
Abstract
Abstract
Purpose
Klippel-Trenaunay syndrome (KTS) is a rare combined vascular malformation composed of capillary malformation, lymphatic and/or venous malformation and limb overgrowth, which commonly affects the extremities. Due to limb involvement, it is not uncommon for these patients to require referral to an orthopaedic surgeon. Herein we reviewed the prevalence of orthopaedic diagnoses in a large cohort of KTS patients and described the associated surgical interventions.
Methods
Between 1976 and 2012, 410 patients fulfilling strict criteria for KTS were evaluated at a single institution. Patient charts were reviewed for demographic information, details of the clinical evaluation, orthopaedic consultation and surgical interventions.
Results
A total of 264 of 410 patients (64%) with confirmed KTS required orthopaedic evaluation. Of these 264 patients, 84% had documented limb-length discrepancy. Other common diagnoses included: angular deformities (10%), scoliosis (9%), osteopenia/osteoporosis (7%), pathological fractures (6%), joint contracture (5%), degenerative joint disease (4%) and limb/joint pain (4%). Of the 264 patients evaluated by orthopaedic surgery, 133 patients (50.4%) underwent 169 surgeries. Surgery was most commonly performed for limb-length discrepancy (62%). Multivariable analysis confirmed an orthopaedic condition was more likely in patients with lymphatic malformation (odds ratio (OR) 3.78; p < 0.001), as well as in those with bone and/or soft-tissue hypertrophy of the lower extremity (OR 7.51; p < 0.001) or foot (OR 3.23; p < 0.001).
Conclusion
Orthopaedic conditions are common in patients with KTS and approximately 50% require surgical intervention. Those with a lymphatic malformation and/or soft-tissue hypertrophy of the lower extremity are more likely to need surgery.
Level of Evidence
Level IV, Descriptive Case Series
Keywords
Introduction
Klippel-Trenaunay syndrome (KTS) is a rare, complex vascular malformation syndrome that typically affects the extremities. The associated vascular malformations form in utero and are derived from a combination of venous, lymphatic and/or mixed tissues.1,2 In accordance with the International Society for the Study of Vascular Anomalies (ISSVA) classification, the vascular malformation must be accompanied by a capillary malformation (port wine stain) and have associated overgrowth of the limb (Fig. 1). 3 Patients with KTS often have symptoms spanning multiple medical subspecialties, requiring a multi-disciplinary approach to care. Associated lymphedema in the affected extremities places patients at risk of skin breakdown, ulcers and even skin cancers. 4 Thromboembolic diseases may develop due to altered blood flow and clotting abnormalities.5,6 KTS has also been implicated in gastrointestinal bleeding, genitourinary bleeding and complications associated with pregnancy.7–10

Limb-length discrepancy, soft-tissue hypertrophy and overlying capillary malformation are apparent in this patient with Klippel Trenaunay syndrome.
Due to extremity involvement, it is not uncommon for these patients to be referred to an orthopaedic surgeon for evaluation of pain or disability. Lee et al 11 reported common causes of pain in patients with KTS, including chronic venous insufficiency, cellulitis, superficial thrombophlebitis, deep vein thrombosis, calcification of vascular malformations, growing pains, intraosseous vascular malformation, arthritis and neuropathic pain. In addition to pain, orthopaedic surgeons may be asked to evaluate these patients for longitudinal and angular growth abnormalities.12–14 While small case series and case reports exist regarding orthopaedic management of KTS, large cohort studies are lacking.12–16 The purpose of this study was to review the prevalence of orthopaedic diagnoses in a large cohort of KTS patients and describe the associated operative interventions.
Materials and methods
Institutional review board approval was obtained for this study. A retrospective medical record review was performed of 901 patients between 1976 and 2012 with a possible diagnosis of KTS. Patient records and photographs were evaluated to confirm the diagnosis based on the strict ISSVA classification for KTS (capillary malformation + venous +/- lymphatic malformation + tissue overgrowth), 3 yielding 410 cases. Medical and surgical records were evaluated for the age of presentation, sex, race/ethnicity, family history, location of disease, orthopaedic manifestations of disease and orthopaedic surgical interventions.
Associations of baseline features with orthopaedic diagnoses were evaluated using logistic regression and summarized with odds ratios (ORs) and 95% confidence intervals (CIs). Multivariable models were developed using backwards and forward selection using a statistical significance level of 0.05. Statistical analyses were performed using version 9.4 of the SAS software package (SAS Institute Inc., Cary, North Carolina).
Results
The medical records of 410 patients with confirmed KTS were reviewed. In all, 69% of patients were evaluated before the age of 18 years, with 34% evaluated within the first year of life. There was a slight female preponderance, which was not statistically significant (54% versus 46%; p = 0.63). The majority of patients were white (95%). KTS most commonly involved the lower extremities (91%).
In all, 264 of 410 patients (64%) with confirmed KTS required orthopaedic evaluation due to one or more orthopaedic diagnoses. Of these 264 patients, 84% had documented limb-length discrepancy (Fig. 2). Other common diagnoses included: angular deformities (10%), scoliosis (9%; Fig. 3), osteopenia/osteoporosis (7%; Fig. 4), pathological fractures (6%), joint contracture (5%), degenerative joint disease (4%) and limb/joint pain (4%). The presence of a lymphatic vascular malformation was associated with an increased need for orthopaedic evaluation (OR 2.5; p = 0.004). Orthopaedic diagnoses present in the cohort are summarized in Table 1.

Significant limb-length discrepancy, requiring surgical intervention, is apparent in this patient.

Posteroanterior radiograph of the lumbar spine in a Klippel Trenaunay syndrome patient demonstrating scoliosis measuring 25°.

Left knee diffuse osteopenia in a patient with Klippel Trenaunay syndrome, with cortical thinning compared with the contralateral side.
Orthopaedic diagnoses in patients with Klippel-Trenaunay syndrome
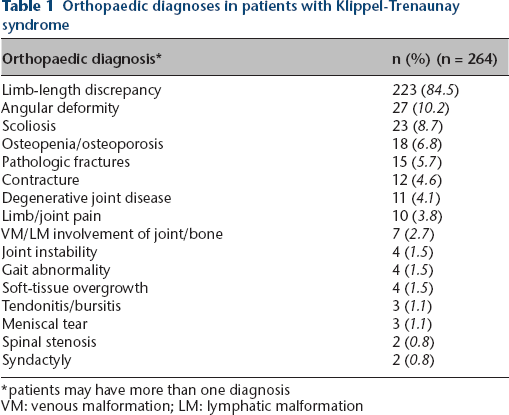
patients may have more than one diagnosis
VM: venous malformation; LM: lymphatic malformation
Of the 264 patients evaluated by orthopaedics, 133 patients (50.4%) underwent 169 operations. Surgery most commonly was performed for limb-length discrepancy (62%). A total of 43 patients underwent amputation of all or part of the affected limb (32% of those who required surgery and 10% of the total KTS cohort; Fig. 5). Other common procedures included arthroscopic debridement (10%), debulking of venous or lymphatic malformation (7%), total joint arthroplasty (5%) and pathological fracture fixation (4%). Orthopaedic surgeries performed in the cohort are summarized in Table 2.

Left below knee amputation with visible varicosities along the lateral aspect of the knee and proximal stump.
Orthopaedic surgeries in patients with Klippel-Trenaunay syndrome
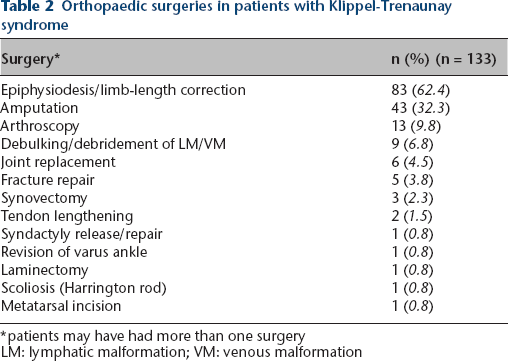
patients may have had more than one surgery
LM: lymphatic malformation; VM: venous malformation
A subgroup analysis of KTS patients based on the type of vascular malformation was also performed. Eight records did not specify the type of vascular malformation and were eliminated from this analysis. Of the remaining 402 patients, 263 required orthopaedic surgical evaluation (65%). A multivariable model confirmed an orthopaedic condition was more likely in patients with lymphatic malformation (OR 3.78; p < 0.001), as well as in those with bone and/or soft-tissue hypertrophy of the lower extremity (OR 7.51; p < 0.001) or feet (OR 3.23; p < 0.001). A vascular malformation in the buttocks, perineum or genitalia was also associated with an increased risk of orthopaedic diagnosis (OR 0.58; p = 0.029).
Discussion
KTS is a complex vascular malformation syndrome with clinical ramifications that bridge multiple medical and surgical subspecialties. Orthopaedic manifestations of KTS are common, presenting in almost two-thirds of patients. The orthopaedic surgeon is crucial in recommending both surgical and non-operative therapies. Physical medicine and rehabilitation physicians and physical therapists can also help to guide nonoperative therapies such as shoe lifts, stretching exercises and bracing. At many academic institutions, vascular anomaly clinics provide multidisciplinary care for patients with KTS and other vascular syndromes. In such programmes, it is best to involve the orthopaedic surgeon early to guide the optimal timing of intervention. However, in other programmes where patients with complicated vascular malformations are managed primarily by dermatologists, plastic surgeons, vascular surgeons and other subspecialties, it is important that paediatric orthopaedists remain involved in the care of these complex patients.
This study highlights the increased risk of orthopaedic diagnoses in patients with symptoms related to lymphatic malformation and/or tissue hypertrophy, a finding not previously described. Particularly in centres with vascular anomaly clinics, these patients may warrant pre-emptive evaluation by orthopaedics. Early involvement of the orthopaedist is particularly crucial in limb-length discrepancy, in order to determine the optimal timing of intervention to improve symmetry at skeletal maturity. Discrepancies of < 2 cm are typically managed non-surgically. 17 The rate of limb overgrowth in KTS is variable, though progression of limb-length discrepancy rarely occurs after age 12 years. Regular radiographs are essential in monitoring and predicting the timing of surgical intervention. 17
Scattered case reports and series discuss the surgical complications associated with orthopaedic procedures in patients with KTS.15–18 Special considerations include increased risk of perioperative bleeding, disseminated intravascular coagulation (DIC) and poor healing. Many patients require multiple unit blood transfusions intraoperatively,15,16 which should be communicated with anaesthesia and operative staff prior to surgical intervention. In a series of 11 patients with vascular malformations and associated knee arthropathy, six patients required transfusions obtained from an intraoperative cell saver device, and two patients developed DIC, thus highlighting the increased risk of coagulopathy and bleeding in these patients. Poor healing may occur, possibly complicated by poor bone quality. Isolated osteoporotic bone in the area of KTS is associated with pathological fractures. Redondo et al 19 recommended prophylactic bisphosphonates to prevent these fractures but no prospective studies have evaluated the effectiveness of this treatment strategy. 16 Despite the surgical risks, pain and disability can be improved significantly by operative intervention.15,18
With increasing availability of genetic testing, the term ‘Klippel-Trenaunay syndrome’ may soon become obsolete. In the 2018 ISSVA classification, most patients previously diagnosed with KTS would now be diagnosed with ‘PIK3CA-related overgrowth spectrum’ (PROS). 14 Due to this change in terminology, some of our recent patients were not included in this study. While it is helpful to examine a group of disorders based on common genetic mutations, there is broad phenotypic variation within PROS, which may urge some to retain sub-classification (such as KTS) within the group.
This study has several limitations, including the use of retrospective chart review, in which it can be difficult to apply stringent diagnostic criteria with the limited information present. While many patients were monitored longitudinally, some patients did not have long-term follow-up. However, every effort was made to identify outside procedures by reviewing the initial consultation notes as well as each patient's past surgical history. The study was strengthened by the large cohort of patients available for study, the fact that the Mayo Clinic has long served as a referral centre for KTS and by the extensive photodocumentation within the medical record.
Prospective studies are needed to better understand the clinical phenotype, genotyping and natural history of patients with vascular malformation overgrowth syndromes. It is crucial that paediatric orthopaedists understand the severity and range of conditions that are associated with KTS, in order to best treat these complex patients. Patients with symptoms related to lymphatic malformation and/or lower extremity overgrowth should be closely monitored by orthopaedists, due to the increased risk of orthopaedic conditions.
Footnotes
All other authors report no conflict of interest.
HN: Chart review, Data collection, Manuscript preparation.
BSS: Content expert on orthopaedic questions, Manuscript preparation.
KRA: Chart review, Data collection, Manuscript preparation.
AAS: Study design, Content expert on orthopaedic questions, Manuscript preparation.
DD: Study design, Content expert on Klippel-Trenaunay syndrome, Manuscript preparation.
MT: Study design, Content expert on Klippel-Trenaunay syndrome, Manuscript preparation.