
Abstract
Background
Smoking rates in Switzerland remain disproportionately high among people with a migration background and with a low socioeconomic status. These groups face multiple access barriers and are often labeled as “hard-to-reach”, underserved communities or disadvantaged in public health literature. Cessation strategies that are inclusive and setting-sensitive remain scarce and under-evaluated for these vulnerable populations.
Objectives & Design
The one arm pre-post non-clinical trial study aimed to implement and analyze a setting- and milieu-sensitive as well as a linguistically adapted community-based smoking cessation group intervention for disadvantaged groups with a migration background in Switzerland, and to assess its reach, acceptability, and behavioral effects.
Methods
A two-part workshop program, each lasting two hours, was delivered between 2022 and 2024 to 82 preexisting community groups in their native language across Switzerland. The intervention was conducted in 12 languages and embedded in daily life settings such as clubs and associations. Data was collected in six selected languages from 42 groups through telephone surveys at baseline (T1) and follow-up (T2, three months later). Key indicators included smoking status, quit attempts, reduction in daily cigarette consumption, and the activation of smoke-free social norms. Descriptive statistics were computed, and chi-square tests and paired-samples t-tests were used to analyze changes between baseline (T1) and follow-up (T2).
Results
Out of 795 participants from the 42 groups included in the analysis, N=184 completed the baseline survey, and 99 could be followed up at T2. Among smokers, 23% had quit cigarette smoking by follow-up, and 50% of those still smoking had made at least one quit attempt. Cigarette consumption decreased significantly. Over a quarter of non-smoking participants reported actively encouraging smokers in their environment to quit or reduce smoking, indicating normative diffusion through strong social ties.
Conclusions
The findings suggest the potential of short, community-embedded interventions may hold considerable potential. When tailored to the specific social target groups and delivered in everyday environments, such programs may achieve relevant individual outcomes and promote broader shifts toward smoke-free norms within disadvantaged communities.
Keywords
1. Introduction
Tobacco use remains one of Switzerland’s major public health challenges, with approximately 24% of the population smoking cigarettes, well above the European average.1,2 While overall prevalence has declined, socially disadvantaged populations and individuals with a migration background continue to smoke at disproportionately high rates.3,4 These groups not only bear a heavier tobacco-related disease burden but also face significant barriers in accessing existing prevention and cessation services.5-8
Multiple factors contribute to this disparity. People with lower socioeconomic status and limited language proficiency are less likely to participate in mainstream programs.5,9-11 Limited awareness, lack of trust in health services, and the absence of specific services within their community setting, educational level, and linguistically adapted resources further restrict access.12-14 Also, the often more challenging living conditions and reduced opportunities in these populations, such as unstable employment, precarious housing, and limited social mobility, can further hinder engagement with prevention efforts. Even when low-threshold, setting-sensitive interventions are accepted, the transition to regular cessation support often fails, highlighting structural gaps in service integration.
In addition, tobacco use continues to be socially accepted in many environments. In certain communities, smoking is deeply embedded in everyday life and serves as a social and emotional coping strategy as well as a connection factor among individuals.15,16 This context makes quitting more difficult and undermines efforts to establish non-smoking as a social norm. The combined impact of these social and structural determinants reinforces health inequalities, underscoring the need for targeted, community-based interventions.
With nearly half of the Swiss population having a migration background, and approximately 8.2% affected by poverty and 13.7% by low educational level – all factors strongly associated with smoking – the issue of tobacco-related health inequality is of particular concern in Switzerland.3,17-21 It is estimated that around 10% of the population experiences multiple, intersecting forms of disadvantage, making inclusive and targeted interventions a public health priority. 22
However, populations experiencing intersecting forms of disadvantage, such as those affected by poverty, limited education, and migration, are not only at higher risk for tobacco use but are also significantly harder to reach through conventional public health efforts. Due to factors such as institutional mistrust, language barriers, and precarious life circumstances, these groups are often underrepresented in both prevention programs and related research.23,24 This has also led to their classification in literature as “hard-to-reach populations” or also as underserved communities. As a result, both intervention delivery and accompanying effectiveness research face considerable challenges in terms of participation, retention, and measurement reliability. These structural and psychosocial barriers must be explicitly considered when designing and evaluating smoking cessation initiatives aimed at vulnerable populations.
Recognizing this, the Swiss Tobacco Prevention Fund (TPF) has supported language- and socio-cultural-specific cessation programs for so-called “hard-to-reach populations” (underserved communities) (and among them those with migration background) since 2006. Previous projects were delivered in group settings and specifically tailored to address structural disadvantages, including limited education, a lack of local language skills, and restricted financial resources.15,25-30 However, their delivery, based on multiple in-person sessions and small group formats, made them relatively resource-intensive. Moreover, they were implemented exclusively on-site, which posed challenges during COVID-related restrictions and limited scalability across diverse group settings and locations. In addition, they were primarily conceptualized for relatively small groups and were limited to a few languages, not adequately reflecting the linguistic and migration diversity of the Swiss population. Furthermore, the interventions focused solely on smokers, without involving non-smoking family members or friends who could potentially support cessation efforts. As a result, there was a growing need to optimize the reach and cost-efficiency of such interventions while maintaining their accessibility and effectiveness for vulnerable groups.
To respond to these needs, the project “Gemeinsam rauchfrei!” (“smokefree together!” https://www.gemeinsam-rauchfrei.ch/) was implemented between 2022 and 2024. It aimed to provide an innovative, setting-sensitive, and multilingual approach to tobacco prevention and cessation targeting disadvantaged population groups with a migration background in Switzerland. The aim of this study was to examine the effectiveness of a community- and language-sensitive smoking cessation workshop for disadvantaged and migrant populations in Switzerland, and to examine its reach, participant engagement, and the changes it has fostered in smoking-related attitudes and behaviors.
2. Methods
2.1. Study Design
This study investigated the quantitative outcomes of a smoking cessation intervention program tailored to the settings and milieus of socioeconomically disadvantaged migrant populations in Switzerland (low financial resources, low local language skills, low educational level) by means of one arm pre-post non-clinical trial. The intervention was implemented as a low-threshold, relationship-community-based group approach, embedded in participants’ everyday environments and delivered in their native languages within the group settings of already pre-existing groups (e.g., clubs, social meeting points, churches, mosques).
While the overall project included both quantitative and qualitative components, the present study focused exclusively on quantitative data. Qualitative findings, with a focus on the project’s feasibility, gathered through semi-structured interviews and focus groups, were not included in this article, as they had already been analyzed and published after one-third of the workshops had been completed. 6 Additional qualitative data collected later largely confirmed the earlier findings and did not yield substantially new insights regarding participant experiences or program processes. 31
2.2. Intervention
The goal of the intervention was not to facilitate immediate cessation attempts (to ensure that those who are not aiming to stop smoking at the moment also participate in the workshops), but rather to inform participants about the health risks of smoking and secondhand smoke, introduce evidence-based cessation strategies, and reduce barriers to accessing pharmacological support. Given the pre-existing group setting, participants were not required to be smokers themselves; however, the intervention was designed with the aim that at least half of the group members would be current smokers.
The intervention aimed to reach 80 pre-existing (but not predefined) groups of 15 to 20 individuals by offering them two thematically structured workshops called “Smoking harms” and “How do I quit?”, each held in the participants’ native language and with a duration of two hours.
For this number of groups, no formal a priori power calculation was conducted. Instead, the planned sample size was pragmatically derived from the research team’s extensive implementation experience with earlier cessation programs, specifically Tiryaki Kukla and Jeto pa Tym. 30 Between 2014 and 2019, these projects delivered 73 information sessions and 37 six-session cessation courses for Turkish-speaking communities, and 48 information sessions and 21 six-session cessation courses for Albanian-speaking communities, amounting to 151 group-based intervention formats. Although implemented in only two language groups, these projects demonstrated both the feasibility of delivering smoking cessation interventions at scale within migrant communities and the effectiveness of structured multi-session courses in reducing smoking rates among participants. In contrast, the present study used a much shorter, less resource-intensive two-session two hours each workshop format, and extended the intervention to additional language communities. Based on this prior experience and the increased scalability of the new format, a target of approximately 80 pre-existing groups was considered realistic and feasible for the implementation period (less than 3 years). The study therefore followed a feasibility-driven sampling approach rather than a power-based recruitment strategy. 30
The first workshop included information on the health consequences of smoking and passive smoking, the addictive nature of nicotine, and the social and financial impacts of tobacco use. The second workshop focused on evidence-based cessation strategies, including defining a suitable time point to stop (e.g., “critical life transitions”) craving management techniques, stress coping without smoking, the use of nicotine replacement therapy, and local cessation support services. The workshops were delivered either on site or online, depending on the preferences and infrastructure of the participating organizations, and took place one week apart. The spoken language in both sessions was tailored to the educational level and socio-economic situation of the participants. Physicians conducted the first workshop, while the second workshop was led by trained smoking cessation coaches (RCCs) - both from the same language and migration background communities as the respective group. This approach allowed for high accessibility and credibility.
Workshops’ content included evidence-based information on the health risks of smoking and secondhand smoke, as well as practical guidance on cessation strategies, craving management, and the use of nicotine replacement therapy (NRT) or comparable products. Participants who expressed readiness to quit smoking were offered a free starter package of NRT products - typically including three nicotine patches or 30 pieces of nicotine gum.
2.3. Participants and Recruitment
Groups were recruited for the workshops through existing networks between fall 2022 and summer 2024 among community organizations, migrant associations, and religious institutions. All adult participants in the workshops were invited to participate in the assessments of the study.
The project employed a purposive, community-based sampling strategy. The project team collaborated with key individuals embedded in these networks – so-called “multipliers” – who played a central role in identifying and mobilizing suitable pre-existing groups. These multipliers were trusted community members with long-standing relationships in their respective communities. Additionally, the participating organizations (e.g., clubs or associations), as well as the multipliers, received an incentive for organizing and coordinating the group workshops on the participants’ side, amounting to CHF 200 for each group and CHF 300 for each group’s multiplier (at the time of the study, around 1:1 in Euros).
The project initially aimed to reach the following language groups: Albanian, Arabic, Bosnian, French, German, Italian, Portuguese, Serbian, Spanish, and Turkish. In 2023, Russian and Ukrainian were added to the program in response to the significant increase in Ukrainian refugees in Switzerland. This newly emerging group was explicitly included in the intervention, as no other tailored prevention services were available to them at the time.
2.4. Questionnaire
A standardized questionnaire was developed to be used in pre-and post-intervention telephone interviews. It was based on previous studies and instruments of smoking cessation and prevention research targeting similar populations.6,26-30,32-35 The prior findings informed us of the selection and formulation of the questions. However, the instruments were not formally validated within each specific ethnic or language group included in this study.
The questionnaire included multiple domains. It assessed participants’ smoking status and smoking behavior, including type, frequency, and context of tobacco use.30,35 It also captured information about smokers in the participants’ social environment and their own readiness to quit smoking. 30 To assess nicotine dependence, selected items from the Fagerström Test for Nicotine Dependence were used. 35 Participants were also asked about alternative behaviors they engaged in to manage stress or emotions instead of smoking. 30 Knowledge about the health risks of active and passive smoking was assessed with adapted items from prior studies. 30 Psychosocial constructs included self-efficacy, measured using a single item from the validated short scale of general self-efficacy (ASKU), as well as health-related action competence, based on subscales developed by Lenartz, focusing on self-control, self-regulation, and personal responsibility.36,37 Perceived social support was measured with items derived from the “social integration” scale by De Jong Gierveld and Van Tilburg. 38 Finally, the questionnaire included sociodemographic items such as age, gender, household structure, nationality, migration background, educational level, and employment status, which were placed at the end of the interview. The domains of the questionnaire are also summarized in Table 3 in the Appendix. First-hand smoking–related questions were assessed only among participants who reported smoking at baseline.
To ensure clarity and relevance to the respective lifeworld of the different subgroups, the questionnaire was pretested with individuals who shared the same migration and language background as the target population. Translations were performed according to established procedures: an initial translation was conducted by a professional translator, followed by an independent back-translation performed by a second translator. Discrepancies between the original and back-translated versions were reviewed and resolved by consensus.
The same questionnaire was used at both measurement points (T1 and T2), with only minor contextual adjustments (e.g., questions about attempts to quit since the first workshop).
2.5. Outcome Measures
Primary outcome measures included pre-post changes in smoking status (e.g., from smoking to non-smoking), the number of cigarettes smoked per day (among daily smokers), and the occurrence of at least one quit attempt during the three-month follow-up period (T2). These outcomes were used to assess the program’s effectiveness in initiating changes in smoking behavior. Secondary outcome measures comprised motivation to quit, knowledge about the health risks of (passive) smoking, awareness and use of cessation strategies, perceived self-efficacy regarding smoking cessation, and perceived social support. For the non-smoking participants, their encouraging activities regarding smoking cessation towards smokers were assessed. Additionally, aspects of action-oriented health literacy were assessed, including self-regulation, personal responsibility, and self-control.
2.6. Data Collection
Anonymous workshop participants (they attended the workshops without the collection of any personally identifiable information) were informed about the telephone interviews during the first session of the workshop. Participants were asked to indicate their cell phone numbers if they were interested in participating. Those who expressed interest were subsequently contacted by the study team and provided with further information about the study purpose, study procedure, confidentiality, data protection, and the voluntary nature of participation at the beginning of each telephone interview. Participants were required to explicitly confirm their consent verbally before any data collection took place. If a participant did not provide consent, the interview was immediately terminated, and no information was recorded. Verbal consent was documented by the interviewer in the electronic interview form using a mandatory consent field, which had to be completed before the questionnaire could proceed.
Upon verbal consent, data were collected via structured telephone interviews at two time points: shortly after the first workshop (T1) and approximately three months after the second workshop (T2). Participants who could not be reached after one to two attempts on different days and at different times were sent a text message, requesting them to suggest a date for an interview appointment. Further contact attempts were discontinued if there was no response to this message either.
Due to the project structure and the considerable costs associated with conducting interviews in multiple languages using trained personnel, only participants from the following six language groups were included in the quantitative study: Turkish, Albanian, Bosnian, Serbian, and Spanish. These groups were informed by evidence from previous studies, program evaluations, and reports, which consistently suggest higher smoking prevalence and tobacco-related risks in these population groups. Ukrainian/Russian-, and Arabic-speaking groups were not included in the study procedures because they were incorporated into the projects’ workshops at a later stage, after the evaluative component with other language groups had already started. Autochthonous or equivalent language groups (e.g., German-, French-, or Italian-speaking populations) were not included in the quantitative evaluation, as they have several other differences to the traditionally defined disadvantaged migrant populations. Digital or written formats were deliberately avoided, as the majority of participants had limited digital literacy and low levels of formal education, as suggested by previous studies. 15 Furthermore, given the predefined evaluation deadlines within the project timeframe, only workshops provided between September 2022 and June 2024 were included in the analysis.
All interviews were conducted by trained research assistants who shared the same linguistic and national backgrounds as the participants. Most of them were Social Work or Psychology students in advanced semesters, or professional intercultural interviewers, and had prior experience in conducting structured interviews.
As a “thank you” for participating in both interviews, participants received a voucher worth CHF 20 for a local retail chain (at the time of the study, around 1:1 in Euros).
2.7. Statistical Analysis
Descriptive statistics were used to summarize sociodemographic characteristics, smoking and related behavior, and other indicators at baseline (T1) and follow-up (T2). Frequencies, percentages, means, and standard deviations were calculated as appropriate. To examine changes in smoking behavior between T1 and T2, differences in smoking status were tested using a chi-square test. Among individuals who reported daily smoking at both time points, changes in the number of cigarettes smoked per day were analyzed using a paired-samples t-test. In addition, the proportion of participants who reported quit attempts within the follow-up period was calculated descriptively. All analyses were conducted using RStudio with R Version 4.4.1. Statistical significance was set at p < .05.
3. Results
Between summer 2022 and fall 2024, a total of 163 workshops were conducted for 82 groups (one group participated in the first workshop only). Due to the anonymous and open nature of the workshops, individual attendance across sessions was not systematically recorded, and participants could join or leave at different points. Based on facilitator reports and average group sizes, we estimate that approximately 1,600 individuals participated across these 82 groups. None of the workshops were held for German or French disadvantaged groups. In line with the predefined timeline and selected languages, the analyzed workshops reached 42 groups, with an average of 18.5 participants per group, totaling 795 participants. The majority of the workshops – 60%- were conducted online, with a duration of around 2 hours each, as planned. Of these, 404 individuals expressed interest in participating in the study by providing their mobile phone number. Ultimately, N = 184 respondents were successfully contacted, gave their consent, and were interviewed at T1, and 99 of them could be followed up to T2. The process flow is illustrated in Figure 1, while the composition of the participating subgroups is presented in Table 1. Overall sociodemographic characteristics of the respondents are presented in Table 2. The average age of the respondents was M = 44.9 (SD = 11.7) years, with a range of 19 to 75 years. 96 (52.2%) were female and 88 (47.8%) were male. Sociodemographic and socioeconomic characteristics of the respondents are summarized in Table 2. Participants flow Composition of the Participants in the Workshops From the Participating Subgroups Note. To ensure participant confidentiality, absolute numbers below five are not reported separately. Respondents Included in the Evaluation Note. To ensure participant confidentiality, absolute numbers below five are not reported separately.


3.1. Smoking Behavior at Baseline (T1)
Among the N=184 respondents interviewed at T1, 43.5% (n=80) reported regular smoking, 13.6% (n=25) smoked occasionally, and 24.5% (n=45) had smoked in the past. Additionally, 18.5% stated they had never smoked. The reported number of cigarettes smoked per day among daily smokers ranged from 2 to 40, with a mean of 15.9 (SD=7.8). A total of 37.1% (n=39) of all smokers reported smoking 20 or more cigarettes per day.
Tobacco dependence was assessed among daily smokers (n=80) using two items adapted from the Fagerström Test for Nicotine Dependence. In total, 21.3% (n=17) of daily smokers reported smoking within five minutes of waking, and an additional 37.1% (n=30) within 30 minutes. A further 14.9% (n=12) smoked within 60 minutes, while 25.2% (n=20) waited longer than one hour after waking.
Regarding the ability to refrain from smoking in places where it is prohibited, 30.3% (n=32) reported difficulty doing so. Nevertheless, 66.0% (n=69) of smokers stated that they were willing or somewhat willing to abstain from smoking in the presence of non-smokers.
Previous quit attempts were common: 73.3% of current smokers (n=77) had tried to quit smoking at least once, with the number of attempts ranging from 1 to 10 (M=2.7; SD=1.8).
Use of novel tobacco products and e-cigarettes was low: only two participants reported using waterpipes (shisha), four used heated tobacco products (e.g., IQOS), and nine reported the use of nicotine-containing e-cigarettes (vapes).
Respondents indicated that many individuals in their close environment also smoked. On average, participants reported that 4.7 (SD=2.5) of their ten most important family members and friends were smokers. Among non-smokers, this number was similarly high, with a mean of 4.2 (SD=2.6). In 72.0% of households - including those of non-smokers - at least one person smoked regularly. The most reported locations for smoking at home were the balcony or garden (n=83), followed by the kitchen (n=18), the living room (n=5), and the bathroom (n=3).
3.2. Changes in Smoking Behavior and Quit Attempts
At T2 (approximately three months after the second workshop), 99 respondents participated in the follow-up assessment. Sociodemographic characteristics and baseline smoking behavior of T2 respondents were largely comparable to the T1 sample (all p’s>.05), except for a slightly higher average age at T2 (M=46.7 years) compared to T1 (M=42.8 years). Only participants who completed both T1 and T2 assessments were included in the following analyses.
From those and among those who identified themselves as current smokers at T1 (n=62), 14 participants reported at T2 that they had quit smoking, representing 22.6%. Two individuals who had not smoked at T1 reported smoking at T2. A chi-square test showed a statistically significant change in smoking status between T1 and T2 (n=99, χ2 = 65.327, df = 4, p < .001).
Of the 50 participants who reported smoking at T2, half (n=25) had attempted to quit smoking in the three months prior to the follow-up. Most of them had made one or two quit attempts during this period.
Among those who smoked daily at both times, the average number of cigarettes smoked per day decreased from 16.9 at T1 to 14.1 at T2. This reduction was statistically significant (n=35, t = 2.37, df = 34, p < .05).
3.3. Intention to Quit Smoking and Self-Efficacy
At T1, 79.0% (n=50) of all respondents reported an intention to quit smoking. Approximately one-third (n=17) had already set a quit date. Among the 50 participants who were still smoking at T2, 78.0% (n=39) expressed a continued intention to quit, although 10.0% (n=5) of them reported a decrease in motivation (from “yes” to “rather yes”). At T2, only five individuals had set a specific date for quitting. Self-efficacy regarding quitting smoking was assessed separately from motivation. At T1, 32.4% (n=20) of smokers reported feeling confident and 26.0% (n=16) rather confident that they could quit smoking. Among those who were still smoking at T2, 8.0% (n=4) reported feeling confident and 22.0% (n=11) rather confident. A total of 40.0% of these participants (n = 20) did not provide an answer to this question at T2.
3.4. Behavior Change Strategies and Social Support
Behavior change competencies were assessed using five items. Significant differences between T1 and T2 were observed in the proportion of respondents who reported being able to follow through with their intentions (item 4: n=59, χ2 = 12.619, df = 4, p = .01) and those who reported having people they could truly rely on (item 5: n=60, χ2 = 14.573, df = 4, p = .005). No significant change was observed for the items assessing stress management.
At T2, most smokers reported at least one concrete strategy or alternative behavior to reduce or replace smoking. Among non-smoking workshop participants, more than half stated they felt competent to support others in quitting. Awareness of available cessation support services was also relatively high, with nearly two-thirds of respondents reporting knowledge of at least one such service.
3.5. Indirect Impact on the Social Environment
At T2, non-smoking participants (n = 49) were asked whether they had succeeded in motivating others in their environment to reduce or quit smoking. A total of 30 participants (61.2%) reported that they had encouraged someone close to them to reduce smoking. Additionally, 13 participants (27%) reported that they had successfully motivated someone in their environment to quit smoking entirely.
Furthermore, 58.1% (n=36) of smoking participants at T1 reported being (rather) willing to refrain from smoking in the presence of non-smokers. At T2, this willingness had decreased to 45.1%. The proportion of respondents who smoked on the balcony or in the garden increased slightly at T2, while the proportion of those who smoked inside the home remained unchanged. These differences were not statistically significant (all p’s>.05).
3.6. Tobacco-Related Knowledge and Awareness
At both time points (T1 and T2), the vast majority of respondents correctly identified that secondhand smoke slows lung development in children and that smoking is a leading cause of lung cancer. Similarly, most participants correctly acknowledged that passive smoking significantly increases the risk of heart attacks, although this item had a relatively high proportion of “don’t know” responses.
The misconceptions that “light” cigarettes are less harmful and that tobacco becomes dangerous only above a certain number of cigarettes per day were correctly rejected by most respondents. Also, respondents answered in the majority of cases correctly that smoking is the most frequent reason for lung cancer and can negatively influence the development of the lungs in kids, and even secondhand smoke increases the risk of a heart attack. The statement that adolescents are less likely to start smoking if no one smokes at home, even though it has been mostly confirmed, received mixed responses, with 21% of respondents at T1 indicating they were unsure. On average, respondents answered 4.9 (of 6) items correctly at T1 and 5.1 at T2. These differences were not statistically significant (all p’s>.05).
4. Discussion
This study assessed a community-based smoking cessation intervention tailored to disadvantaged populations with a migration background in Switzerland. Overall, the findings indicate that the intervention successfully reached its intended target groups, with 95% of participants being first-generation migrants and a high proportion of individuals facing socioeconomic disadvantages - two indicators commonly associated with limited access to mainstream prevention services.2,3,5,20 In addition, based on the number of cigarettes smoked per day and patterns of nicotine dependence, a significant number of participants can be classified as high-risk smokers. Over half reported daily smoking within their family or close social environment, a context known to reinforce tobacco-related social norms and complicate cessation efforts. 16 The program achieved meaningful behavioral outcomes: by follow-up, 23% of smokers reported having quit smoking, and among those who continued smoking, daily cigarette consumption decreased significantly. In addition, half of current smokers reported at least one quit attempt, and non-smokers were activated as supportive agents within their social networks. Taken together, these results suggest that brief, linguistically and socially tailored interventions embedded in community settings can prompt both individual behavior change and broader normative shifts within disadvantaged populations, that are typically underrepresented in conventional smoking cessation programs. However, it should be noted that autochthonous disadvantaged population groups could not be reached despite considerable recruiting efforts.
As only individuals with a migration background participated in the interventions, it is questionable to what extent the results can be transferred to the autochthonous population, and it also raises the question of why this target group could not be reached despite intensive efforts. This may be explained by differences in group composition and, more specifically, by the stronger focus of autochthonous groups on certain topics (e.g., sport, leisure activities, interest-based gatherings) and other activities and contacts outside the group, and by their comparatively less holistic perception of the group as a central unit and hub for social interaction, in contrast to the migration and diaspora populations.
Interestingly, the relatively high proportion of participants reporting tertiary education should be interpreted with caution. In migrant populations, self-reported educational attainment is known to be influenced by differences in national education systems and classification schemes.39,40 In many countries of origin, vocational training or post-secondary non-academic education may represent the highest attainable level of education and may therefore be perceived and reported as ‘tertiary’, even though it does not correspond to tertiary education as defined in the Swiss or ISCED classification. As a result, self-reported education levels may overestimate formal tertiary attainment and do not necessarily contradict indicators of socioeconomic disadvantage.
The implementation indicators further support the successful reach of the target population. Out of 82 participating groups, all but one received the full two-part intervention, and group sizes ranged from 15 to 20 participants, as planned. Importantly, more than half of all participants were current smokers, confirming that the intervention not only addressed individuals who smoke but also reached mixed groups that included both smokers and non-smokers. This aligns with the program’s goal of creating a supportive social environment for behavior change and activating smoke-free norms within participants’ broader networks. Notably, one quarter of non-smoking participants reported encouraging smokers in their social circles to reduce or quit smoking. This finding underscores the potential of community-based interventions to mobilize strong social ties and catalyze behavioral change through normative influence - a mechanism well established in the literature on peer-based and family-centered public health strategies.16,23,41-43
Importantly, the program also achieved its key behavioral outcomes. Among smokers, 23% reported having quit smoking by follow-up. Among those who continued to smoke, the number of cigarettes consumed per day decreased significantly on average, which represents a promising outcome from a harm reduction perspective. Furthermore, 50% of current smokers at T2 reported at least one quit attempt. These behavioral indicators suggest that even brief, community-embedded interventions can prompt meaningful changes in smoking behavior.
Taken together, these results underscore that short, targeted interventions - when designed in a community-based and socially sensitive manner - can reach and activate disadvantaged populations while achieving both individual and interpersonal-level impacts.
4.1. Limitations
This study has several limitations that must be considered when interpreting the results. First, the reliance on self-reported data introduces potential biases, including recall inaccuracies and social desirability effects. Although data collection was conducted orally and in native languages by trusted intermediaries, these methods cannot entirely eliminate response biases and raise the risk of information bias, as smoking status was not biochemically validated and misclassification cannot be excluded.
Second, no formal sample size or power calculation was conducted. The study followed a pragmatic, feasibility-based sampling strategy informed by earlier projects (Tiryaki Kukla and Jeto pa Tym), which together implemented 151 group-based information sessions among Turkish- and Albanian-speaking communities. 30 While such feasibility-driven approaches are common in real-world community interventions, they limit the statistical precision of effect size estimates and do not allow for the determination of expected effects a priori. Future studies using randomized or controlled designs could incorporate formal power analyses to strengthen causal inference.
The study further relied on a purposive, community-based sampling strategy using pre-existing groups recruited through community networks and multipliers. As such, the sample cannot be considered representative of all disadvantaged migrant populations in Switzerland. Although recruitment across multiple languages, settings, and networks was used to increase heterogeneity within the target population, selection bias cannot be fully excluded. In addition, recruitment depended partly on personal and contextual factors related to the recruiters and multipliers, which may have influenced the number of groups reached within individual language groups.
While 82 workshops were delivered, only 42 groups were included in the analysis. Although this partial inclusion may have introduced some bias, the broad linguistic and contextual diversity across the included groups suggests that the findings are still reliable. Not all language groups were equally represented, which limits the generalizability of results across all migrant populations in Switzerland. Moreover, follow-up response rates differed between language groups, and overall attrition between T1 and T2 was approximately 50%. However, these response patterns are not unusual in community-based studies targeting underserved populations and align with response rates observed in comparable research.30,33,44
Another important limitation is related to the proportion of participants who initially expressed interest in the study: only about half could ultimately be reached for the baseline survey. Nevertheless, this level of engagement is consistent with previous studies that have used similar outreach methods in structurally disadvantaged settings.30,33
Although the project team symbolically compensated clubs/groups and key facilitators for their support in organizing the workshops and participants for their participation in the assessment and follow-up, this may have influenced participation rates. However, such incentives were modest and designed to support coordinative feasibility rather than motivate individual responses, making it unlikely that this significantly biased the outcomes regarding smoking itself.
Furthermore, the number of individuals who quit smoking may theoretically be over- or underestimated. Some participants who dropped out of the study might have quit without being captured in the follow-up data, while others may have relapsed. Also, given the outreach-based, community-embedded design, the use of telephone follow-up, and the involvement of socioeconomically disadvantaged and highly mobile populations, biochemical verification was not feasible without substantially increasing participant burden and attrition. The reliance on self-reported data is therefore consistent with comparable community-based smoking cessation studies, but may have resulted in an overestimation of quit rates.
Importantly, the intervention did not explicitly require a commitment to quit smoking. Rather, it focused on building awareness, motivation, and self-efficacy, allowing participants to decide for themselves whether and when to initiate cessation. This approach, including the framing around “critical life transitions” as potential windows for change, suggests that the three-month follow-up may have been too short to fully capture delayed behavioral effects. On the other hand, longer follow-up intervals would likely have led to even higher attrition, especially in a population already known for low research participation rates.
Finally, the study did not include a control group, which limits causal inference. Observed changes between baseline and follow-up cannot be attributed exclusively to the intervention but may partly reflect external influences or secular trends. Therefore, the results should be interpreted as indicative rather than causal.
4.2. Conclusions
This study suggests that setting- as well as linguistically tailored, low-threshold smoking cessation interventions may represent a promising approach to reach and engage disadvantaged populations with a migration background - groups typically underserved by conventional tobacco control efforts. By embedding the intervention in established community settings and addressing both smokers and non-smokers, the program appeared promoted individual behavior change while fostering supportive social environments.
The observed quit and quit-attempt rates between T1 and T2, along with reductions in cigarette consumption and the activation of non-smokers as change agents, indicate potential of such interventions for shifting smoking-related norms. However, these findings should be interpreted with caution, given the absence of a control group, the reliance on self-reported data, and the fact that primary outcomes applied only to the subgroup of regular smokers. The three-month follow-up period provides only a short-term perspective, and longer follow-up is required to assess the sustainability of these effects.
While methodological limitations such as self-reporting and partial group inclusion must be acknowledged, the findings suggest that even brief interventions can be impactful when they are built on language accessibility and existing social ties. Future programs should consider extending follow-up periods to capture longer-term effects and further investigate how social networks can sustain momentum for cessation over time.
Taken together, the results point to the potential value of community-based, inclusive prevention strategies in reducing tobacco-related health inequalities. From a policy perspective, the findings suggest that existing population-wide tobacco control strategies could be strengthened by systematically integrating linguistically and setting-based tailored outreach interventions targeting disadvantaged migrant populations. While Swiss tobacco control policies provide a general framework, they may insufficiently address structural and language-related barriers faced by specific subgroups. Sustained public funding and institutional anchoring of low-threshold, community-based programs could help close this gap and support further reductions in smoking prevalence among underserved populations. Further research is needed to confirm their long-term impact and generalizability of such approaches, which may also inform scalable models for other public health challenges involving underserved groups.
Footnotes
Acknowledgments
We would like to thank those responsible at the Tobacco Prevention Fund, Verena Friedrich and Brigitte Moser, for the trust they have placed in us and for their support in conducting the study. Special thanks go to the stop-smoking coaches who supported us in conducting and coordinating the surveys and thus made a significant contribution to the success of the evaluation. We would also like to thank all the key persons and association members who took part in the focus groups, interviews and the pre-/post-survey and made their experience and knowledge available to us.
ORCID iDs
Ethical Considerations
The study was submitted to the Cantonal Ethics Committee Zurich (BASEC Req-2025-00635). The committee confirmed that the project did not fall under the scope of the Swiss Human Research Act (HRA) and therefore did not require ethical approval. Also, no prospective study protocol was registered as the project was designed as a pragmatic, non-clinical intervention.
Consent to Participate
All participants provided verbal informed consent prior to data collection.
Consent for Publication
Not applicable. The manuscript does not contain any individual person’s data in any form (including images, videos, or identifying details).
Author Contributions
AZ: Conceptualization, Methodology (evaluation component), Investigation, Supervision, Formal Analysis, Data Curation, Resources (training of research staff), Writing – Original Draft, Writing – Review & Editing, Funding Acquisition (evaluation component).
LBO: Methodology (evaluation component), Investigation, Supervision, Formal Analysis, Data Curation, Resources (training of research staff), Writing – Original Draft, Writing – Review & Editing.
PL: Conceptualization, Methodology (evaluation component), Investigation, Supervision, Formal Analysis, Data Curation, Resources (training of research staff), Writing – Original Draft, Writing – Review & Editing.
SS: Conceptualization, Methodology (evaluation component), Investigation, Supervision, Formal Analysis, Data Curation, Resources (training of research staff), Writing – Original Draft, Writing – Review & Editing, Funding Acquisition (evaluation component).
SA: Project Administration (workshops), Investigation (practical implementation), Resources (training of coaches and physicians), Writing – Review & Editing.
RPC: Conceptualization (intervention), Methodology (intervention component), Supervision (workshops), Investigation, Resources (training of coaches and physicians), Writing – Review & Editing, Funding Acquisition (intervention component).
OS: Project Administration (workshops), Investigation (practical implementation), Resources (training of coaches and physicians), Writing – Review & Editing.
CSG: Conceptualization (intervention), Methodology (intervention component), Supervision (workshops and overall project), Formal Analysis, Writing – Review & Editing, Project Administration, Funding Acquisition (intervention component).
NK: Project Administration, Resources, Supervision (workshops and staff coordination), Investigation, Formal Analysis, Interpretation, Writing – Original Draft, Writing – Review & Editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swiss Tobacco Prevention Fund (TPF) under contract numbers 326.5-/36 (for workshop implementation) and 326.5-2/43 (for the study part). The opinions expressed and arguments employed herein do not necessarily reflect the official views of the Swiss Government. The funders had no role in study design, data collection and analysis, the decision to publish, or the preparation of the manuscript.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Corina Salis Gross is a member of the Swiss Federal Commission on Addiction and Prevention of Non-Communicable Diseases (EKSN). The other authors have no conflicts of interest to declare.
Data Availability Statement
The datasets and the original questions are available upon reasonable request from the corresponding author.
Appendix
Summary of Questionnaire Domains and Assessment Instruments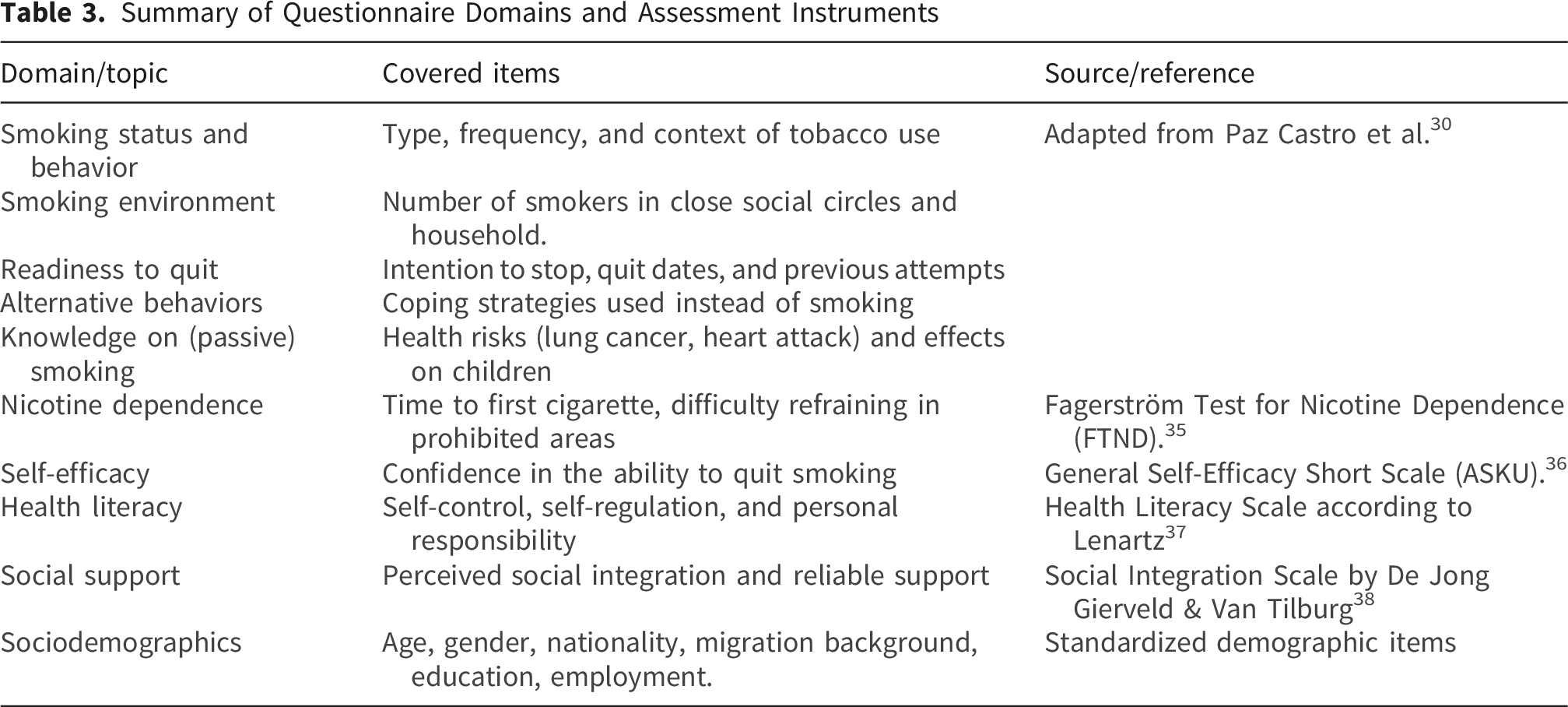
Domain/topic
Covered items
Source/reference
Smoking status and behavior
Type, frequency, and context of tobacco use
Adapted from Paz Castro et al.
30
Smoking environment
Number of smokers in close social circles and household.
Readiness to quit
Intention to stop, quit dates, and previous attempts
Alternative behaviors
Coping strategies used instead of smoking
Knowledge on (passive) smoking
Health risks (lung cancer, heart attack) and effects on children
Nicotine dependence
Time to first cigarette, difficulty refraining in prohibited areas
Fagerström Test for Nicotine Dependence (FTND).
35
Self-efficacy
Confidence in the ability to quit smoking
General Self-Efficacy Short Scale (ASKU).
36
Health literacy
Self-control, self-regulation, and personal responsibility
Health Literacy Scale according to Lenartz
37
Social support
Perceived social integration and reliable support
Social Integration Scale by De Jong Gierveld & Van Tilburg
38
Sociodemographics
Age, gender, nationality, migration background, education, employment.
Standardized demographic items