
Abstract
Background
Tobacco usage and obesity remain critical public health issues in the United States. This study examined the relationship between smoking behaviors, specifically—cigarettes per day (CPD) and motivations to smoke—and body mass index (BMI). We hypothesized that motivations related to food or stress, as well as a higher CPD, will be positively associated with BMI.
Methodology
We analyzed the electronic medical records of 204 patients from the Johns Hopkins' Tobacco Treatment and Cancer Screening Clinic (TTCSC) between January and April 2022. Demographic information, smoking behavior, CPD, and motivations to smoke were recorded. Multiple linear regression analysis was performed.
Results
We found no statistical significance between motivations to smoke, CPD, and BMI. However, the age at a patient’s first visit to the TTCSC was negatively associated with BMI (B = −0.152, P < 0.001).
Conclusions
Smoking behaviors were not significantly related to BMI in our sample. It is advisable for clinicians working in tobacco cessation clinics to consider the BMI of individuals who present for cessation services, especially for younger individuals who smoke. They may be more likely to have an elevated BMI at presentation.
Background
Obesity has been prevalent in the United States, where the rate of obesity was 41.9% for adults aged over 20 from 2017 to 2020. 1 Although the rate of tobacco use has declined within the past few decades, approximately 12% of American adults continue to smoke as of 2021. 2 Not only are these public health issues persistent, but they also impose significant health issues when combined. For instance, both tobacco usage and obesity put individuals at greater risk for stroke, diabetes, or heart disease, and current smokers with obesity are at a 3.5 to 5-fold greater risk for all-cause mortality than normal-weight, never-smokers.3,4 Therefore, it is crucial to further examine the relationship between these two public health issues by analyzing how smoking behaviors are related to body mass index (BMI) for patients seeking tobacco cessation management.
Several past studies have investigated the association between the number of cigarettes (eg, cigarettes per day) and BMI. In longitudinal studies, the research compared the BMI among individuals who exhibited different frequencies of smoking and found that smoking was inversely associated with BMI.5-7 Non-longitudinal studies with adult participants from the West Bank and China also showed the aforementioned relationship. 8 However, other research on European adults who smoke observed a positive association between the frequency of smoking and BMI or the risk of obesity.9-12
Individuals’ self-reported motivations that trigger them to smoke may be related to BMI. One motivation is weight loss, where many individuals who smoke believe in the appetite-suppressing and metabolically enhancing effects of cigarettes and, thus, hope that these effects would assist them in losing weight.13-16 Individuals who smoke act on this belief, ultimately experiencing a lower BMI.17-21 On the other hand, individuals may combine smoking with eating because nicotine dependence has been related to experiencing higher food cravings, especially for foods with high fat and sugar content. 22 Along with food, stress is a highly-cited reason to smoke, where research has shown that more than 72% of individuals who smoke utilize smoking as a coping mechanism to deal with stress. The association between stress as a motivation to smoke and BMI has inconsistent results, where several studies have found either a positive or negative association.23-27
There have been only two studies that are specifically targeted to explore how various motivations to smoke may be associated with BMI,28,29 and they used relatively small sample sizes of 6928 and 79 patients. 29 Our study will address these concerns using a relatively larger sample size (n = 204). It will also attempt to clarify the relationships between cigarettes per day (CPD) and motivation to smoke and how both, in turn, affect BMI. In addition, only one of these studies utilized a sample of patients seeking smoking cessation. 28 Therefore, it is vital to continue studying the effects of smoking on BMI for this patient population, as patients hoping to quit smoking are at a higher risk for weight gain and obesity than the general population of individuals who smoke. 30 Therefore, their information when first attempting to quit smoking can be vital for physicians to recognize when attempting to treat these patients.4,31 It is hypothesized that individuals who smoke and cite food or stress as a motivation to smoke at their initial clinic visit for tobacco cessation management will have higher BMI.
Methods
Study participants
All study participants were patients from the Johns Hopkins’ Tobacco Treatment and Cancer Screening Clinic (TTCSC). The electronic medical records (EMR) of 204 patients seen in the clinic from January 2022 to April 2022 were reviewed. Any patient of 18 years or older was eligible for review. We excluded patients who met the following criteria: pregnant, breastfeeding, or in the six-month postpartum period; being currently in receipt of other treatment for smoking cessation or weight control; being diagnosed with a current severe psychiatric disorder, eating disorder, or substance use disorder other than tobacco use disorder; having any health condition requiring a specialized diet or that affected eating (eg, uncontrolled diabetes); or taking medication that affects weight. This study was approved by the Institutional Review Board at the Johns Hopkins School of Medicine (IRB00282725). This was a retrospective chart review of patients enrolled in the Tobacco Treatment Clinic. The review of the clinical notes is performed to understand the clinical utility of the variables in regard to a patient’s smoking phenotype. Such reviews are approved by the Institutional Review Board as a quality improvement project.
Data collection and study design
The initial clinic visit in the TTCSC involved answering a series of questions about tobacco dependence. These variables included the patient’s age when they first started smoking, the number of cigarettes they smoked per day (CPD), and their motivations to smoke. Motivations or triggers were elicited using an open-ended question; patients were not provided with a list of possible responses. Demographic variables were captured by the EMR.
Our outcome of interest was BMI. To most accurately record a patient’s BMI for their initial clinic visit, we utilized the BMI from the EMR on the date of their visit, if available. All patients had their weight captured on the Rice Lake 250 Bariatric Scale, asking for shoes to be removed and being in light clothing. Height was provided verbally by the patient. However, because most patients did not have a BMI recorded on the same day as their initial clinic visit, we allowed for recording a patient’s BMI within three months before or after their initial clinic visit—a reasonable adjustment as most adults gain an average of one to two pounds each year. 28 Patients who did not have a recorded BMI within this timeframe were removed from the sample. A BMI of <25 was considered a normal weight, 25 to 29.9 was overweight, and ≥30 was considered obese.
Our predictors were the motivations to smoke and the number of CPD. Motivations to smoking were categorized into the following: stress, food, coffee, other, time of the day, first thing in the morning, location, social influence, boredom, driving, break at work, and alcohol. For our clinical approach, we do not assess the immediate motivation on any prior scale. Given our strategy is focused on implementation, thinking of small interventions at a time with immediate follow-up, we provide small goals, and if achieved in 4-week, we see this as ongoing motivation to smoking cessation as we wean the patients off of cigarettes and compliant with counseling with or without pharmacotherapy.
Covariates included sex, race, and age at the first visit to TTCSC.
Statistical analysis
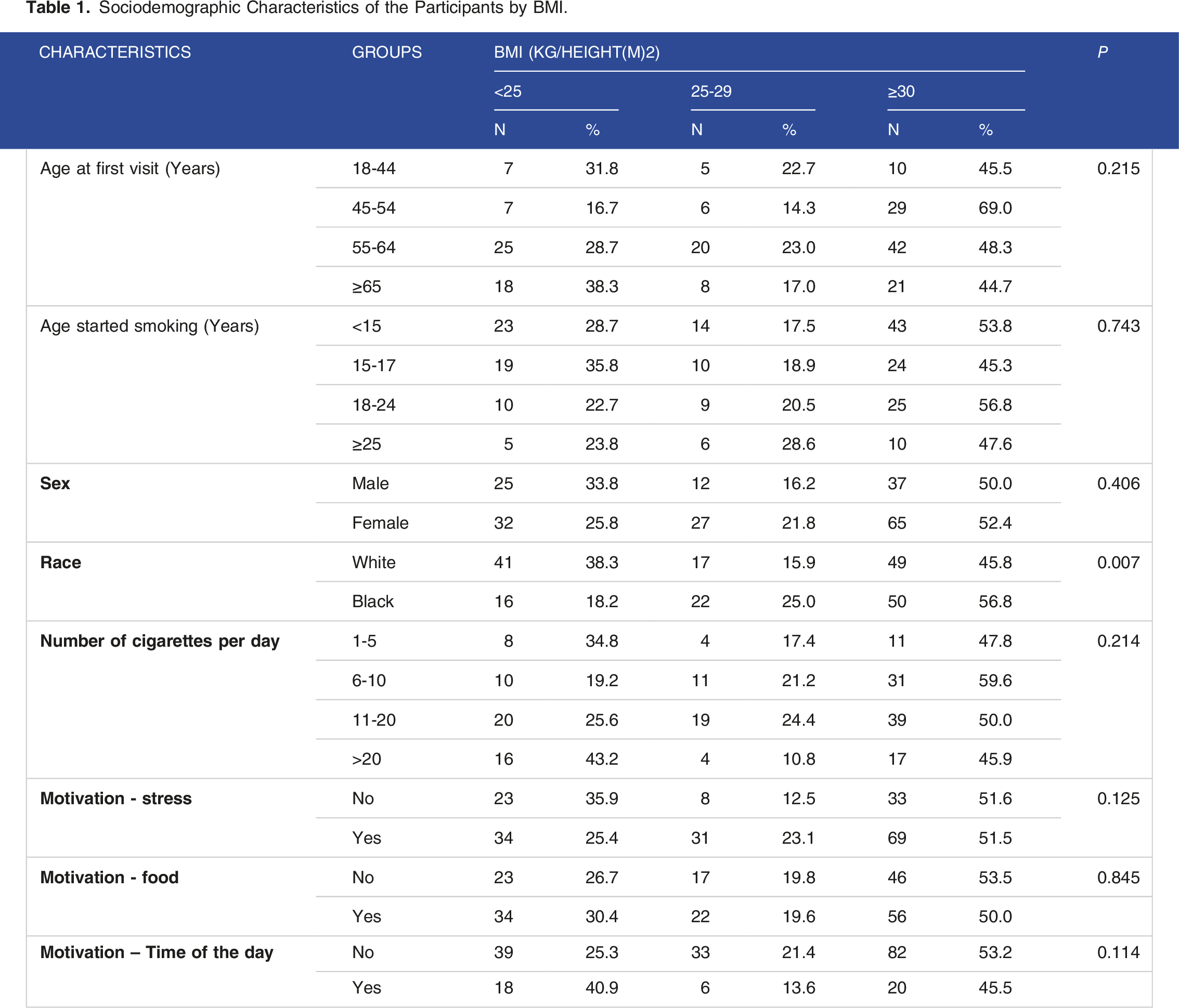
Sociodemographic Characteristics of the Participants by BMI.
Results
Baseline characteristics
Descriptive Statistics of all Variables in the Study.

Note. BMI: Body Mass Index.
Motivations to smoke
Motivation and influence on smoking (n = 204).

Note. aRow percentage (1 person can mention more than one option).
Factors Related to BMI
Factors Affecting BMI of the Participants (Multiple Linear Regression).
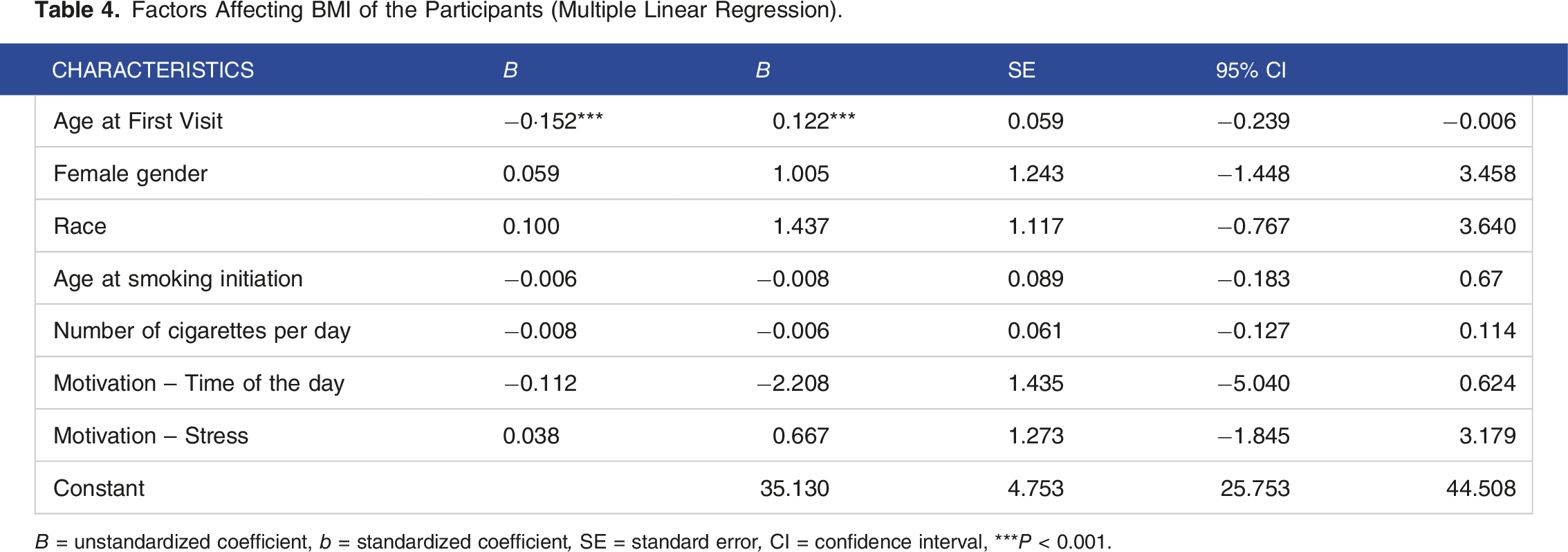
B = unstandardized coefficient, b = standardized coefficient, SE = standard error, CI = confidence interval, ***P < 0.001.
Discussion
The charts of 204 patients seen at the Johns Hopkins’ TTCSC from January to April 2022 were reviewed to assess the relationship between their number of smoked CPD with BMI and their motivations to smoke with BMI. While we hypothesized that the motivators of food and stress, along with the number of CPD, would be positively associated with BMI, this observational cohort study did not show any significant relationship. However, we found that there was a negative association between the age of a patient at their first clinic visit and their BMI.
Although our study did not show statistical significance for the number of CPD and BMI, prior studies have observed an association. For instance, one study analyzing a sample of former individuals who smoke found that the number of CPD was not related to obesity and being overweight for women, but it did for men. 13 It is significant to note, however, that even though CPD may not be consistently correlated with BMI, it may have a strong association with fat accumulation. A study with Saudi Arabians who smoke found that waist circumference and body fat were positively associated with CPD, 33 while no statistical significance was shown with BMI. 34 Similarly, the CPD of Swiss individuals who smoke was related to fat accumulation and not BMI. 35 The mix of studies with varying results on the relationship between CPD and BMI also corroborates the potential bidirectional relationship between smoking and obesity. Cigarette smoking has also been shown to influence metabolism by elevating fatty acids and glycerol levels, which partially explains why quitting smoking can quickly have a positive impact on metabolism. Research by Pezzuto et al (2023) 36 supports this, showing that quitting smoking can lead to improvements in high-density lipoprotein cholesterol and total cholesterol levels. This evidence may also explain why our study did not find a significant link between actively smoking and a decrease in BMI.
Prior literature demonstrates that certain motivations to smoke and BMI are related, although it did not show statistical significance in our study. Numerous studies have reported a wide range of individuals who smoke—adolescents, female high schoolers, college students, general adult women, or those who binge eat—are motivated to smoke because they believe smoking will incline them to consume less food and stimulate their metabolism to burn calories faster.17-21 Therefore, we hypothesized that those who, instead, report food as a motivation to smoke would have a higher BMI. However, due to the contrary results of our study against others in the past, future research may benefit from pursuing this question further, specifically among individuals who smoke and are seeking tobacco cessation management.
We also hypothesized that stress would be positively associated with BMI among individuals who smoke because of research that attests to this presumption. For instance, a paper by Kendzor et al 24 (2014) found that among individuals who smoke in a smoking cessation program, those who experienced more stress due to factors such as a lower income or living in a disadvantaged neighborhood requiring hypervigilance had higher BMI. Furthermore, reduced working hours have lowered BMI for French individuals who smoke, and the authors of this study postulate that it may be due to reduced stress. 25 However, once again, the research on this issue is mixed. Although people living in stressful neighborhoods are more likely to smoke, they tend to have a lower BMI 27 instead of a higher one, prior research has found.24,25 Therefore, stress is not always associated with increased BMI among individuals who smoke and should be further investigated.
As mentioned, we only know of two comprehensive studies that have studied how various motivations to smoke are related to BMI. One of these is by Hovland and Ceballos (2007), whose study examined smoking cessation patients, 28 but a study by Ely et al 29 (2021) examined the same question by utilizing general individuals who smoke. Hovland and Ceballos (2007) observed that normal-weight individuals who smoke were more likely to smoke for tension reduction and the enjoyment of handling a cigarette, but overweight individuals who smoke were more motivated to smoke for stimulation. On the other hand, Ely’s study found that individuals who smoke with higher BMI were less likely to say they smoke for stimulation and indulgence 29 —which is opposite to the results of Hovland and Ceballos’ study (2007). The results of Hovland and Ceballos’ study (2007) have greater applicability to ours as we both utilize individuals who smoke specifically seeking smoking cessation. However, Hovland and Ceballos (2007) collected already-existing participants in a smoking cessation study, meaning that many participants may have changed their motivations to smoke while receiving management. Our study uses information from people’s first clinic visits for cessation management, meaning they have not yet been under the guidance of health care professionals in attempting to quit. Therefore, whether or not individuals who smoke have received ongoing support from clinicians to quit smoking could potentially influence the motivation of individuals who smoke and their BMI.
Another potential explanation for our study results would be that ours may have been impacted by the trend of unintentional weight loss, which is particularly common for older individuals. 37 In fact, unintentional weight loss occurs for 27% of those 65 years and older—a concern as weight loss is associated with increased risk for mortality, difficulty in performing daily functions, poorer quality of life, and hospital complications.37,38 Considering BMI may rise further with the achievement of smoking cessation, clinicians should remain aware of patients’ BMI and age at presentation to counsel on associated risks (eg, cardiovascular disease, diabetes). It is crucial to ensure that patients have proper access to resources for weight management to mitigate the potential for increased risk for chronic conditions associated with a high BMI. Future research should investigate whether smokers’ age has an impact on the likelihood of weight loss or gain following cessation.
While not our primary research question, we did note a statistically significant relationship between increasing age at the initial visit to the TTCSC and lower BMI, suggesting younger individuals who smoke but are attempting to quit smoking may be more vulnerable to having a higher BMI compared to older individuals who smoke. These results may support the general trend of increasing obesity rates for younger adults, where Aggarwal et al (2023) found that the prevalence of obesity rose from 32.7% to 40.9% from 2009 to 2020. 39 The older patients within our study may have also developed chronic diseases that are associated with lower weights, such as chronic obstructive pulmonary disorder (COPD) and cancer.37,38
There are also several limitations of our study. The first is that despite our sample size of n = 204 being larger than those of prior research that investigated the relationship between the motivation to smoke and BMI, a larger sample size is likely needed in future studies to most accurately evaluate the association. Motivations were collected through open-ended responses, which led to high variability within responses since patients were not prompted with ideas for what responses to give, which may have resulted in not capturing the full range of each patient’s motivations. Surveys utilizing already-validated models from prior research might have yielded more standardized responses with less subjectivity on the part of the clinician or data collector. 40
We were unable to account for education level or income, which are known to influence BMI.41,42 Other factors influencing BMI that we did not consider for this analysis include alcohol consumption, psychiatric or other obesogenic medications, weight loss medication, or other lifestyle factors. We suggest studies to account for these limitations to investigate this research question further. We were also unable to use validated tools to evaluate the motivations to quit smoke among participants in our study. Therefore, it is suggested to consider conducting in-depth interviews or using specific sub-scale questions developed by West (2004) to explore a similar research question. 43
Finally, this study was conducted in a single metropolitan area in the U.S. Hence, this study outcome would not be directly applied to other countries outside the U.S. due to differences in social and economic systems. Despite the limitation, our pilot study would allow us to initiate the feasibility and effectiveness of the interventions by contributing to scientific knowledge with updated findings.
Conclusions
Our research emphasizes the significance of taking into account several factors, including weight, when managing smoking cessation. Our study finding indicates that individuals who are concentrating on losing weight may face extra obstacles in quitting smoking because of worries about gaining weight. As a result, health care providers should be aware of these influences when guiding patients on strategies to stop smoking (eg, nicotine replacement therapy and avoiding triggers/stresses). Moreover, providing behavioral interventions that tackle both smoking cessation and weight control concurrently may be a viable option in the medical field. These interventions could assist individuals in overcoming obstacles to quitting smoking while still pursuing their weight loss objectives.
Footnotes
Author contributions
The authors confirm contribution to the paper as follows: study conception and design: J.J.M., P.G.; data collection: P.G., A.E.B., J.J.M.; access and verification of data: B.K., P.G., J.J.M.; analysis and interpretation of results: B.K., J.J.M., A.E.B.; draft manuscript preparation: J.J.M., B.K., A.E.B, P.G. All authors had full access to all the data utilized in this study and accepted responsibility for the final version of the manuscript to be submitted for publication.
Ethical Statement
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.