
Abstract
Actinomycosis is a rare chronic granulomatous infection caused by Actinomyces species. We report the case of a 47-year-old man with no previous medical history, who presented with a slowly growing abdominal mass extending to the abdominal wall, initially mimicking a malignant tumor. A diagnosis of an Actinomyces abscess was confirmed through surgical resection and histopathological examination. This case is presented to highlight the morphological characteristics and emphasize the diagnostic difficulties of this disease.
Introduction
Actinomyces is a gram-positive, anaerobic, filamentous bacteria, with Actinomyces israelii being the most common species. These bacteria normally colonize the oral, digestive, and urogenital tracts but can become pathogenic in cases of tissue ulceration or necrosis, leading to the formation of respiratory, cervicofacial, or abdominopelvic abscesses. Abdominal actinomycosis is rare, particularly affecting the proximal colon. Extension to the abdominal wall is atypical and even rarer, with only about 30 cases reported in the literature. 1
Case Report
A 47-year-old Tunisian man, with no medical or surgical history and no exposure to tobacco, drugs, or alcohol, presented to the general surgery department with a slow-growing abdominal mass in the epigastrium that had been noticed 4 months earlier. He had no other symptoms, particularly no weight loss, fever, or changes in bowel habits. The patient appeared generally well, and his vital signs were normal.
On physical examination, the patient had a mass measuring approximately 10 cm × 5 cm, which was immobile and located in the epigastric region, with tenderness on palpation. Laboratory investigations revealed an elevated total white blood cell count of 14 000/µL (normal range: 4000-11 000/µL) and an increased level of the inflammatory marker C-reactive protein at 220 mg/L (normal range: 0-3 mg/L).
In addition, a colonoscopy was performed, which was found to be normal. HIV testing was not performed. Abdominal and pelvic computed tomography (CT) with contrast revealed a large, heterogeneous mass within the anterior abdominal wall, measuring 10 cm in greatest diameter, with extensive inflammatory changes in the surrounding fat and regular thickening of the transverse colon (Figure 1).

Abdominopelvic computed tomography with contrast revealing an ill-limited, infiltrative mass within the anterior abdominal wall, adherent to the posterior rectus sheath, transverse colon, and stomach.
Abdominal magnetic resonance imaging revealed an infiltrative mass adherent to the posterior rectus sheath, transverse colon, and stomach, and excluded any colonic fistula (Figure 2). The multidisciplinary decision, made by radiologists, surgeons, and gastroenterologists, was to proceed with surgical resection of the mass.

Abdominal MRI.
The patient was admitted to the hospital 1 day prior to surgery for preoperative preparation, which included laboratory tests and intravenous hydration. During the operation, the mass was resected along with the posterior rectus sheath, 15 cm of the transverse colon, and the gastric antrum. A stapled lateral colo-colonic anastomosis was performed, and a lateral stapler was applied to the stomach. The anterior abdominal wall was closed after anterior abdominal component separation with interrupted sutures. The specimen was sent for histopathological examination.
Macroscopic evaluation revealed dense fibrosis that predominantly infiltrated the mesocolon, causing adhesion to the stomach and anterior abdominal wall, which mimicked a true tumor (Figure 3).

Gross examination: A white, dense fibrosis that infiltrate the mesocolon, with adherence to the stomach and anterior abdominal wall.
Microscopic examination of the mass showed extensive fibrosis with steatonecrosis and a significant pleomorphic inflammatory infiltrate, including lymphocytes, neutrophils forming foci of suppuration, and foreign body granulomas. These abscesses and granulomas frequently contained sulfur granules with aggregates of filamentous bacteria, PAS-negative, modified acid-fast stain-negative, consistent with actinomycosis (Figures 4 and 5). Fibrosis and inflammation extended into the gastric wall and abdominal wall muscle. The lymph nodes exhibited hyperplasia. No epithelioid granulomas with necrosis or atypical cells were observed.

Histological feature: Aggregates of Actinomyces with pleomorphic inflammatory infiltrate (HE*25).
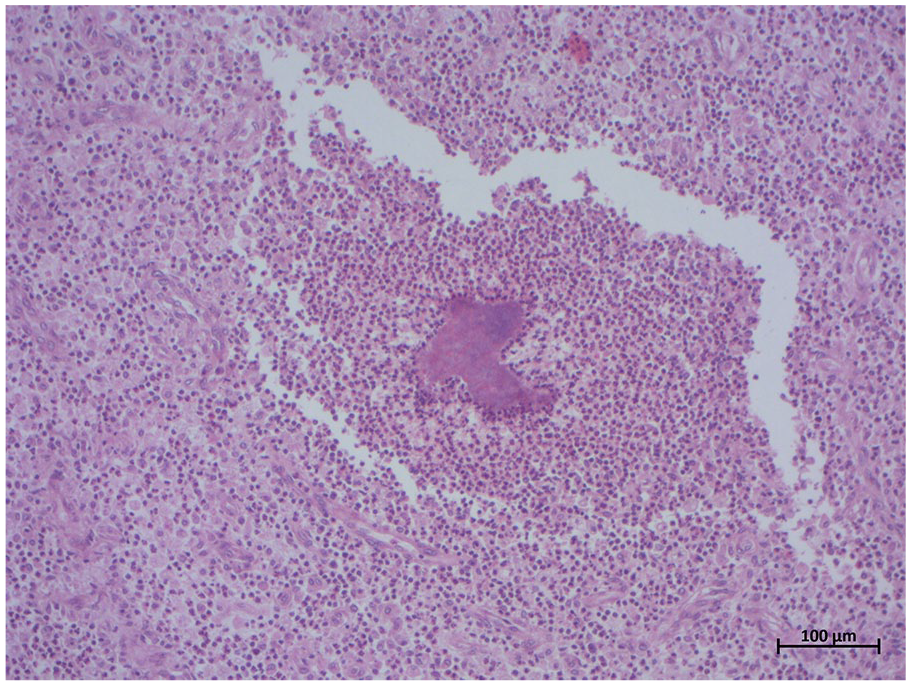
Histological feature: Aggregates of Actinomyces with pleomorphic inflammatory infiltrate (HE*100).
After surgery, the patient remained in the hospital for close monitoring and observation. On the seventh day of hospitalization, he developed a fever, abdominal pain, and a rigid abdomen on examination, which were indicative of postoperative peritonitis. During reoperation, the surgeons discovered a leakage of the colo-colonic anastomosis. A double colonic stoma was created. The peritoneal fluid cultures grew a mixture of polymicrobial gram-negative and anaerobic bacteria, including Escherichia coli and Clostridium species. Blood cultures revealed growth of E coli. The patient died 48 hours later from septic shock and multiorgan failure.
Discussion
Abdominal actinomycosis is rare, accounting for only 20% of all cases of actinomycosis. It typically presents as a slow-growing mass, similar to the case we report here, and may be associated with other symptoms including altered bowel habits, anorexia, vomiting, cramping pain, weight loss, fever and night sweats. In some cases, it can rarely lead to bowel perforation.2,3
There are some predisposing or risk factors such as immunocompromised states, bowel surgery, ingestion of a foreign body, and the presence of intrauterine devices, which are essentially associated with abdominopelvic actinomycosis.4,5 However, in most cases, the etiopathogenesis remains unknown, as is the case in our report.
Computed tomography is essential in determining the size and extent of the disease; it typically reveals an infiltrative mass with irregular density and contrast enhancement. However, these features are also seen in other diagnoses such as Crohn disease, abdominal tuberculosis, and malignant tumors, making diagnosis challenging.1,3
The final diagnosis is usually confirmed by histological examination after resection of the mass. Preoperative diagnosis occurs in only 17% to 20% of cases. 1 Computed tomography–guided biopsy or fine needle aspiration (FNA) may be useful in avoiding unnecessary surgery and obtaining a histological diagnosis. However, false-negative results can occur due to nonrepresentative samples that show only nonspecific inflammation. 3
In our case, a CT-guided biopsy may have been helpful. However, due to concerns about potential malignancy, we opted for surgery. Frozen section examination during surgery could also have been useful to avoid unnecessary mutilating surgery. 2 In our case, the abdominal mass was initially suspected to be a malignant tumor before surgery. Due to this misdiagnosis, no frozen section examination was performed.
Microbiological analysis of sulfur granules, which represent macrocolonies of Actinomyces obtained from aspiration of purulent collections, is highly suggestive of the diagnosis. However, they are not pathognomonic of actinomycosis and may also be seen in nocardiosis, botryomycosis, and Aspergillus infections.3,6 The use of histochemical stains facilitates the differentiation of these microorganisms. The periodic acid-Schiff (PAS) stain helps distinguish Nocardia and Actinomyces (typically PAS-negative) from true fungal hyphae (PAS-positive). In addition, a modified acid-fast stain is effective in differentiating between Nocardia (which are generally modified acid-fast positive) and Actinomyces (which are not). 7 In our case, microbiological examination was not performed because the mass was fixed in formalin. However, histochemical staining was consistent with actinomycosis.
Colonoscopy was normal and not helpful in this case because the lesion was extramucosal, but it was essential to exclude colitis or a neoplastic process. In some cases, colonoscopy may show luminal narrowing or nodules with central umbilication, which are associated with chronic inflammation and fibrosis of the bowel wall. 6
The treatment of choice in uncomplicated cases is prolonged antibiotherapy, usually with high doses of intravenous penicillin for 2 to 6 weeks, followed by oral penicillin or amoxicillin for 6 to 12 months.8,9 For patients with penicillin allergy, other effective antibiotics including tetracycline, erythromycin, chloramphenicol, clindamycin, and imipenem can be used. In complicated cases, combined surgery and antibiotics are recommended and this approach achieves a cure in about 90% of cases.8,9
Conclusion
Abdominal actinomycosis should be considered as a differential diagnosis in patients presenting with an abdominal mass and vague symptoms. Imaging studies, microbiological analysis, CT-guided biopsy, and FNA can aid in diagnosis and help avoid unnecessary invasive surgical interventions that may lead to serious complications. Medical treatment should be attempted first in uncomplicated cases, while surgery should be reserved for complicated or persistent disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient’s parents for the publication of their anonymized information in this article.