
Abstract
Squamous cell carcinoma is the most common mucosal malignancy of the head and neck. Adenoid pseudo-angiosarcomatous SCC is a rare variant occurring commonly in the skin of the head and neck. However, involvement of oral cavity is extremely rare, with only few case reports in the English literature. Morphologically, the tumor shows marked acantholysis, with anastomozing channels mimicking vascular neoplasms. This variant represents a diagnostic challenge for pathologists, and immunohistochemical analysis remains essential for an accurate diagnosis. Herein, we describe the case of a pseudovascular SCC of the oral cavity in a 67 years old man with a brief revue of the literature to raise awareness on this rare variant; presenting diagnostic difficulties.
Introduction
Squamous cell carcinoma SCC accounts for the most common mucosal malignancy of the head and neck (over 90% of all neoplasms). 1 Several histological variants have been described, including adenoid pseudo vascular/pseudo-angiosarcomatous SCC; which is a rare but well defined entity. 2 Involvement of oral cavity is extremely rare, with only few case reports in the English literature. 2 Morphologically, the tumor shows marked acantholysis, with anastomozing channels mimicking vascular neoplasms. 3 This variant constitutes a diagnostic challenge for pathologists, and immunohistochemical analysis remains essential for an accurate diagnosis, especially when squamous differentiation is absent. Herein, we describe the case of a pseudovascular SCC of the oral cavity in a 67 years old man with a brief revue of the literature to raise awareness on this rare variant; presenting diagnostic difficulties.
Case Presentation
A 67 years old man presented to the department of maxillofacial surgery with a 2 months history of a painful mass on his left inner cheek, associated to bleeding. Except his smoking history, he had no major medical troubles. Upon oral examination, the lesion was hyperemic, ulcerated with an easily bleeding surface. The overlying skin showed an angiomatous appearance (Figure 1). A first biopsy was performed in another institution, revealing a hemangioendothelioma. Computed tomography (CT) showed an ill-defined, tissular mass, with heterogenous enhancement, measuring 78 × 54 × 38 mm (Figure 2). The tumor was infiltrating the infratemporal fossa and the mandible, with multiple homolateral cervical adenopathies. Due to the discordance between pathological and radiological findings, a second biopsy was performed, and the sample was sent to our department for histological examination. Morphologically, the tumor consisted of atypical epithelioid cells, with hyperchromatic nuclei, prominent nucleoli showing multiple mitosis. Neoplastic cells arranged in trabecula and irregular anastomosing channels due to tumor cell discohesiveness (Figure 3). Serial sections through the specimen failed to demonstrate any squamous-type differentiation. The morphology was suggestive of an angiosarcoma. A large panel was made on immunohistochemistry, showing positivity for epithelial markers (AE1/AE3; EMA, p63, p40) with negative vascular markers (CD31, CD34, erg) (Figure 4). Thus, the diagnosis of pseudovascular adenoid SCC was made. The patient was referred to oncology department, because of the locally advanced stage of the disease. The follow-up period is too short (3 months), to evaluate the survival.

Clinical findings of the mass, arising in the internal surface of the left cheek.

CT scan imaging showing an infiltrative heterogenous mass of the left cheek (white star).

PASCC histological features: pseudo vascular pattern: (A) hematoxylin and eosin, ×100 and (B and C) hematoxylin and eosin, ×400 (black arrow: pseudovascular channel).
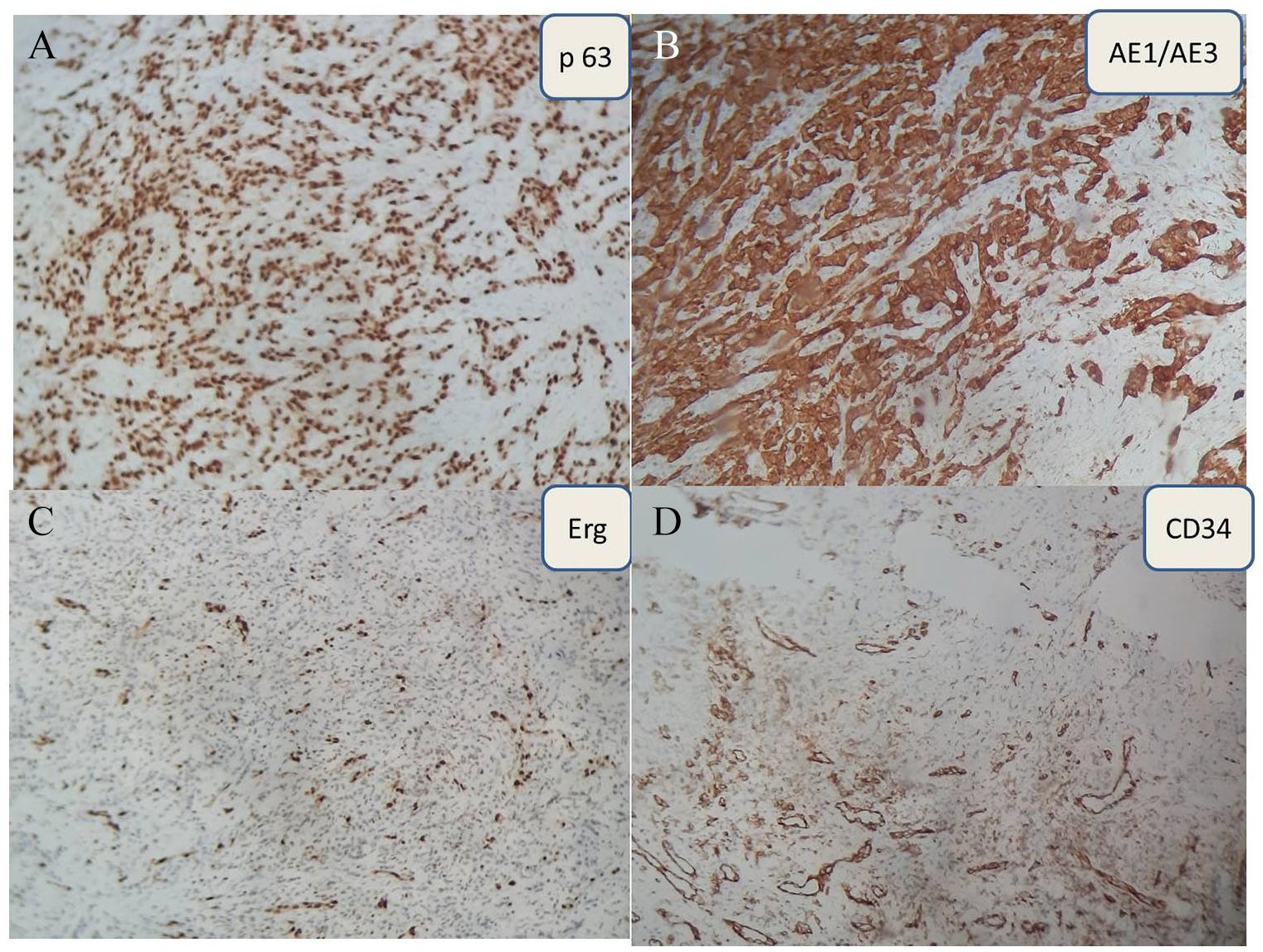
PASCC immunohistochemistry: the carcinomatous cells are p63 positive (A), AE1/AE3 positive (B), erg negative (positivity seen in stromal vessels) (C), CD34 negative (positivity in stromal vessels) (D) (immunohistochemical stain, ×100).
Discussion
Conventional-type SCC is by far, the most common malignancy in the upper aerodigestive tract. Histological variants include: verrucous SCC, spindle-cell SCC, papillary SCC, basaloid SCC, adenoid pseudo vascular SCC, lymphoepithelial carcinoma, and adenosquamous carcinoma. Although less frequent, the recognition of SCC’s subtypes remains essential because of their prognostic implications. 3 Pseudo-vascular adenoid SCC (PASCC) represents a rare variant of adenoid SCC; the latter is defined by a pseudoglandular pattern with marked acantholysis. 4 To the best of our knowledge, only few cases of PASCC in the oral cavity have been reported in the English literature to date.2,3 It mainly occurs in old patients (the peak incidence is the sixth decade) with male predilection, it clinically presents as a rapidly growing and infiltrating masses; as in the present case. 5 On histology, ASCC is classified into 3 categories: (1) the common or ordinary subtype consisting of acantholytic atypical keratinocytes arranging in a solid pattern without specific structures, (2) the pseudoglandular/pseudovascular subtype which is defined by the presence of vascular spaces containing red cells, and (3) pseudoangiosarcomatous subtype, which shows atypical cells, arranging in vascular structures resembling atypical endothelial cells. 4 Hence, morphologically, PASCC constitutes a real mimicker of angiosarcoma. In addition, the neoplastic stroma shows marked vascularization, which raises the similarity with vascular neoplasms. 6 The diagnosis becomes more challenging when epidermoid differentiation lacks or is masked by the pseudo vascular architecture. Uncommon histological findings include: dyskeratosis and reactive firbosis.2,5 On cytology aspirates, PASCC shows atypical epithelioid cells, with finely vacuolated cytoplasm, oval to spindled nuclei and prominent nucleoli. These cells may be sparsed or arrange in syncytial pattern. 7
The definite diagnosis requires immunohistochemistry, neoplastic cells express cytokeratins, epithelial membrane antigen, and p63; while vascular markers including CD31, CD34, and von Willebrand factor, are negative. 1 The main differential diagnosis to rule out is angiosarcoma, especially on biopsies, where only the pseudovascular component might be represented and PASCC cannot be distinguishable from an angiosarcoma. Other diagnosis to consider are: adenosquamous carcinoma and mucoepidermoid carcinoma of minor salivary gland origin; when glandular pattern is present. 8 Thus, the diagnosis is based on a careful histological and immunohistochemical analysis. Given the fact that PASCC have only been reported in some cases, its prognosis remains unclear. For some authors, PASCC shares with adenoid SCC the same prognosis with a more aggressive biological and clinical behavior than conventional SCC. In conclusion; we have reported the clinical and histopathological features of this rare SCC subtype. The authors believe that the diagnosis of SCC’s variants has to be considered in the oral cavity, and epithelial markers are mandatory before ruling out the diagnosis of SCC.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Note
Guarantor is the corresponding author.
Author’s Contributions
All authos have read and approved final manuscript. S.Derqaoui wrote the manuscript; I boujida elped writing the paper; Z.sayad provided clinical information; H Elouazzani and NCherrad supervised the work and made the final corrections.
Informed Consent
Informed consent was obtained from the patient.