
Abstract
Hepatocellular carcinoma is a prevalent malignant tumor affecting the liver, and surgical resection and liver transplantation are the primary treatment options for early-stage HCC patients. However, the presence of benign hepatic tumors with similar imaging characteristics to HCC poses challenges in diagnosing and treating the disease, often resulting in misdiagnosis and inappropriate treatment. This case report presents a 52-year-old female patient who exhibited space-occupying liver lesions on abdominal CT and MRI scans. Based on pathological sections from other hospitals, liver malignancy was highly suspected, and hepatocellular tumor was diagnosed preoperatively. But the tumor markers of the patient were all within the normal range. After evaluating the overall condition of the patient, we finally chose the diagnosis and treatment of dissection and partial hepatectomy. Surprisingly, the final diagnosis of postoperative pathology was sclerosing hemangioma. The patient recovered well and was discharged 2 weeks later. Hepatic sclerosing hemangioma is an extremely rare disease that can be easily mistaken for malignant liver tumors due to absence of typical imaging presentations. The diagnosis also needs to be differentiated from other benign tumors, such as liver adenoma and liver abscess, according to the medical history, symptoms, and auxiliary examinations. Therefore, special attention should be given to the diagnosis and treatment of sclerosing hemangioma.
Introduction
Hepatic sclerosing hemangioma is an infrequent benign condition, with sclerosis believed to be a potential complication of common liver hemangiomas. 1 While typical hemangiomas can be reliably identified by using ultrasound, CT, and MRI, sclerosing hemangiomas exhibit a variety of other degenerative changes that often obscure the underlying nature of the disease. 2 Patients with sclerosing hemangioma frequently undergo partial hepatectomy as the imaging presentation is often misinterpreted as primary hepatocellular carcinoma. Pathological findings after surgery are necessary to establish an accurate diagnosis.1,3 Further consideration should be given to the standardization of diagnostic and treatment approaches for sclerosing hemangioma, aiming to prevent unnecessary invasive surgical procedures for patients with this condition.
Case presentation
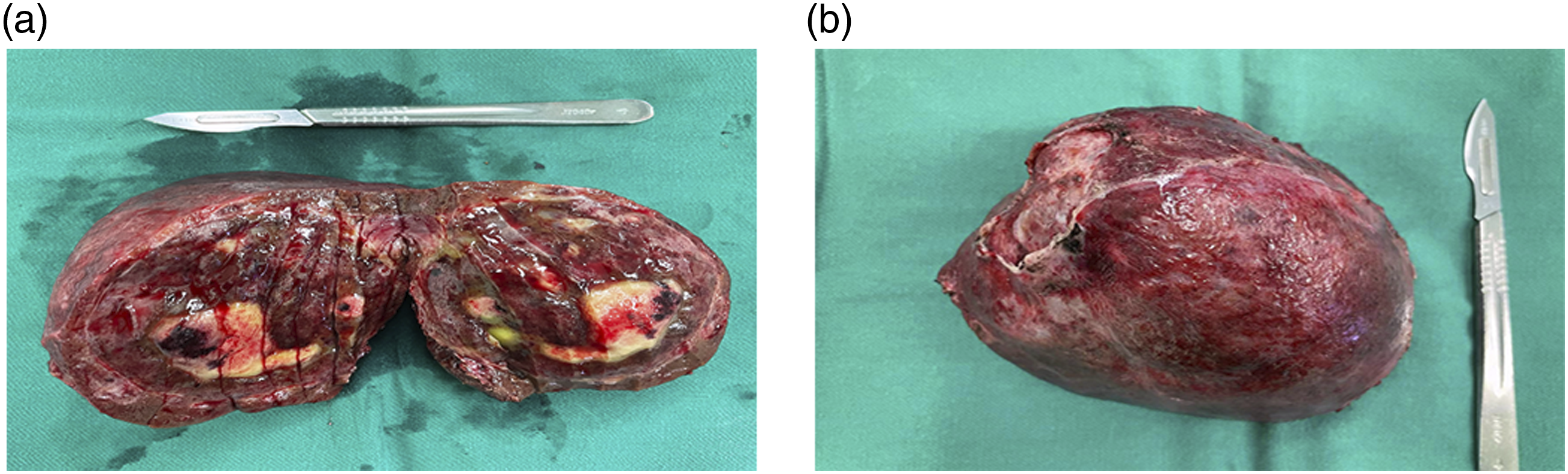
A middle-aged woman aged 52 was found to have multiple occupying lesions in the liver on CT scan during her hernia repair surgery at an outside hospital. The patient was referred to our hospital with pathological tissue sections from an outside liver puncture. On admission, the patient experienced mild abdominal discomfort symptoms, primarily abdominal distension. Laboratory tests on admission indicated significantly elevated levels of alanine transaminase: 361.8 U/L, aspartate aminotransferase: 475.4 U/L, alkaline phosphatase: 127 U/L, and gamma-glutamyl transpeptidase: 52.8 U/L. Conversely, bilirubin indicators and tumor markers including methemoglobin, carcinoembryonic antigen, glycoantigen 19-9, and hepatitis B virus DNA results fell within the normal range. CT scans revealed hypodense foci in the right lobe of the liver measuring approximately 9.7*8.6 cm, accompanied by poorly defined hypodense foci in the left inner lobe of the liver. MRI findings suggested the presence of three occupying lesions in the liver, with the largest mass measuring approximately 89*74 mm. The mass exhibited a predominantly mixed signal shadow on long T1-long T2 sequences along with multiple segregated enhancing shadows at the edge and inside. Significant enhancement was observed during the arterial phase and continuous enhancement during the venous and delayed phases. Other imaging observations included an 11 mm nodule in the s4 segment of the liver with delayed enhancement and a tiny round long T2 signal without significant enhancement (Figure 1). Based on the above imaging examinations, a preliminary diagnosis of neoplastic lesion (sarcoma), hepatocellular carcinoma, intrahepatic metastasis of hepatocellular carcinoma or atypical hemangioma was made. Liver biopsy revealed a large area of coagulated necrotic tissue surrounded by vascular granulation tissue proliferation, inflammatory cell infiltration, and iron-containing hemoglobin deposition. Exploratory laparotomy was performed, revealing multiple intrahepatic occupancies. After the resection of the liver mass, the excised specimen was a solid, soft, circular mass with a complete capsule from the right lobe of the liver, measuring 10*6.5*6.5 cm. The cut surface was grayish-white, partially grayish-yellow. Additionally, a grayish-white nodule with a diameter of 0.4 cm was identified in the inner left lobe of the liver (Figure 2). Moreover, another grayish-white nodule measuring 2.5*2.5*1 cm was located beneath the falciform ligament of the liver. Intraoperative rapid pathology indicated a spindle cell lesion with interstitial small vessel hyperplasia in the right posterior lobe of the liver, fibrous tissue hyperplasia with chronic inflammatory cell infiltration in the left inner lobe of the liver, and a tumor of vascular origin in the mass below the sickle ligament. Postoperative conventional pathology suggested vascular-derived lesions but failed to confirm the disease definitively. Therefore, immunohistochemical staining was performed on the sections, revealing positive CD31, CD34, and ERG staining in all three lesions, leading to the final diagnosis of sclerosing hemangiomas. The patient’s postoperative recovery was uneventful, and she was discharged on the 11th day after surgery. An abdominal magnetic resonance imaging scan of a 52-year-old woman showed multiple space-occupying lesions in the liver. The irregular mass in the right lobe of the liver showed multiple separate enhancement shadows in the interior and margin of the mass, with continuous enhancement of the arteries, veins, and delayed phase. The gross manifestation of a large mass in the right lobe of liver was 10*6.5*6.5 cm, the capsular was complete, and multiple gray and white areas were visible on the tumor section.
Discussion
Literature review of sclerosing hemangioma cases in the liver.
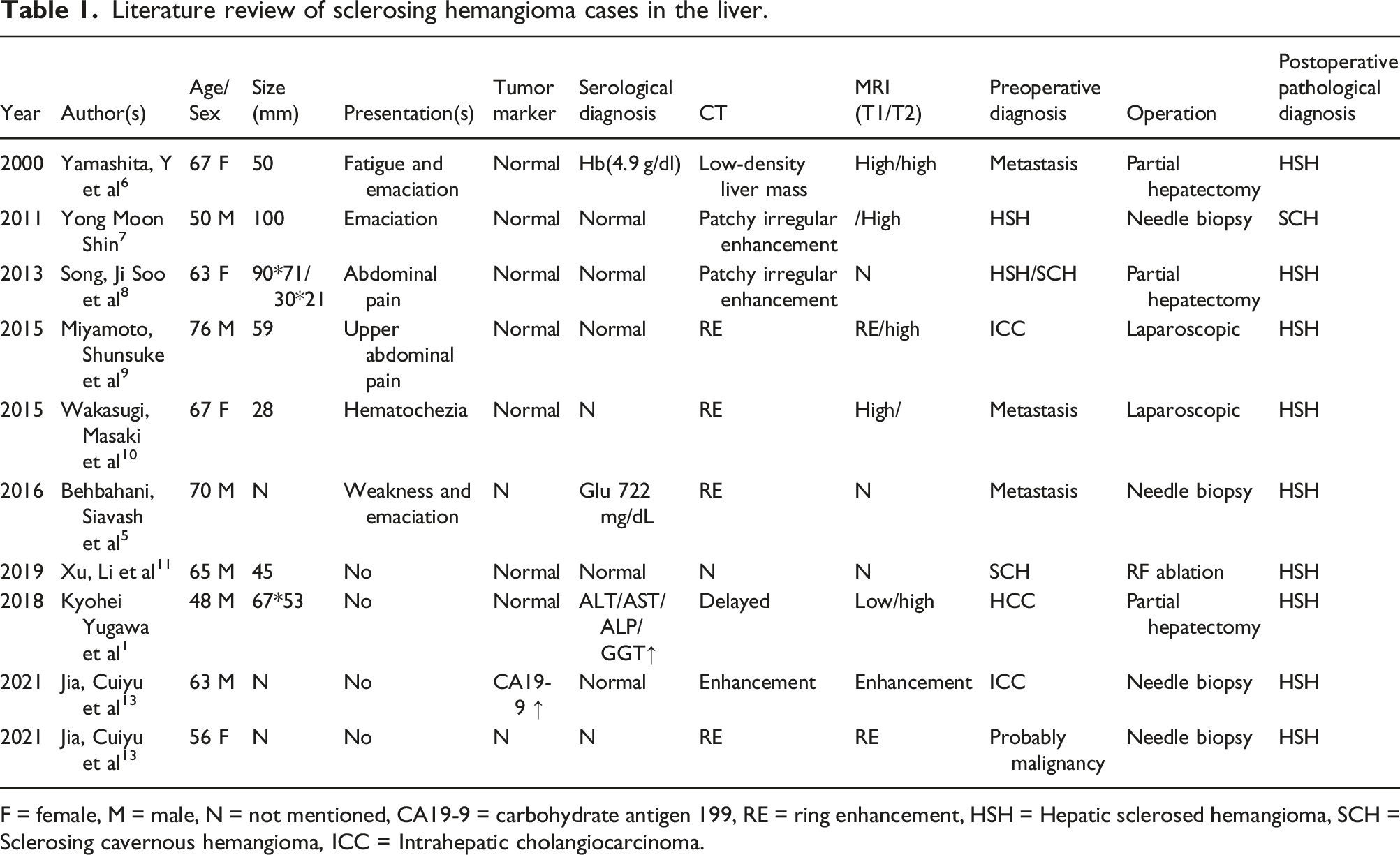
F = female, M = male, N = not mentioned, CA19-9 = carbohydrate antigen 199, RE = ring enhancement, HSH = Hepatic sclerosed hemangioma, SCH = Sclerosing cavernous hemangioma, ICC = Intrahepatic cholangiocarcinoma.
Conclusion
Accurate preoperative diagnosis is essential for the treatment of liver tumors. Some rare benign diseases, such as sclerosing hemangioma, which have confusing imaging features, still cannot be ignored in the differential diagnosis of malignant liver masses. For the diagnosis of such rare diseases, the help of pathological examinations is indispensable, and a comprehensive analytical consideration of the disease can help us in the final characterization.
Footnotes
Acknowledgements
The authors would like to thank the National Natural Science Foundation of China for funding this work.
Author contribution
Xinyu Zhan and Yiyun Gao were responsible for case investigation and writing manuscripts. Haoming Zhou and Ping Wang analyzed and interpreted the patient data of laboratory and imaging tests. Jian Xu and Dongming Wu performed clinical follow-up.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the National Nature Science Foundation of China (82071798).
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for the publication of this case report.