
Abstract
Introduction
Tobacco use causes 7.7 million deaths globally. 1 Tobacco use prevalence is projected to be 12% in low-income countries and more than 20% in middle-income countries over the next decade. 2 According to the India National Family Health Survey (NFHS-5) conducted in India, between 2019 and 2021, the overall prevalence of tobacco use among adults is approximately 28.6%. 3 A wide range of tobacco products are available including bidis (“home-made cigarettes” consisting of flaked tobacco hand-wrapped in a dried temburni [Dio-spyros melonoxylon] leaf), cigarettes, hookah, and mishri (roasted and powdered tobacco used as a dentifrice), facilitating use of multiple products.4,5 Among individuals who use tobacco in India, 12% report multiple tobacco product (MTP) use. 6 MTP use is associated with increased risk for adverse health outcomes and warrants in-depth study. 4
People infected with the Human Immunodeficiency Virus (PWH) are an important population at risk for tobacco-related harms. About 2.1 million individuals are infected with HIV in India. 7 It is well-documented that PWH have higher rates of tobacco use. 8 In India, the prevalence of tobacco use is estimated at 68% in HIV-positive males and 12% in HIV-positive females, compared to 58% in HIV-negative males and 11% in HIV-negative females. 9 Tobacco use in PWH increases the risk for several complications including tuberculosis, 8 cancer, and cardiovascular events.10,11 Data from the US shows that the prevalence of MTP use (22%) is lower in PWH 12 compared to the general population (32%). 13 However, PWH who use MTP are less likely to successfully quit. 14 Research on factors associated with MTP use in LMICs has primarily focused on the general population. 15 It is essential to identify factors associated with MTP use in vulnerable populations, such as PWH, to effectively monitor trends and to guide tobacco policy and cessation services. 15 This study aims to identify the patterns and correlates of MTP use among PWH who currently use tobacco in a Chennai, India clinic.
Methods
Study design and setting
This descriptive study uses baseline data from a pilot study that assessed tobacco use patterns in PWH who were initiating HIV care in a single clinic in Chennai. Participants were recruited during routine HIV care visits. Inclusion criteria: individuals aged 18 years or older who presented for HIV care at the Voluntary Health Services Infectious Disease Medical Center (VHS-IDMC) between October 2019 and December 2021. Due to COVID-19 pandemic, recruitment was paused from March 2020 to April 2021. Exclusion criteria: patients were excluded if they were unable to understand English, Tamil, or Telugu, or unwilling to participate in a 3-month follow-up assessment for the pilot study. Of 154 patients enrolled in the pilot, the current analysis focused on those who reported current tobacco use (58 of 154). The study was approved by ethics review boards at Massachusetts General Hospital (2018P000799), Boston, USA and VHS-IDMC (VHS/IEC/95b/2020) in India. All participants provided written informed consent.
Study measures
The survey measured demographics and cessation indicators including intentions to quit tobacco, confidence in quitting, and the belief in the importance of quitting. Tobacco use status questions were derived from the Global Adult Tobacco Survey. 16 The questionnaire (included as Supplemental material) was pre-tested by study staff. We provided participants with a list of tobacco products to indicate products used on a daily or weekly basis, and classified individuals as either using; (1) a single product, (2) multiple products, or (3) unknown (those who did not specify the number of products they used) (Supplemental Figure 1). Among individuals who reported MTP use, we cataloged reported products to identify which were frequently combined.
Urine cotinine was used to assess nicotine exposure. 17 Urine samples were collected at the time of the in-person survey. The Fagerström Test for Nicotine Dependence (FTND) scale (sensitivity 0.75, specificity 0.80 18 ) was used to assess nicotine dependence on smoked tobacco. 19 The Fagerström Test for Nicotine Dependence-Smokeless Tobacco (FTND-ST, correlation with serum cotinine 0.53 [P < 0.001], internal consistency coefficient alpha 0.47) was used to assess nicotine dependence on smokeless products. 20 Items on both scales are summed to a total score ranging from zero to 10. For individuals using smoked and smokeless products, we compared total scores on both scales and used the higher of the two in the analysis.
Participants were asked whether they had tried to quit smoking in the past year, and to indicate their intentions to quit tobacco within the next six months. Questions were based on the Transtheoretical Model's stages of change and have been used in prior studies.21,22 Participants also indicated their level of confidence in quitting and belief in the importance of quitting on 10-point scales (low numbers indicated less importance or confidence) used in a prior study conducted in LMICs. 14
Analysis
We conducted a descriptive analysis and compared group differences between (1) single product use vs MTP use, and (2) single product use vs unknown use. We provide medians and interquartile ranges (IQR) for continuous variables, and percentages and 95% confidence intervals (95% CI) for categorical variables. Group differences were tested using Fisher’s exact test for categorical variables, 23 and the Wilcoxon rank-sum test for continuous variables. 24 The statistical significance level was set at a two-sided significance level of 0.05. Data were analyzed using STATA V15.1.
Results
This study was conducted among adult PWH at a single clinic in Chennai (n = 154, 67.5% male, 57.8% Telugu/41.5% Tamil, mean age 19.8 (SD: 8.4)). Current tobacco use was reported by 37.7% (58/154) of adults with PWH at the clinic.
Characteristics of PWH Who Currently Use Tobacco and Are Initiating HIV Care in Chennai, India.
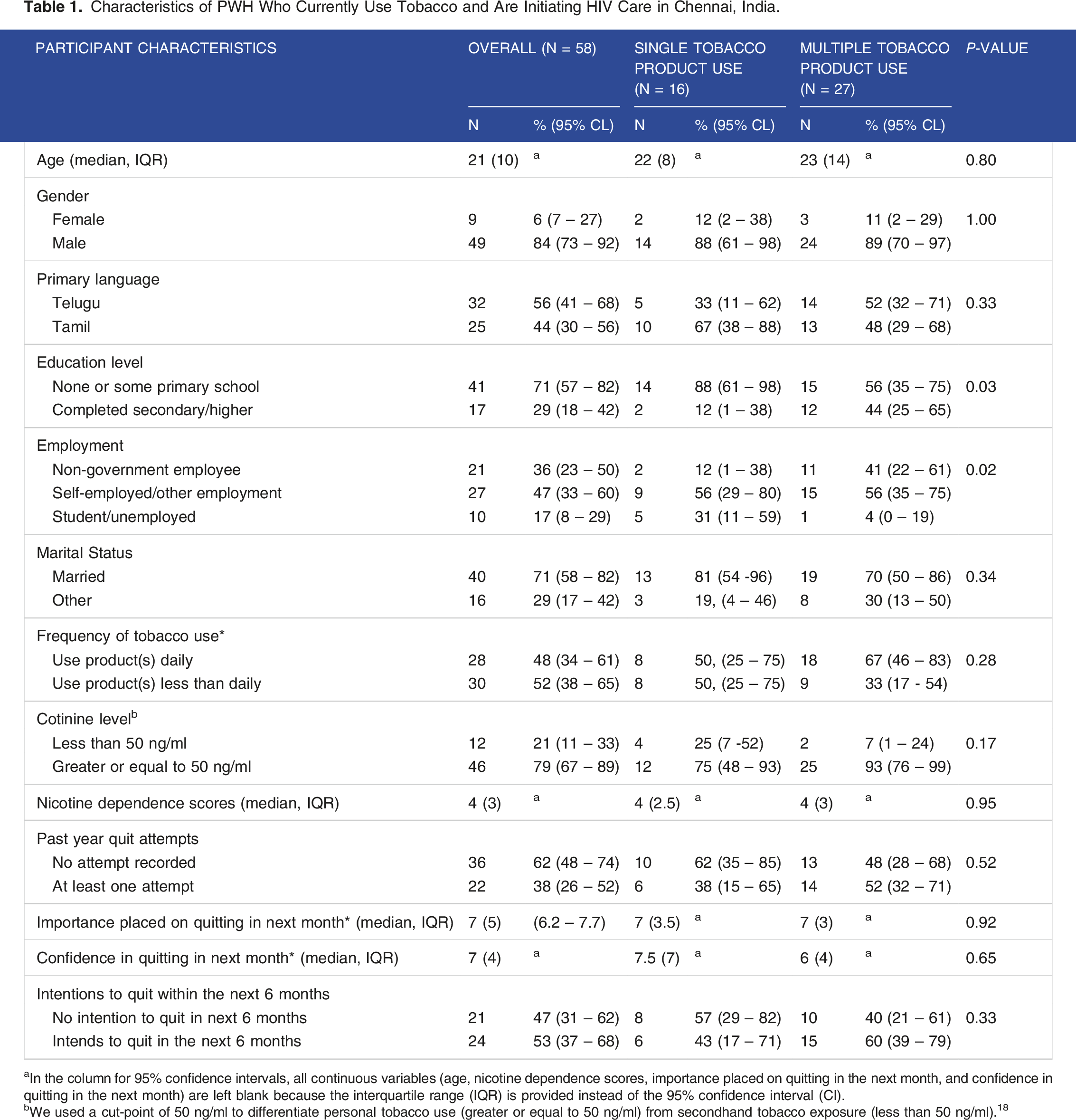
aIn the column for 95% confidence intervals, all continuous variables (age, nicotine dependence scores, importance placed on quitting in the next month, and confidence in quitting in the next month) are left blank because the interquartile range (IQR) is provided instead of the 95% confidence interval (CI).
bWe used a cut-point of 50 ng/ml to differentiate personal tobacco use (greater or equal to 50 ng/ml) from secondhand tobacco exposure (less than 50 ng/ml). 18
‘Less than daily’ tobacco use (n = 30/58, 52%; 95% CI: 38% - 65%) was more common than daily use. Forty-six percent of current tobacco users (n = 27/58; 95% CI: 33% - 60%) used multiple products, and 28% (n = 16/58; 95% CI: 17% - 41%) used a single product. The remainder of current tobacco users (n = 15/58, 25%; 95% CI: 15% - 39%) did not specify number of products used. Seventy nine percent (n = 46/58, 95% CI: 67% - 89%) had cotinine levels equal to or higher than 50 ng/mL. (Table 1)
Participants who reported MTP use most commonly combined regular and hand-rolled cigarettes (n = 9/27; 33%), with another tobacco product. Overall, participants combined two to five products (median n = 3; IQR: 3). (Supplemental Figure 2)
Among participants who reported MTP use, 44% had secondary school education or higher (n = 12/17; 95% CI: 25% - 65%); this proportion was lower in those who reported single product use (n = 2/16, 12%; 95% CI: 1% - 38%) (P-value = 0.03). A higher proportion of participants in the group were employed (non-government employees: n = 11/27, 41%; 95% CI: 22% - 61%, self-employed or other forms: n = 15/27, 56%; 95% CI: 35% - 75%) compared to the single product use group (non-government employees: n = 2/16, 12%; 95% CI: 1% - 38%, self-employed or other forms: 9/16%, 56%; 95% CI: 29% - 80%) (P-value = 0.04). We did not observe correlations between MTP use and cessation indicators including the frequency of tobacco use, cotinine levels, nicotine dependence scores, quit attempts, confidence, and importance of quitting (Table 1).
In the group of current tobacco users with unknown product use, a higher percentage was employed by non-government institutions (P-value = 0.04) and reported ‘less than daily’ tobacco use compared to the single product use group (P-value = 0.04) (Supplemental Table 1)
Discussion
Among PWH who currently use tobacco in a Chennai clinic, nearly half reported MTP use. Individuals combined an average of three tobacco products. PWH who reported MTP use were more likely to have a higher education level and to be employed compared to those who reported single product use. Among individuals with an unspecified number of tobacco products, most were employed, and daily tobacco use was uncommon. The frequency of tobacco use, cotinine levels, nicotine dependence scores, number of quit attempts, confidence, and importance of quitting were similar between individuals who reported MTP use and those who reported single product use.
The observed prevalence of MTP use among PWH who currently use tobacco is significantly higher at 46% compared to 12% in the general population in India. 25 In the state of Tamil Nadu (where Chennai is located), MTP use in the general population decreased from 1.5% in 2009-10 to 1.0% in 2016-17. 14 Given these broader trends in tobacco consumption in the region, this work highlights a concerning disparity impacting PWH.
The results show that individuals who report MTP use were more educated, and a greater proportion were employed compared to those who used a single product. Our findings contradict findings from studies conducted among PWH in high-income settings, which suggest that MTP use is associated with lower education attainment and unemployment,12,14,26 and findings from the general population in LMICs that indicate that low socioeconomic status is associated with MTP use. 27 Explorations of MTP use among PWH in LMICs are limited in the literature, and meaningful comparisons across regions and countries cannot be readily ascertained.
In this study, regular and hand-rolled cigarettes were the predominant tobacco products, often combined with at least one other product. Identifying the patterns of use in PWH can inform the design of tailored cessation interventions. Researchers in India have identified five latent classes of tobacco use patterns with notable differences across groups. 25 Their work shows that among individuals who report MTP, those who predominantly use cigarettes tend to smoke earlier upon waking. 25 These findings can be used to tailor cessation programs that account for the observed patterns of tobacco use.
Tobacco control efforts in India have positively impacted the prevalence of tobacco use, with the number of tobacco users reducing by 8.1 million in 2017 compared to 2009. 28 Between 2010-20, tobacco use in Tamil Nadu was estimated at 4.9% among women and 20.0% among men. 3 However, the diversity of tobacco products available in India and associated MTP use emphasize the need for education programs that address the heightened challenges associated with MTP use.
Tobacco control policies should not consider products in isolation. Policies addressing tobacco use should consider patterns of use, recognizing that people often use multiple products, and may substitute or combine products for greater nicotine consumption. Accounting for MTP use patterns, when designing public health campaigns, offers opportunities for harm reduction and has the potential to reduce dependence on tobacco.
Limitations
Recruitment of study participants was impacted by the COVID-19 pandemic. This may have introduced selection bias if patients’ patterns of initiating HIV care differed before and after the COVID-19 pandemic started. The small sample size limited our statistical power to detect associations between MTP use and cessation-related outcomes. Due to the multiple testing conducted in the study, the P-values should be interpreted with caution.
Conclusion
Among PWH who currently use tobacco in a Chennai clinic, almost half combine multiple products. MTP use in PWH was linked to higher education levels and employment in this single clinical setting.
Supplemental Material
Supplemental Material - Patterns and Correlates of Multiple tobacco Product use Among people With HIV in India
Supplemental Material for Patterns and Correlates of Multiple tobacco Product use Among people With HIV in India by Catherine S. Nagawa, Poongulali Selvamuthu, Nagalingeswaran Kumarasamy, Faith Beulah Balakrishnan, Nancy A. Rigotti, and Gina R. Kruse in Tobacco Use Insights.
Supplemental Material
Supplemental Material - Patterns and Correlates of Multiple tobacco Product use Among people With HIV in India
Supplemental Material for Patterns and Correlates of Multiple tobacco Product use Among people With HIV in India by Catherine S. Nagawa, Poongulali Selvamuthu, Nagalingeswaran Kumarasamy, Faith Beulah Balakrishnan, Nancy A. Rigotti, and Gina R. Kruse in Tobacco Use Insights.
Footnotes
Acknowledgement
We would like to acknowledge the participants and study team members for their valuable contribution to this study.
Author Contributions
Conceptualization: GK, CN, PS; Formal analysis: CN; Writing-original draft preparation: CN, GK; Writing-review and editing: PS, NK, FB, NR, GK; Funding acquisition: PS, NR, GK; Supervision: GK, NR.
Declaration of Conflicting Interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GK has a family financial interest in Dimagi, INC. GK has received research from the National Comprehensive Cancer Network with funding from Astra Zeneca and the National Cancer Institute. NR has consulted for and received a research grant from Achieve Life Sciences for an investigational smoking cessation medication. She receives royalties from UpToDate for writing reviews on smoking cessation. For the remaining authors no conflicts of interest were declared.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study reported here was supported by NIH/NIAID 5P30AI060354-14 grant “Harvard University Center for AIDS Research” Developmental Award and NIH U01CA261614. NC received support from NCI T32CA05771.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.