
Abstract
Introduction
Among dual-smoking couples, both partners have smoking-related motivations that may either facilitate or hinder cessation efforts. Existing research typically focuses on individual-level motivation, which may be inadequate for capturing aspects of concordance and discrepancy. This study characterized couples’ motivational profiles and examined their associations with smoking cessation outcomes.
Methods
We conducted secondary analyses from a randomized controlled pilot study of 95 dual-smoking couples to examine how dyadic motivations to quit smoking predicted individual and joint point-prevalence abstinence at 3 months. Both partners reported their own motivation to quit (self-oriented) and their motivation for their partner to quit (partner-oriented). We examined dyadic motivation to quit smoking on abstinence across four goal characterizations: (1) Parallel Goals (partners’ self-oriented motivations), (2) System-Oriented Goals (an individual’s self- and partner-oriented motivation), (3) Shared Target Goals (both partners’ motivation for one individual to quit), and (4) Parallel Partner-Oriented Goals (each partner’s motivation for the other to quit). Using response surface analyses with logistic regression, we estimated the effects of alignment (a1) and misalignment (a2) in the couples'’ motivation levels on individual and joint cessation outcomes.
Results
For individual cessation, quitting odds were higher when self-motivation or partner-oriented motivation aligned within the couple (Parallel goals: a1 = 0.725; Shared Target goals: a1 = 0.881; Parallel Partner-Oriented goals: a1 = 0.729), when self-motivation exceeded partner’s self-motivation (Parallel goals: a3 = 0.453), or exceeded partner-oriented motivation (System-Oriented goals: a3 = 1.094). Joint quitting was more likely when both partners had high self-motivation (Parallel goals: a1 = 0.918), high self- and partner-oriented motivation (System-Oriented goals: a1 = 0.310), high shared motivation for one partner to quit (Shared Target goals: a1 = 0.673), or high partner-oriented motivation for each other (Parallel Partner-Oriented goals: a1 = 0.965). All effects were statistically significant (P < .05).
Conclusion
The findings highlight the role of dyadic motivations in predicting individual and dyadic abstinence among dual-smoking couples. Couple-based interventions that aim to increase and align partners’ motivations to quit could improve cessation outcomes in this population.
Keywords
Introduction
Individuals with high levels of motivation to quit smoking are more likely to persist in quitting efforts and achieve abstinence, 1 even after accounting for other influential factors, such as prior quit attempts. 2 The level of motivation to quit is closely linked to cessation self-efficacy (ie, confidence in one’s ability to quit),3,4 which shapes both the intensity and duration of quit efforts in challenging circumstances. 5 Cessation interventions can be calibrated to an individual’s level of motivation to quit. That is, highly motivated individuals can benefit from pharmacotherapies (eg, nicotine replacement therapy, varenicline, bupropion)6,7 and behavioral counseling, 8 whereas individuals with lower motivation may respond better to low-intensity strategies aimed at fostering motivation (eg, reflecting on smoking behavior or setting short-term abstinence goals).9-11 Longer low-intensity interventions (such as receiving motivational messages for 6 months or more) could produce more sustained effects on motivation. 12
In dual-smoking couples (ie, romantic partners who both smoke), considering both partners’ motivations to quit may be more informative than considering individual-level motivation. In many dual-smoking relationships, individuals’ motivation to quit are not correlated, 13 suggesting that even though individuals may experience high motivation to quit, there will often be mismatches or misalignment between motivation levels within the couple. Even when couples are aligned in their motivation levels, that alignment can occur at either a high level (both are very motivated) or at low level (both are not very motivated). Aligning at high levels is likely to support smoking cessation, whereas alignment at a low level may interfere with it. Understanding ways to promote smoking cessation within couples remains of public health relevance, as estimates suggest that roughly one-third of married couples are dual-smoking couples.14-16
Approaches to analyzing the impact of motivation on cessation within couples, rather than individuals, can be informed by the theory of transactive goal dynamics (TGD). 17 The TGD conceptualizes interpersonal relationships as systems in which partners’ goals are interdependent and partners mutually influential each other’s goal outcomes. 17 TGD offers a unique advantage over other theories, such as Social Interdependence Theory, 18 in that it conceptualizes close relationships (eg, couples) as dynamic systems of interdependent goals in which each partner’s motivations and behaviors directly influence the other’s outcomes. From this perspective, the motivation of both members of a couple shape smoking behaviors and cessation outcomes. When both partners have high levels of motivation to quit, they may be more likely to collaborate, provide mutual support, and reinforce each other’s cessation behaviors, thereby increasing the likelihood of successful quitting. By contrast, when motivation levels are low or misaligned, conflict or lack of support can emerge, 19 potentially undermining cessation efforts and/or heightening the risk of relapse. Examining alignment in partners’ motivations to quit and its impact on individual and joint cessation outcomes is especially important in dual-smoking relationships, where quit attempts are less common and relapse is more likely than in single‐smoking relationships. 20
TGD posits that individuals in relationships pursue goals interdependently. This means that each partner experiences motivation for their own cessation outcomes as well as motivations for their partner’s outcomes (partner-oriented motivations). 17 For example, Alicia may be highly motivated to quit smoking herself (self-oriented motivation to quit), and also highly motivated for her partner, Bokai, to quit (partner-oriented motivation to quit). Alternatively, Alicia may have low motivation in both areas or feel strongly about one, but not the other, resulting in either alignment (at high or low levels) or misalignment between her self- and partner-oriented motivations. The same dynamic applies to Bokai. Each partner may experience alignment or misalignment within themselves, and alignment or misalignment as a couple (eg, both wanting to quit vs only one partner wanting to quit).
The Present Research
In this study, we examined how baseline alignment and misalignment (ie, discrepancy) in motivations to quit smoking influenced both individual and couple-level cessation outcomes among dual-smoking couples. Motivational alignment reflects the degree to which two motivational ratings (eg, self- and partner-oriented motivations) are similar in value. Misalignment reflects the extent and direction of the difference between two motivational ratings (eg, one form of motivation being higher than another). We evaluated how these two constructs impact cessation outcomes across four goal structures shown in Figure 1 that characterize the couple’s motivations to quit. Configuration of Motivations to Quit in Dual-Smoking Couples
We applied Response Surface Analysis (RSA), 21 which is well-suited to assess both linear and curvilinear effects of alignment and discrepancy on behavioral outcomes. We hypothesized that the degree of motivational alignment, and the direction of any discrepancy, would each influence cessation success. Specifically, we hypothesized that:
Alignment Hypothesis
The odds of quitting smoking will increase as both motivation levels (ie, self-motivations to quit, partner-motivations to quit) increase.
Misalignment Hypothesis
The odds of quitting will be higher as discrepancies in motivation levels decrease. In situations where the motivation input differs (eg, Alicia has low motivation to quit herself but high motivation for Bokai to quit), we expect that an individual’s likelihood of quitting is higher if self-oriented motivation exceeds their partner’s motivation (ie, self > partner) compared to when the partner’s motivation is greater.
Methods
The current study utilized secondary data from a randomized controlled pilot study. 22 The pilot study examined the feasibility, tolerability, and initial smoking cessation outcomes of partner-involved financial incentives (PIFs) in dual-smoking couples. Dual-smoking couples (n = 95 couples [180 individuals]) were recruited between February 2021 and May 2022 using Facebook/Instagram ads, Craigslist postings, and the Research-Match database in the United States. Eligibility criteria included: (1) smoking at least 5 cigarettes daily, (2) being 18 years or older, and (3) romantically partnered and cohabiting with another individual who smoked. Individuals with a high risk of psychosis, recent hospitalization, or pregnancy were excluded. Couples were randomized to one of three conditions: (1) control group with no financial incentives, (2) single-target condition in which one partner received incentives, and (3) dyadic-target condition in which both partners received incentives. Power analyses based on prior research indicated that an intent-to-treat sample of approximately 95 participants would provide ∼82% power to compare the control and PIF conditions. However, because the present study is a secondary analysis, these power calculations were not based on the specific research questions addressed here. All participants received four weekly online psychoeducation modules that combined behavioral change coaching with information about addiction and quitting and were offered home delivery of NRT (patch and/or gum) calibrated to their smoking level. This treatment was provided for 8 weeks following baseline. The main study findings showed that dyadic implementation of PITs is feasible, tolerable, and associated with smoking cessation in dual-smoking couples. 23 The study was approved by the Institutional Review Board at the University of Georgia (IRB #7344). Written informed consent was obtained from all individual participants included in the study.
Using TGD, we identified four distinct and potentially important characterizations that combine self- and partner-oriented motivations. The four characterizations of the motivation levels are as follows (also shown in Figure 1). One, parallel goals characterize alignment (or misalignment) between the couple’s self-oriented motivations to quit. Two, shared target goals characterize the couple’s desire for a particular individual in the relationship to quit (eg, Alicia’s self-oriented motivation to quit and Bokai’s motivation for Alicia to quit), describing the degree of alignment or misalignment in the motivation for a single individual to quit in the couple system. Three, system-oriented goals characterize the alignment within one person’s motivations for both members of the couple to quit smoking. For example, system-oriented goals capture how much Alicia is motivated to quit and how much she would like Bokai to quit smoking. In this way, system-oriented goals differ from the other goal characterizations by focusing on internal alignment (within an individual) between self- and partner-oriented motivations, rather than on interpersonal alignment of these motivations between partners. Four, parallel partner-oriented goals characterize the extent to which the couple is aligned in their desire for the other to quit (eg, Alicia is motivated for Bokai to quit, Bokai is motivated for Alicia to quit). Within each characterization, self- and partner-oriented motivations may align at high or low levels or may misalign.
Measures
Demographic and smoking characteristics: Data were collected on demographic and smoking-related characteristics. These included age, gender, race, education level, income, and relationship length in years, cigarettes per day as self-reported by participants, and e-cigarette use. We assessed nicotine dependence using the Fagerström Test for Nicotine Dependence (FTND).
24
The FTND is a widely used six-item scale that measures the severity of nicotine dependence, with scores ranging from 0 to 10
Motivations to quit (independent variable). Motivations to quit smoking were assessed at baseline using two sets of four self-report questions. First, participants completed the Motivation Rulers, which assess confidence, readiness, and importance of quitting on 11-point scales (eg, 0 = not at all ready, 10 = 100% ready). Participants also reported their motivation to stop smoking using the Motivation to Stop Smoking Scale (MTSS) on a scale from 1 (I don’t want to stop smoking) to 7 (I REALLY want to stop smoking and intend to in the next month).25,26 Scores on the MTSS were converted to an 11-point scale for analyses. These four items (three from the Motivation Rulers and the MTSS) captured one’s own motivation (α = .90) and were averaged for analyses.
Second, participants completed these same items from the Motivation Rulers and the MTSS oriented toward the partner (eg, how important is it to you that your partner quit smoking?) Scores on the partner-oriented MTSS were converted to an 11-point scale for analyses. These four items capturing motivation for the partner to quit demonstrated good reliability (α = .87) and were averaged for analyses. Partners’ scores were linked by a coupleID variable, allowing us to identify each configuration of motivation for each couple and participant.
Smoking cessation outcomes (dependent variable). Cessation outcomes were: (1) individual cessation, and (2) joint cessation. Cessation was assessed through point-prevalence abstinence at a 3-month follow-up, defined as self-reported abstinence for 7 or more consecutive days with biochemically confirmed using carbon monoxide levels ≤5 ppm via ICOquit breath sensors. 27 Individual cessation was defined as an individual reporting 7-day point prevalence at 3 months follow-up, and joint cessation was defined as both partners reporting 7-day point-prevalence abstinence at follow-up.
Analysis
We first provide descriptive statistics of the overall study sample. We then used response surface analysis (RSA) implemented using logistic regression. 28 The RSA approach offers a detailed understanding of how combinations of two predictor variables relate to an outcome variable. 28 RSA offers a key advantage over other approaches by modeling partners’ motivations simultaneously in relation to each other, rather than collapsing them into a single difference score. 29 The approach enables exploration of how each partner’s motivation level (high vs low) and the extent of their alignment or misalignment relate to outcomes, capturing nuances that a single difference score would obscure. Within this approach, we used logistic regression to quantify how couple motivation levels shape the log odds of individual and joint abstinence, with intervention (0 = No, 1 = Yes) added as a covariate. Separate models were estimated for individual and joint cessation outcomes using a complete case analysis.
RSA models were run for each of the four characterizations of the couple’s motivations to quit (Table 1). Models 1A and 1B estimate individual and joint outcomes under the parallel goals system, reflecting each partner’s self-oriented motivation to quit. In this model, we assumed that each partner’s self-oriented motivation impacts joint quitting outcomes equally; therefore, we set β1 = β2 and β3 = β5 in the model that assessed joint outcomes. A similar approach was followed for Model 4 estimated outcomes for the Parallel partner-oriented goal system, characterizing the extent to which each partner wants the other to quit. For the remaining two models, the estimates were assumed to have independent effects on both individual and joint cessation outcomes. Model 2A (individual cessation) and 2B (joint cessation) provide estimates of cessation outcomes under the System-Oriented Goals system, which characterizes the extent to which one person expresses motivation for both members of the couple to quit smoking. Model 3A and 4B provide estimates for the Shared Target Goals system, describing the couple’s motivation for a particular individual in the relationship to quit smoking. Model 4A and 4B provide estimates for the Parallel Partner-Oriented Goals system, describing the couple’s motivation for each other to quit smoking. Within each model, we plotted abstinence as a function of these motivations using the formula: For each couple (i = 1, …, n): Zᵢ: Cessation outcomes (separate models ran for individual and joint outcomes) Xᵢ: Differs based on model (see Table 1) Yᵢ Differs based on model (see Table 1) Wᵢ: Intervention received (yes/no) Operationalization of Xi and Yi in Each Model aIn these models, we assumed that β1 = β2 and β3 = β5.


Percentage of Participants With Aligned versus Discrepant Scores

Second, we performed polynomial regression to assess linear and non-linear relationships between the motivational alignments and (a) individual cessation and (b) joint cessation outcomes. We first ran a fully adjusted model that controlled for both partners’ age, gender, race, ethnicity, and household income. Because these covariates did not change the motivation-alignment coefficients (see Supplemental Table 1), we report results from a parsimonious model. To address multicollinearity, both predictors (motivations to quit) were centered around the scale midpoints. Third, we summarize the five response-surface parameters (a1–a5) derived from the polynomial regression (see Supplemental Table 2). Each parameter corresponds to a specific feature of the three-dimensional surface that relates partners’ self-- and partner-oriented motivations (X and Y) to cessation outcomes.
Fourth, we visualized these relationships using three-dimensional response surface graphs, which clearly illustrate how alignment or misalignment in motivation affects individual and joint cessation. We interpreted the surface values (a1, a2, a3, a4, and a5) to address three primary questions: (1) how alignment in motivation levels (a1: linear; a2: non-linear) across the four goal combinations affects individual and joint cessation outcomes; (2) how misalignment in motivation levels (a3: linear; a4: non-linear) across goal combinations influences cessation outcomes; and (3) whether the shapes (curvatures) of the outcome along the aligned (X = Y) and misaligned (X ≠ Y) diagonals differ significantly, and how this divergence impacts quit outcomes. All statistical tests were two-tailed, and a significance level of P < .05 was assumed.
Results
Characteristics of Participants Who Enrolled in a Pilot Trial Investigating the Feasibility and Preliminary Efficacy of Financial Incentives for Smoking Cessation in Dual-Smoking Couples

Effects of Parallel Goals: Combining Partners’ Self-Oriented Motivations to Quit
Individual Cessation
Regression Coefficients, and the Five Derived Congruence and Discrepancy Parameters the Response Surface Analysis Model
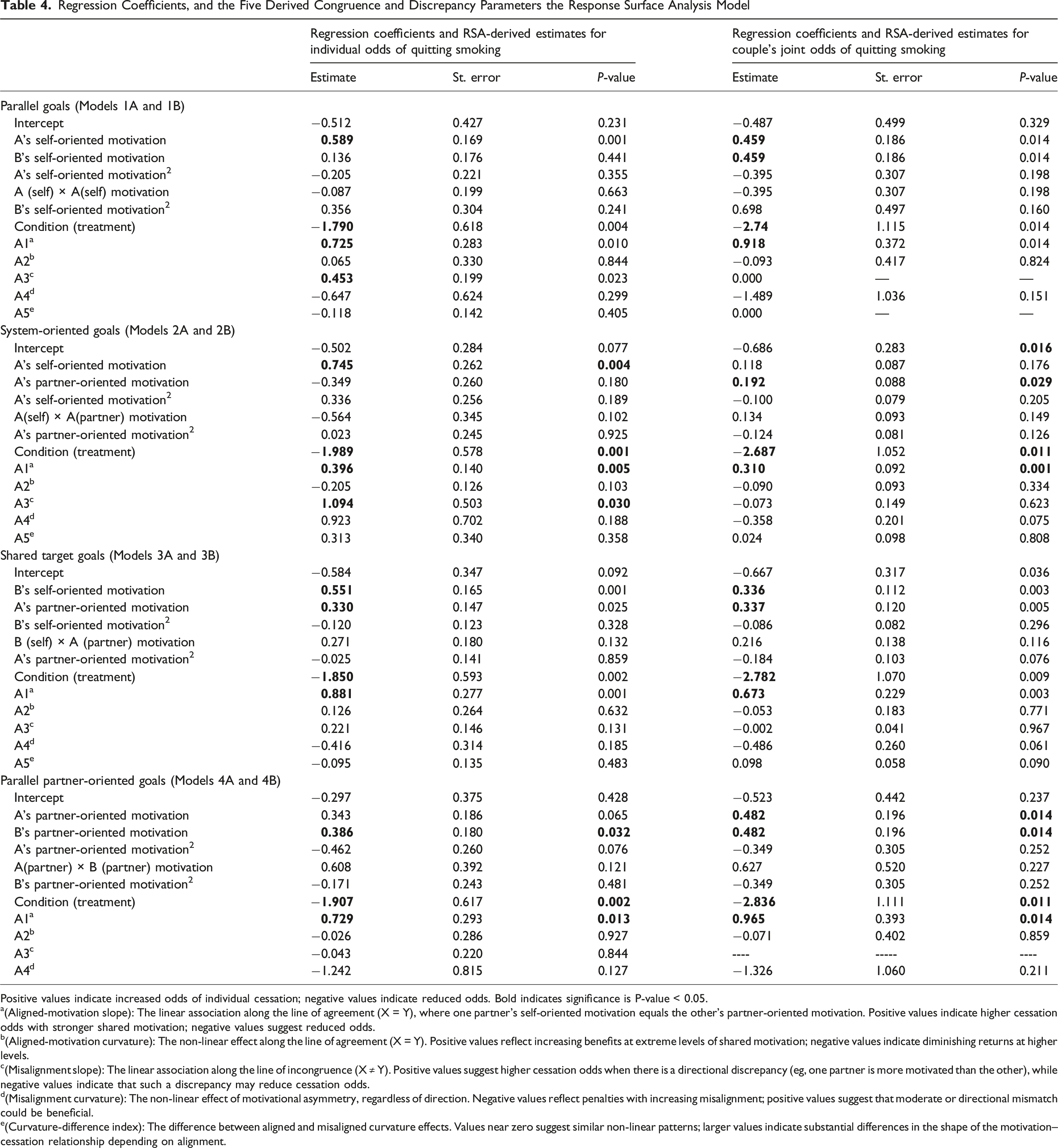
Positive values indicate increased odds of individual cessation; negative values indicate reduced odds. Bold indicates significance is P-value < 0.05.
a(Aligned-motivation slope): The linear association along the line of agreement (X = Y), where one partner’s self-oriented motivation equals the other’s partner-oriented motivation. Positive values indicate higher cessation odds with stronger shared motivation; negative values suggest reduced odds.
b(Aligned-motivation curvature): The non-linear effect along the line of agreement (X = Y). Positive values reflect increasing benefits at extreme levels of shared motivation; negative values indicate diminishing returns at higher levels.
c(Misalignment slope): The linear association along the line of incongruence (X ≠ Y). Positive values suggest higher cessation odds when there is a directional discrepancy (eg, one partner is more motivated than the other), while negative values indicate that such a discrepancy may reduce cessation odds.
d(Misalignment curvature): The non-linear effect of motivational asymmetry, regardless of direction. Negative values reflect penalties with increasing misalignment; positive values suggest that moderate or directional mismatch could be beneficial.
e(Curvature-difference index): The difference between aligned and misaligned curvature effects. Values near zero suggest similar non-linear patterns; larger values indicate substantial differences in the shape of the motivation–cessation relationship depending on alignment.

Illustration of How Alignment and Misalignment in Partner Motivations Influence Smoking Cessation Outcomes
Joint Cessation
The significant and positive linear congruence effect (a1 = 0.918, P = .014) indicated increasing odds of 7-day point prevalence joint cessation as self-oriented motivations to quit increase within the couple. We did not observe significant non-linear effects (a2 = −0.093, P = .824; a4 = −1.489, P = .151, a5 = 0.000). The two lines corresponding to a1 and a3 are shown in Figure B, illustrating the effects of aligned (a1) and misaligned (a3) motivation on joint cessation outcomes (Table 4, Figure 2B).
Effects of System-Oriented Goals: Combining Motivations for Self and Partner Within One Individual
Individual Cessation
We observed a significant positive linear congruence effect (a1 = 0.396, P = .005), indicating higher odds of individual abstinence as self-oriented and partner-oriented motivations levels both increased. Additionally, the significant positive linear discrepancy effect (a3 = 1.094, P = .030) indicated increasing odds of individual abstinence when self-oriented motivations to quit exceeded partner-oriented motivations to quit, highlighting a potential benefit of self-driven motivation even when partner-oriented motivation was lower (Table 4, Figure 2C).
Joint Cessation
The significant positive linear congruence effect (a1 = 0.310, P = .001) similarly indicated increasing odds of joint quitting as both self- and partner-oriented motivations increase. The linear discrepancy effect (a3 = −0.073, P = .623) and all non-linear terms (a2 = −0.090, P = .334; a4 = −0.358, P = .075; a5 = 0.024, P = .808) were not statistically significant (Table 4, Figure 2D).
Effects of Shared Target Goals: Combining Motivations Self-Oriented Motivation to Quit and Partner’s Motivation for Them to Quit
Individual Cessation
We observed a significant positive linear congruence effect (a1 = 0.881, P = .001), that showed higher odds of individuals abstinence as self-oriented motivation increased with their partner’s motivation for them to quit. No significant linear discrepancy (a3 = 0.221, P = .131) or non-linear effects (a4 = −0.416, P = .185; a5 = −0.095, P = .483) were observed (Table 4, Figure 2E).
Joint Cessation
The significant positive linear congruence effect (a1 = 0.673, P = .003), also indicated increasing odds of joint quitting as both self- and partner-oriented motivations increase. Linear discrepancy (a3 = −0.002, P = .967) and non-linear effects (a4 = −0.486, P = .061; a5 = 0.098, P = .090) were not statistically significant (Table 4, Figure 2F).
Parallel Goals: Effects of Combining Partners’ Motivations for Each Other to Quit on Cessation
Individual Cessation
The significant positive linear congruence effect (a1 = 0.729, P = .013), indicated higher odds of individual 7-day prevalence as both partner-oriented motivations increased. Linear discrepancy (a3 = −0.043, P = .844) and non-linear effects (a4 = −1.242, P = .127; a5 = −0.291, P = .118), were not statistically significant (Table 4, Figure 2G).
Joint Cessation
The linear congruence effect was positive and statistically significant (a1 = 0.965, P = .014), which indicated increasing odds of joint quitting success as both partner-oriented motivations to quit increased. Linear discrepancy (a2 = −0.071, P = .859) and non-linear terms a4 = −1.326, P = .211) were not significant (Table 4, Figure 2H).
Discussion
In this study, we examined how alignment and misalignment in the couple’s baseline motivations to quit smoking impacted individual and joint cessation outcomes at 3 months. We characterized and defined the couple’s motivations as: (1) parallel self-directed goals, (2) system-oriented goals (3) shared target goals, and (4) parallel partner-directed goals. Two hypotheses were proposed; (1) the alignment hypothesis
Our findings support the alignment hypothesis. Across all four goal characterizations of motivation levels, we found higher odds of quitting as self- and partner-oriented motivations to quit increased. This was true for both individual and joint cessation. The system-oriented models differed slightly from the rest of the characterizations in that the model focused on internal alignment or misalignment within one person, ie, motivations for them to quit and motivation for their partner to quit. Here, we also found that internal alignment between one’s desire to quit and their desire for their partner to quit resulted in positive cessation outcomes at follow-up. By contrast, the misalignment hypothesis was not consistently supported. There were situations in which having self-oriented motivation to quit that was greater than partner-oriented motivation was linked to modest improvements in individual cessation, but the effects were neither as strong nor as consistently replicated as those observed when motivations aligned. Our findings highlight that high mutual motivation for self and partner increased odds of both individual and joint cessation, while discrepancies between motivation levels appeared less influential on joint quitting.
The finding that joint cessation is more dependent on high alignment in the couple’s motivations to quit is supported by findings from prior work conducted by Sterba et al 31 on dyadic efficacy. Dyadic efficacy is defined as partners’ confidence in their ability to quit as a team. 31 In that study, individuals who believed their partner was equally willing to quit reported significantly higher dyadic efficacy scores than those who felt their partner was unwilling. The authors also found that dyadic efficacy predicted both greater individual self-efficacy for quitting and 7-day point prevalence abstinence. 31 Prior research also shows that when one partner improves their health behavior, the other is likely to follow, suggesting that alignment in motivation between partners enhances the likelihood of successful behavior change. This pattern has been observed across multiple health behaviors including physical activity and persists even after accounting for other factors. 15 Taken together, the findings suggest that when partners share a strong desire to quit and commit to a joint effort, they may be able to leverage their relationship for mutual encouragement, leading to higher quit success, at least in the short term. 32
Although motivational misalignment did not consistently influence cessation in our study, it was associated with individual quitting for the more highly motivated partner, consistent with theoretical expectations and prior work.33,34 For instance, longitudinal observational studies show that when one spouse quits successfully, the likelihood that the other will quit increases in subsequent months,33,34 with one study indicating a 4-fold increase in odds of quitting. 33 In such cases, initial misalignment may evolve into alignment as the less-motivated partner’s intentions strengthen in response to the partner’s success and to environmental changes (eg, removal of cigarettes from the household).
The most practically actionable findings emerged from the parallel self-oriented and system-oriented models. The Parallel Self-Oriented Model demonstrates that when both partners are engaged, cessation success is maximized when personal motivations to quit are both high. In practice, this suggests offering joint dyadic cessation programs to couples whose self-oriented motivations are already “in sync.” For pairs in which one partner is less motivated, collaborative goal setting may help foster mutual commitment to quit before initiating cessation treatment. Alternatively, initial efforts can be directed toward supporting the more motivated partner (eg, providing nicotine replacement therapy or individual coaching), while gradually engaging the less motivated partner through shared activities or joint incentives.
The results from the System-Oriented and Shared Target Models inform procedures when the primary need is for one of the individuals to quit smoking. These emphasize that within dual-smoking couples there are times when one person may be ready to quit, and the partner can effectively translate motivation into cessation for that person. In this case, even if the partner's motivation is relatively low, a strong personal drive can still result in successful quitting. To maximize long-term abstinence, turning these individual quit attempts into joint abstinence may be beneficial. Here, one-on-one outreach (eg, phone coaching or brief advice sessions) could use motivational interviewing techniques that probe individuals about their motivations for themselves and motivation for their partners to quit to provide support with the aim to strengthen whichever motivation is weaker.
Our findings also have implications for current smoking cessation services. During cessation counseling, it may be important to assess both partners’ smoking status and their respective motivations to quit. Tailoring services to couples could be beneficial; for example, when an individual seeks Quitline services, the counselor could ask whether their spouse or partner smokes and gauge the partner’s motivation to quit. Following this, the counselor could suggest ways to build mutual commitments through the individual who initiated the call. Incorporating such approaches into clinical settings could foster mutual support and improve the likelihood of sustained abstinence.
Future research should examine the temporal dynamics of each partner’s motivations over the course of treatment to understand how shifts in motivation influence mutual support and social interactions around quitting. It would also be valuable to investigate long-term maintenance
Limitations
Our study has limitations. Agreements in motivation were predominant in the sample; many couples showed either high or low concordance. Situations with greater misalignment may have a higher impact on cessation outcomes. We did not account for changes in motivations to quit over time. Motivations to quit were assessed at baseline in this study. However, the likelihood of this limitation biasing our study estimates was minimized as we adjusted for intervention assignment, which influenced motivation to quit over the subsequent 3 months. Additionally, these data were drawn from a pilot study designed to assess feasibility, tolerability, and preliminary efficacy of financial incentives on smoking cessation. As such, no formal power or sample size calculations were conducted for the secondary outcomes. These secondary findings should therefore be considered exploratory and interpreted with caution. Lastly, the relatively short follow-up period of 3 months is a limitation. Despite short-term abstinence being a strong predictor of long-term abstinence,35,36 some people will relapse after shorter periods of cessation, and this may be particularly true in dual-smoking couples where the lapse of one partner may influence the likelihood the other sustains abstinence. Future studies with extended follow-up will be important to assess how motivations translate into long-term cessation.
Conclusion
The findings highlight the key role of aligned motivations in promoting both individual and dyadic cessation among dual-smoking couples. Couple-based interventions that aim to align and reinforce both partners’ motivations could yield substantially better cessation outcomes in this population.
Supplemental Material
Supplemental Material - Characterizing the Impact of Dyadic Motivations to Quit on Cessation Outcomes in Dual-Smoking Couples
Supplemental Material for Characterizing the Impact of Dyadic Motivations to Quit on Cessation Outcomes in Dual-Smoking Couples by Catherine S. Nagawa, Fangzhi Luo, Ye Shen, James M. MacKillop, Steven R. H. Beach, and Michelle vanDellen in Tobacco Use Insights
Footnotes
Acknowledgments
The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Ethical Consideration
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Institutional Review Board at the University of Georgia (IRB #7344). Informed consent was obtained from all individual participants included in the study.
Author Contributions
Nagawa CS conceptualized the study and drafted the original manuscript; Luo F conducted the formal analyses and contributed to manuscript review and editing; Shen Y secured funding, supervised the formal analyses, and contributed to manuscript review and editing; MacKillop JM secured funding and contributed to manuscript review and editing; Beach SRH secured funding and contributed to manuscript review and editing; vanDellen M secured funding, conceptualized the study, supervised the project, and contributed to manuscript review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Cancer Institute R01CA276594 (PI: vanDellen). JM is supported by the Peter Boris Chair in Addictions Research and a Canada Research Chair in Translational Addiction Research (CRC-2020-00170).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JM is a principal and senior scientist in Beam Diagnostics, Inc. Other authors declare that they have no conflicts of interest.
Trial Registration
The Clinical Trials Registration is NCT #04832260.
Human Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Institutional Review Board at the University of Georgia (IRB #7344).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.