty was whether the visible varicosities reflected isolated superficial venous ectasia versus a broader venous malformation network requiring deeper anatomic mapping; this uncertainty justified cross-sectional venous imaging. At this stage, the diagnostic focus shifted from confirmation of KTS to exclusion of conditions with distinct hemodynamic and prognostic implications.
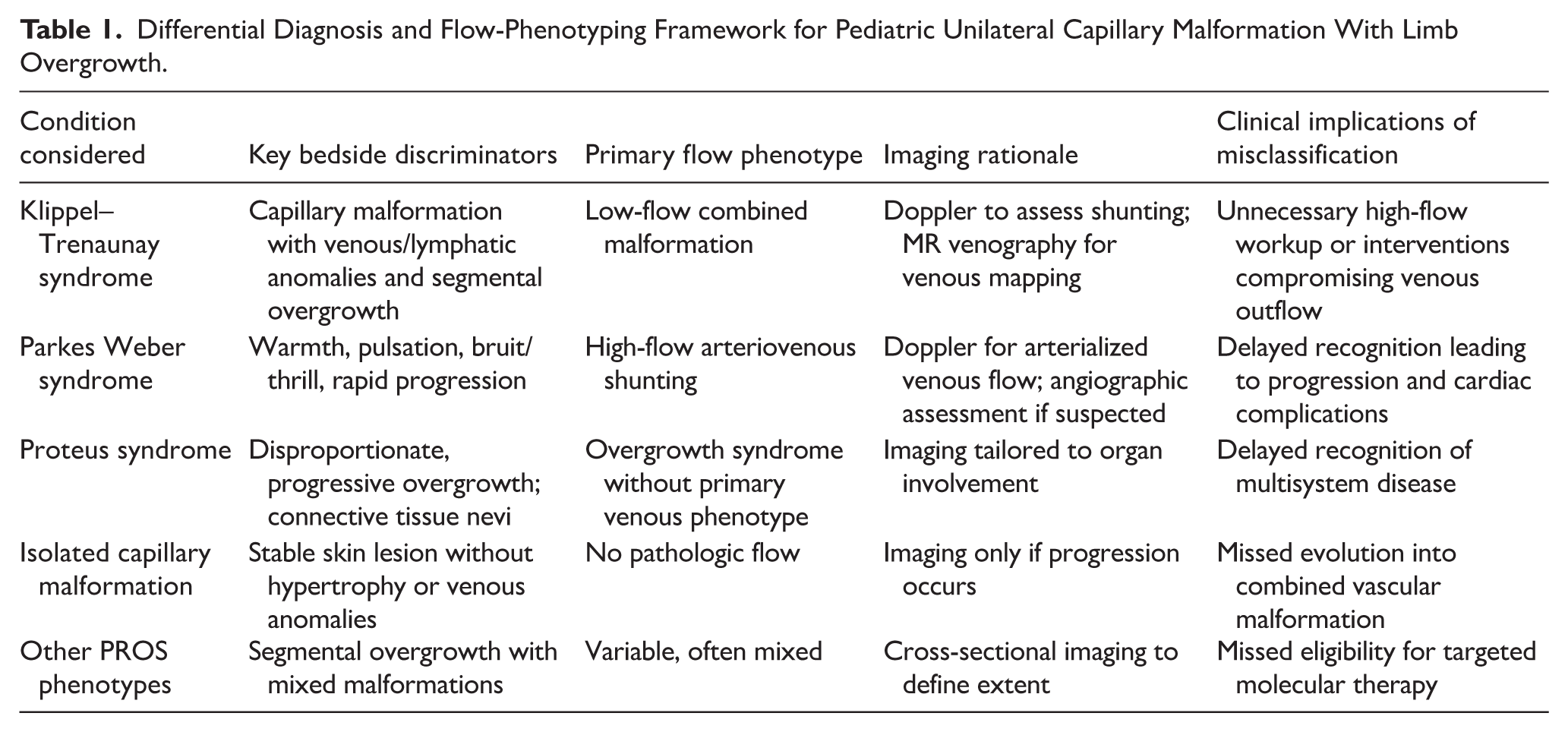
The clinical triad of extensive capillary malformation, venous malformation, and hypertrophy of both soft tissue and bone confirmed the diagnosis of KTS. Differential diagnoses including Parkes Weber syndrome (excluded by absence of arteriovenous shunting), Proteus syndrome (excluded by absence of cerebriform connective tissue nevi and disproportionate overgrowth), and isolated capillary malformation were considered. Differential-diagnosis checkpoints applicable to this presentation are outlined in Table 1.9,18 -21 The absence of progressive, disproportionate overgrowth or connective tissue nevi further reduced the likelihood of alternative PROS phenotypes.
Differential Diagnosis and Flow-Phenotyping Framework for Pediatric Unilateral Capillary Malformation With Limb Overgrowth.
Conservative management was initiated. Graduated compression stockings were prescribed to reduce venous congestion. Compression selection and fitting were tailored to the child’s age and limb dimensions, with caregiver education provided regarding daily wear duration, skin inspection, and seasonal tolerance. Orthopedic evaluation recommended annual scanogram to monitor progression of limb-length discrepancy. Dermatology follow-up was arranged every 6 months. Parents were counseled regarding the chronic course of the disease, risk of thrombosis, recurrent cellulitis, venous insufficiency, and possible need for interventional or surgical procedures in the future. Counseling emphasized the growth-dependent nature of disease progression, the rationale for conservative management in an asymptomatic child, and specific warning signs that should prompt earlier reassessment, including acute limb pain, swelling, erythema, or functional decline.
At 6-month follow-up, the child remained active, pain-free, and without measurable progression of hypertrophy. A structured counseling approach was used to align family expectations with the reality of growth-dependent change, including discussion of adherence barriers to compression garments in preschool children and the need for escalation criteria rather than routine procedural intervention. The salient clinical findings, imaging characteristics, management plan, and follow-up outcomes of the present case are summarized in Table 2. Ongoing surveillance was planned with flexibility to intensify monitoring during anticipated growth spurts.
Summary of Clinical Findings, Imaging, Management, and Follow-Up.

Discussion
Klippel–Trenaunay syndrome represents a complex interaction between dysregulated vascular development and somatic growth, in which clinical risk is determined not solely by the presence of malformations, but by their hemodynamic behavior and response to longitudinal growth. In early childhood, the principal clinical challenge lies in anticipating which anatomic abnormalities will remain indolent and which may evolve into function-limiting or complication-prone disease as biomechanical and circulatory demands increase. This uncertainty necessitates interpretive reasoning that extends beyond static diagnosis.
A central interpretive issue in pediatric vascular anomalies is the distinction between low-flow combined malformations and high-flow arteriovenous entities. Although clinical examination provides important cues, its discriminatory power is limited in young children, where compensatory mechanisms may mask early hemodynamic consequences. 22 The analytical emphasis, therefore, shifts from identifying visible abnormalities to understanding flow characteristics, venous outflow integrity, and their downstream implications. Preservation of deep venous drainage is particularly consequential, as it modulates the risk of venous hypertension, thrombosis, and chronic pain syndromes later in life. 23 This principle underpins contemporary approaches to risk stratification in low-flow vascular malformations.
Skeletal overgrowth in Klippel–Trenaunay syndrome warrants interpretation as a dynamic biomechanical process rather than a static morphologic feature. Even modest asymmetry in early childhood may alter load distribution across developing joints, with cumulative effects that only become apparent during growth acceleration. 24 The clinical relevance of early skeletal assessment lies in establishing growth-sensitive baselines that permit detection of deviation from expected trajectories, thereby enabling timely orthopedic intervention before secondary musculoskeletal adaptation occurs. Such anticipatory frameworks align management with prevention of disability rather than correction of established dysfunction.
Conservative management remains foundational in asymptomatic pediatric patients; however, conservatism should be understood as structured vigilance rather than therapeutic inertia. Compression therapy serves not only to mitigate venous congestion but also to reduce inflammatory signaling associated with venous stasis, which may contribute to pain and recurrent infection.25,26 Its effectiveness in young children is contingent upon individualized fitting, caregiver education, and periodic reassessment as limb dimensions change. Dermatologic surveillance complements this strategy by addressing skin barrier integrity, which plays a critical role in preventing cellulitis and lymphatic complications.
Family engagement is integral to successful long-term management. Caregivers must navigate a condition characterized by visible asymmetry, uncertain progression, and prolonged surveillance, often without immediate clinical intervention. Effective counseling therefore extends beyond diagnostic explanation to include normalization of uncertainty, clarification of escalation thresholds, and reinforcement of the rationale for conservative strategies. When families understand the link between growth, vascular physiology, and future risk, adherence to monitoring plans improves and unnecessary procedural pressure is reduced.
Multidisciplinary coordination becomes increasingly important as children age and disease manifestations intersect multiple organ systems. Dermatology, vascular medicine, orthopedics, and interventional radiology contribute complementary perspectives that guide staged decision-making. The multidisciplinary approach opted in this case is summarized in Table 3. Procedural interventions are reserved for clearly symptomatic venous malformations, where benefits outweigh the risk of disrupting compensatory venous pathways. Importantly, intervention based solely on imaging abnormality, in the absence of clinical impact, may compromise long-term venous function and should be avoided.
Multidisciplinary Surveillance Framework Applied in the Present Case.

Long-term management requires multidisciplinary coordination, as disease manifestations may intersect dermatology, vascular medicine, orthopedics, interventional radiology, and, in advanced cases, hematology. Procedural interventions such as sclerotherapy or embolization are reserved for symptomatic venous malformations and should be guided by symptom burden and anatomic feasibility rather than imaging abnormalities alone. 27 More recently, targeted molecular therapies directed at the PI3K–AKT–mTOR pathway have expanded therapeutic possibilities for progressive or refractory disease. Sirolimus has demonstrated benefit in slow-flow vascular malformations by reducing inflammatory activity and pain,28,29 while alpelisib offers a genotype-directed option for selected PIK3CA-related overgrowth phenotypes. 30 In early childhood, these agents are generally reserved for clearly progressive or function-limiting disease, but their availability influences long-term planning and counseling.
Several limitations of this case warrant consideration. The relatively short duration of follow-up precludes assessment of growth-phase acceleration, which commonly unmasks venous and skeletal complications during later childhood or adolescence. Molecular confirmation of a PIK3CA mutation was not performed, limiting direct genotype–phenotype correlation, although clinical and imaging features were characteristic of Klippel–Trenaunay syndrome. Additionally, while initial imaging established flow phenotype and venous anatomy, serial reassessment will be required to detect evolution over time, particularly during periods of rapid somatic growth. These constraints emphasize the importance of longitudinal observation in understanding disease behavior.
Conclusion
Pediatric Klippel–Trenaunay syndrome requires management strategies that account for evolving anatomy, growth-related risk, and hemodynamic behavior rather than static diagnostic labels. This case supports a cautious, flow-informed approach centered on structured surveillance and sustained family engagement. Such an approach allows timely recognition of clinically meaningful progression while avoiding premature intervention in children who remain functionally well.
Footnotes
Acknowledgements
Dr. Amogh Verma serves as an Associate Editor for Clinical Medicine Insights: Case Reports. He had no involvement in the editorial handling, peer review, decision-making process, or publication outcome of this manuscript. All editorial decisions were made independently in accordance with the journal’s standard editorial policies. The authors declare that this role did not influence the conduct, interpretation, or reporting of the study.
Ethical Considerations
Ethical approval was not required for this study as per the policies of our institution. The Institutional Review Board waived the need for approval in accordance with the institutional guidelines for case-based studies.
Consent to Participate
Written informed consent was obtained from the legal guardian of the patient to participate in this study.
Consent for Publication
Written informed consent was obtained from the legal guardian of the patient for publication of this study (including images or case details).
Author Contributions
Anant Khandelwal: Conceptualization, Methodology, Visualization, Investigation, Validation, Supervision, Project Administration, Writing – Original Draft, Writing – Review & Editing. Raihan Shakeel: Conceptualization, Methodology, Visualization, Investigation, Validation, Supervision, Project Administration, Writing – Original Draft, Writing – Review & Editing. Manjiri Rhishikesh Babar: Validation, Writing – Review & Editing. C S Bhargavram: Validation, Writing – Review & Editing. Amogh Verma: Conceptualization, Methodology, Visualization, Investigation, Validation, Supervision, Project Administration, Writing – Original Draft, Writing – Review & Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable to this article, as no datasets were generated or analyzed during the current study.
Generative AI Use Statement
Paperpal and ChatGPT-5 were used only for language and stylistic refinement. These tools had no involvement in study design, data analysis, interpretation, or content development. All intellectual contributions and scientific interpretations are the sole work of the authors, who take full responsibility for the accuracy, originality, and integrity of the manuscript.