
Abstract
Introduction
Humans have been using tobacco for centuries, but it didn’t emerge until the 19th century that cigarettes were mass-produced. 1 Since then, cigarette smoking has become a global epidemic. 2 Today, nearly one in three adults worldwide, or approximately 1.1 billion people, are smokers.3-5 Shockingly, around 80% of these smokers reside in low- and middle-income countries.6,7 The total number of smokers is projected to reach approximately 1.6 billion by 2025. 4 As per the World Health Organization’s 2024 report, these statistics reveal a pressing need for immediate action. The prevalence of current cigarette smoking was 17.5% in the United States, 13% in Canada, 11.8% in Australia, and 23% in China. 8 In the same report, the smoking prevalence in Iran was 8.9%, in Saudi Arabia 9.7%, in Egypt 17.9%, in Turkey 27.5%, and in Thailand 19.3%. 8
The health consequences of smoking, in addition to nicotine addiction, include the development of fatal and debilitating diseases and the risk of premature death.9,10 Half of the individuals who smoke long-term will eventually be killed by tobacco, with half of these deaths occurring during their productive middle age, leading to the loss of 20 to 25 years of life. 11 The diseases associated with smoking are well-documented and include lung cancer, cancers of other organs, ischemic heart disease, and other cardiovascular diseases, as well as respiratory diseases such as emphysema and tuberculosis.12-17 Currently, the annual death toll from tobacco use worldwide exceeds 5 million and is expected to rise to over 8 to 10 million by 2030.18,19 More than 80% of these deaths occur in low- and middle-income countries. 20 In Iran, 14% of deaths and 16.3% of all cancer deaths are attributed to cigarette smoking.21-23 What’s more alarming is that these deaths are largely preventable.
In high-income countries, healthcare costs attributable to smoking account for between 6% and 15% of total annual healthcare expenditures.24-26 In low-and middle-income countries, these percentages may not be similar due to the earlier stages of the tobacco-related disease epidemic and other qualitative differences.27-29 However, since cigarette smoking has been increasing in these countries since around 1970, these costs are of significant concern to these governments. The economic burden of smoking is not just a statistic but a call for cost-effective interventions to curb this epidemic.
Non-communicable diseases (NCDs) currently disproportionately affect low-and middle-income countries, where nearly three-quarters of deaths from NCDs (28 million deaths) occur.30,31 According to the World Health Organization, in Iran, 82% of deaths (304 400 people) in 2016 were due to NCDs. 32 The mortality rate was 43% for cardiovascular diseases, 16% for cancers, 4% for chronic respiratory diseases, 4% for diabetes, and 15% for other NCDs. 8 These diseases account for more than 76% of the total burden of disease. Smoking is one of the most significant risk factors associated with the development of NCDs.30,31
According to a comprehensive report by the National Institute of Health Research and the Non-Communicable Diseases Research Center, based on data from the STEPwise survey conducted in 2021, the prevalence of current smokers in Khorasan Razavi was 7.8%, the prevalence of former smokers was 3.7%, and the average number of cigarettes smoked per day was 7.7.33-35 In Iran, approximately 50 billion cigarettes are consumed annually, with nearly 10 trillion rials spent on purchasing this product and two to three times this amount spent on treating related diseases. 36
Taking into account the detrimental and destructive effects of smoking on the country’s economy and noting that prior studies have focused on only a limited range of non-communicable diseases (NCDs), this study seeks to estimate the direct medical costs related to smoking-attributable NCDs in hospitals associated with Mashhad University of Medical Sciences from 2015 to 2023.
Methods
This descriptive-analytical research was conducted as a cross-sectional analysis. It was carried out as a census, examining the records of all patients with NCDs hospitalized in the affiliated hospitals within the specified timeframe, provided their data were available in the hospital information system. The study population includes all patients with smoking-attributable NCDs who were hospitalized in the hospitals affiliated with Mashhad University of Medical Sciences from 2015 to 2023. The hospitals included in the study are Akbar, Ibn Sina, Omolbanin, Omid, Khatam Al-Anbia, Dr Sheikh, Dr Shariati, Kamiab, Hasheminejad, Montaseriyeh, Imam Reza, Ghaem, and Taleghani. All hospitals that were included in the study were affiliated with Mashhad University of Medical Sciences. These hospitals are tertiary referral centers, covering a population of 5 335 433 people. Direct medical costs are funded through basic insurance, supplementary insurance, government contributions, and out-of-pocket payments. The focus on adults aged 35 and above is justified by the fact that the onset of smoking-attributable diseases may take several decades, and the health effects of smoking are cumulative over years of exposure. Consequently, most studies on smoking-related costs concentrate on this age group. 37 This study, therefore, provides a comprehensive understanding of the direct medical costs of smoking-attributable NCDs and their impact on the healthcare system among this age group.
The inclusion criteria for this study were meticulously designed to be comprehensive and representative. Patients must be 35 years or older and hospitalized in one of the hospitals affiliated with Mashhad University of Medical Sciences in Mashhad city. This inclusivity, which specifically included a range of hospitals in Mashhad City, ensures the validity of our study and respects the diverse population affected by smoking-attributable NCDs. On the other hand, patients younger than 35 years old or those admitted to the hospitals of Mashhad University of Medical Sciences outside the city of Mashhad are excluded from the study.
A series of meticulous steps were undertaken to estimate the direct medical costs of smoking-attributable NCDs in hospitals affiliated with Mashhad University of Medical Sciences from 2015 to 2023. This rigorous approach, which included determining the relative risk of mortality from smoking-related NCDs (RRi) based on data from a reference study 38 and extracting the prevalence of current and former smokers in Khorasan Razavi from the Risk Factors Survey in Iran.28,39 The 2021 data was utilized due to the lack of significant difference between the data from 2016 and 2021. The smoking-attributable fraction (SAFij) for NCD mortality was then calculated, representing the proportion of NCD deaths that can be attributed to smoking, and it was categorized by disease and population subgroup. Subsequently, the total direct medical costs of the NCDs under study (THEij) were extracted from the hospital information system, accessed through the Vice-Chancellor for Treatment, covering the period from 2015 to 2023 for the hospitals affiliated with Mashhad University of Medical Sciences. Finally, the direct medical costs attributable to smoking-related NCDs were estimated, ensuring a thorough and reliable research process.
The attributable risk is calculated with the following formula37,40:

The direct medical costs of smoking are the costs of smoking-related diseases, which are obtained by multiplying the attributable risk by the total medical costs of smoking is calculated with the following formula
37
:

Where SAFij is the smoking-attributable risk for disease i in population subgroup j and THEikj is the total cost of disease i with health services of type k in population subgroup j.
The tools used for data collection in this study included hospitalization bills of patients admitted to hospitals affiliated with Mashhad University of Medical Sciences, as recorded in the Hospital Information System (HIS), along with relevant articles and reports.8,21-23 The HIS, a comprehensive and reliable database of patient records and billing information, played a crucial role in this study, providing accurate and detailed data for our analysis. Data collection methods involved accessing the HIS to extract patient demographic details and billing information, reviewing articles to obtain the relative mortality risk for the NCDs under study, and examining related reports to gather prevalence statistics for current and former smokers. For data analysis, the extracted information was input into STATA, categorized by the diseases under study (using ICD-10 codes), prevalence data for current and former smokers by population subgroups, and the relative risk of mortality for the NCDs. The data was coded, categorized, and used to develop formulas to calculate the smoking-attributable fraction and the direct medical costs associated with these diseases, followed by the generation of final reports for each. The software used for analysis included Microsoft Excel 2019 and STATA version 14.
Results
Demographic Characteristics
The Demographic Characteristics of the Patients.

Attributable Risk
The Amount of Attributable Risk by Disease, Gender, and Age Group.

aOther heart diseases include rheumatic heart disease, pulmonary heart disease, and other forms of heart disease.
bOther vascular diseases include atherosclerosis, aortic aneurysm, and other arterial diseases.
cOther cardiovascular diseases are comprised of other heart disease, cerebrovascular disease, and other vascular diseases.
Overall, the data indicates that the attributable risk for smoking-related chronic diseases is consistently higher in males than in females across all age groups. The highest risks were generally observed in the older age groups (65-74 and ≥75), particularly for lung cancer, other vascular diseases, coronary heart disease, and COPD (Figure 1) Attributable Risk by Disease and Gender.
Direct Medical Cost of Non-communicable Diseases Attributed to Smoking
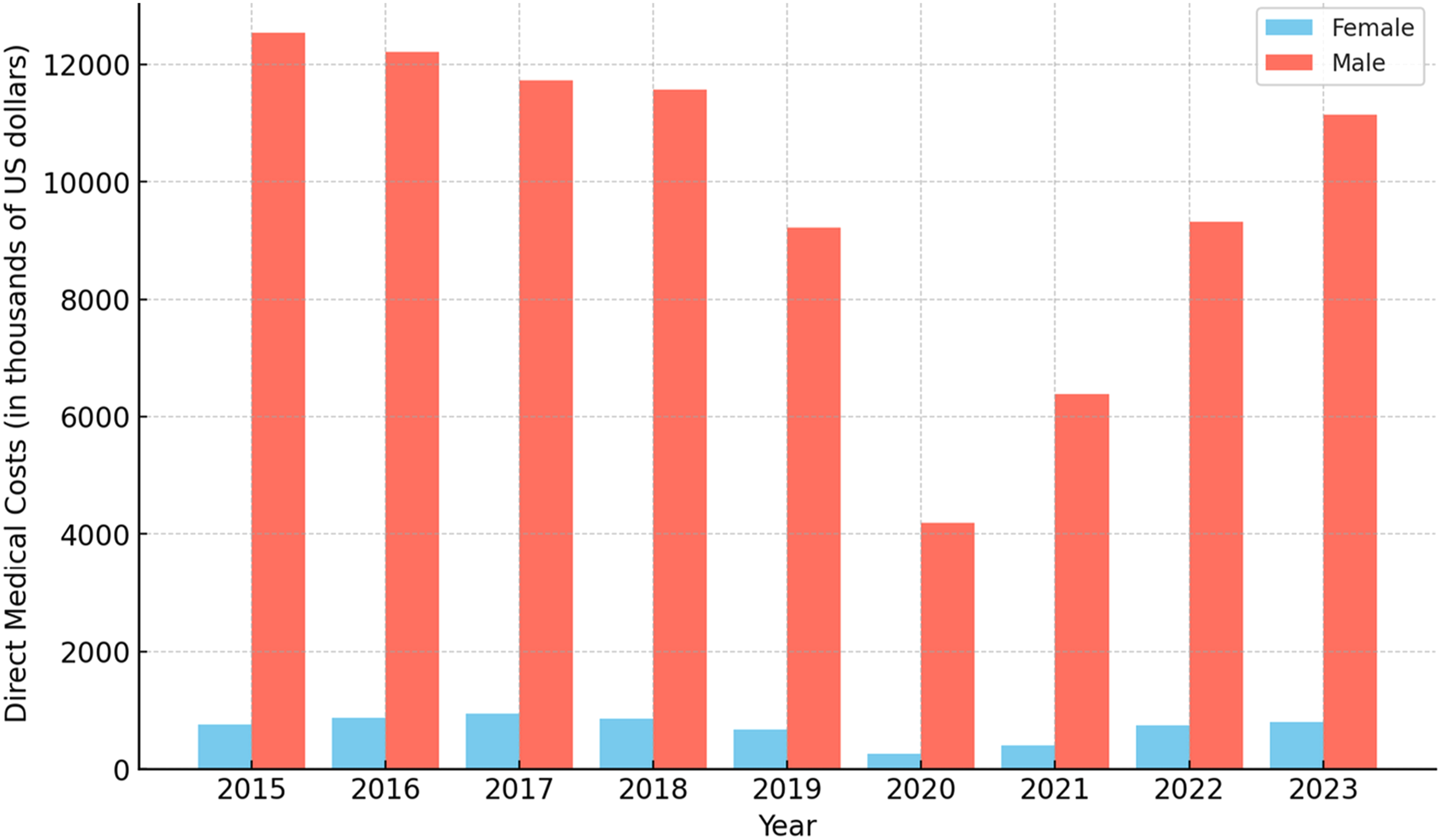
The Direct Medical Costs of Non-communicable Diseases Attributed to Smoking by Disease and Gender in the Years 2014 to 2023 (in Thousands of US Dollars).

The Proportion of Direct Medical Costs Attributed to Smoking by Disease and Gender (2015-2023).
The direct medical costs attributable to smoking-related non-communicable diseases from 2015 to 2023 reveal a stark disparity between male and female patients, with males bearing the overwhelming majority of these costs. Across all disease categories, the total costs for males consistently exceeded those for females, accounting for an average of 93.4% of the total costs, while females contributed just 6.6%. (Figure 3) Trends in Costs Over Time (2015-2023).
In absolute terms, the total direct medical costs for males averaged $9.8 million annually, peaking at $12.5 million in 2015. While considerably lower, the costs for females averaged $0.7 million annually, peaking at $0.9 million in 2017.
Cardiovascular diseases were the costliest category for both genders, but particularly for males, where it accounted for an average of 70.4% of their total smoking-attributable medical costs. In comparison, females spent an average of 3.7% on cardiovascular diseases. Within this category, ischemic heart disease alone constituted 50.5% of the costs for males and 2.6% for females. Respiratory diseases were the second most significant cost driver, particularly COPD, which represented 12.8% of the total costs for males and 2.4% for females. The costs for cancers also demonstrated a substantial gender gap, with males averaging 10.1% of their total costs in this category while females averaged only 0.6%.
The Cost Distribution Analysis for Direct Medical Costs Attributable to Smoking in Public Hospitals From 2015 to 2023.

Discussion
Our study aimed to estimate the direct medical costs of smoking-attributable non-communicable diseases (NCDs) in Mashhad University of Medical Sciences Hospitals from 2015 to 2023. Data from the Non-Communicable Diseases Risk Factors Survey Atlas for 2021 and other studies indicates that the prevalence of current smokers in Khorasan Razavi Province is approximately 10.3%.39,41 Additionally, according to the 2016 National Population and Housing Census data, the population of Mashhad is 3 012 090. 42 Consequently, the number of smokers in Mashhad is estimated to be approximately 240 000 individuals. Given that the average lifetime medical cost for a smoker is approximately $6000 higher than that for a non-smoker, and the life expectancy at birth for smokers is 69.7 years for men and 75.6 years for women, the total annual medical cost per smoker is estimated to be 82.6 dollars.43-45 Thus, the total direct medical costs for smokers in Mashhad amount to approximately 19.3 million dollars.
The findings of other studies on the estimation of smoking-attributable risk in Iran and the associated costs are also aligned with our study.46,47 Still, they may vary in a few sections due to differences in the sources used for relative risk extraction. Moreover, the present study examined 18 diseases or groups of diseases attributable to smoking. The attributable risk for trachea, bronchus, and lung cancer in men in our study is 76.9%. This result is similar to the findings of a study by Varmaghani et al at 75.8% but differs from the results of the study of Rezaei et al at 43.5%.46,47 In women, the attributable risk in the present study is 14.9%, which aligns with the findings of Rezaei et al (11.5%) but differs from those of Varmaghani et al (62.3%). The lower attributable risk in women is due to the lower prevalence of current female smokers compared to male smokers. The attributable risk for ischemic heart disease in men in our study is 24.9%. This is somewhat similar to the findings of Rezaei et al (13.8%) but differs from those of Varmaghani et al (7.4%). In women, the attributable risk in the present study is 2.2%, which is consistent with the estimate by Varmaghani et al (2.4%) but differs from that of Rezaei et al (6.1%). The attributable risk for stroke in men in our study is 16.1%, which is somewhat similar to the findings of Varmaghani et al (11.3%). In women, the risk is 1.0%, which aligns with the results of Varmaghani et al (1.6%). The attributable risk for COPD in men in our study is 68.2%, which is consistent with the findings of Varmaghani et al (67%) but differs from those of Rezaei et al (21.4%). The attributable risk in women in our study is 13.7%, which is relatively similar to the findings of Rezaei et al (9.9%) and somewhat consistent with Varmaghani et al (17.8%).
In the present study, the direct medical costs attributable to smoking for lung cancer, ischemic heart disease, stroke, and COPD in Mashhad in 2016 are estimated to be $10.4 million. In the study by Varmaghani et al. (2016), these costs were estimated at $2 million, which is different from the cost estimates in the present study. 46 However, some costs in our study align with the costs reported by Varmaghani et al in 2016 such as lung cancer and COPD. These results are consistent with those of Rezaei et al in 2014, who estimated the total direct medical costs for lung cancer, ischemic heart disease, and COPD in Iran at $75.7 million (including 4% for lung cancer, 82% for ischemic heart disease, and 14% for COPD). Our estimations for these diseases in 2015 were $254 million (including 5% for lung cancer, 84% for ischemic heart disease, and 11% for COPD). 47
Our study found that the total direct medical costs attributable to smoking for both genders in Mashhad hospitals averaged $10.5 million annually. Significant variations are noted when comparing these costs with similar studies in other regions. For instance, a systematic review of studies in China estimated the direct medical costs of smoking-attributable diseases to range from 9.3 million to 60.0 million dollars, with the most significant proportion allocated to outpatient visits, which accounted for 49.2-68.9% of direct costs. 48 Our study similarly found that the highest costs were for cardiovascular diseases, especially ischemic heart disease, which accounted for 70.4% of the total costs for males. However, unlike the Chinese studies where outpatient costs dominated, our study observed that inpatient costs for chronic conditions like COPD and other heart diseases significantly contributed to the total cost, indicating a difference in healthcare cost structures between these regions. Further, the study by Goodchild et al. in 2018 estimated that globally, healthcare expenditures due to smoking-attributable diseases totaled Purchasing Power Parity (PPP) $467 billion in 2012, which constituted about 5.7% of the global health expenditure. 49 This proportion is comparable to the statistics reported in high-income countries like the United States. (6-8%) but is lower than that in India (4.7%). According to Goodchild et al, in 2018, the cost of diseases attributed to smoking in Iran in 2012 was estimated at $873.2 million (our results were $352.6 million for the country). Our study shows that smoking-attributable healthcare costs in Iran, as represented by data from Mashhad hospitals, might constitute a more substantial portion when considering both inpatient and outpatient costs together. The results of the study conducted by Koronayou and colleagues indicated that the direct medical costs of all smoking-related diseases, including both communicable respiratory diseases and non-communicable diseases (such as cancers, cardiovascular diseases, respiratory diseases, neurological disorders, gastrointestinal diseases, diabetes, musculoskeletal disorders, and physical injuries), amounted to $159 million in Bahrain, $527 million in Kuwait, $222 million in Oman, $246 million in Qatar, $2119 million in Saudi Arabia, and $1150 million in the United Arab Emirates. 50 In the present study, conducted in 2023, the direct medical costs in the country were estimated at approximately $316.7 million. However, it should be noted that this estimate does not include all smoking-attributable diseases, direct non-medical costs, or indirect costs related to smoking.
Our findings revealed a substantial gender disparity in direct medical costs, with males accounting for higher costs compared with females. This is consistent with other studies, such as those conducted in Hong Kong and Taiwan, which also reported higher costs for males.51,52 For example, in Hong Kong, a study by McGhee et al in 2006 found that the direct and indirect costs due to smoking-related diseases were significantly higher among men than women, especially in diseases like lung cancer and COPD. 52 The gender differences are largely due to higher smoking prevalence among men and the associated risk factors that lead to more severe health outcomes.53-55
Our study found that the direct medical costs of smoking-related diseases have been on a declining trend from 2015 to 2020 in Iran. The impact of inflation in the years 2021, 2022, and 2023 has not been uniform across the Iranian economy, with inflation in the healthcare sector, particularly the growth of personnel costs, being lower than in other economic sectors. Despite the significant depreciation of Iran’s official currency during this period, some healthcare costs, such as physician visits, certain nursing expenses, and the procurement of medications for patients, have not increased in line with inflation. This discrepancy has led to a decline in the quality of services provided to patients.6,56 The sharp decline in direct medical costs observed in 2020 can be attributed to the extraordinary economic challenges faced by Iran during this period, particularly the unprecedented devaluation of the Iranian Rial. 57 In 2020, the exchange rate of the Rial to the US dollar experienced a dramatic increase, reflecting heightened economic instability and inflationary pressures. 58 When the healthcare costs, originally incurred in Iranian Rials, are converted to US dollars for analysis, the substantial devaluation of the Rial results in a seemingly significant reduction in the dollar-denominated costs. However, this decline is not representative of the actual healthcare expenditure within the local context. In fact, when assessed in the local currency, healthcare costs for smoking-attributable non-communicable diseases (NCDs) did not decrease; rather, they likely increased due to inflation affecting medical supplies, personnel wages, and healthcare services.
This discrepancy underscores the importance of considering local economic conditions, especially in studies that involve currency conversion for international comparisons. Without accounting for the devaluation of the Rial, the interpretation of trends in direct medical costs could be misleading. Future research on healthcare expenditures in similar economic contexts should account for exchange rate volatility and provide dual analyses in both local currency and standardized international currencies to offer a more accurate depiction of the economic burden.
Our study has several strengths and limitations. One of the key strengths is its comprehensive approach to estimating the direct medical costs of smoking-attributable non-communicable diseases (NCDs) over an extended period of eight years, from 2015 to 2023. This long-term analysis provides a robust overview of the economic burden of smoking on the healthcare system, specifically within the context of hospitals affiliated with Mashhad University of Medical Sciences. The use of extensive hospital information systems and rigorous data collection methods ensured the accuracy and reliability of the findings. The study also utilized a detailed methodology to calculate smoking-attributable fractions (SAFs) and relative risks, allowing for precise cost estimation across different disease categories and demographic groups. Furthermore, by focusing on adults aged 35 and older, the study effectively captured the most impacted population group, where the cumulative effects of smoking over decades are most evident.
However, several limitations should be noted. Firstly, the study is based on data from a single medical university’s affiliated hospitals, which may not fully represent the broader national or regional healthcare landscape. This focus could lead to potential biases in cost estimates, as healthcare practices, costs, and patient demographics can vary significantly across different regions. Secondly, the study primarily relies on direct medical costs. It does not comprehensively address indirect costs such as lost productivity, caregiving, or long-term disability, which are significant components of the overall economic burden of smoking. Additionally, the study did not differentiate between different types of smoking (e.g., active vs passive smoking) or the varying intensity and duration of smoking, which could influence the accuracy of the SAFs and cost estimations. The reliance on secondary data sources for relative risk and prevalence rates may also introduce some uncertainties due to potential variations in study designs and populations in the referenced studies. Another limitation of this study is not conducting a power analysis to determine the minimum sample size, as it aimed to include all eligible hospitalized patients from 2015 to 2023. While this method improves the accuracy of estimating direct medical costs, it could restrict specific statistical analyses for some patient groups. There are also limitations regarding the HIS system. The limitations of the HIS include issues with data accuracy and completeness, which can affect research and clinical decisions. Compatibility problems between different HIS platforms can hinder data sharing. Technological limitations, such as outdated software or hardware, may cause delays or errors. Insufficient user training can lead to data entry mistakes, compromising system effectiveness. Also, Since the HIS only records cost data related to individuals, hospitals, and insurers, and our study was based on utilizing these hospital data without direct access to patients, we were unable to calculate indirect costs. Lastly, the study did not account for possible confounding factors such as comorbidities or socioeconomic status, which could impact both smoking prevalence and healthcare costs. Despite these limitations, our study provides valuable insights into the economic impact of smoking on the healthcare system in Mashhad, the second most populated city in Iran. It highlights the urgent need for effective tobacco control policies and cost-effective interventions.
Conclusion
This research highlights the significant financial burden of cigarette smoking on insurance companies, individuals, and governments, underscoring the need for comprehensive tobacco control policies and targeted interventions, especially among men. One effective strategy to reduce smoking rates is the implementation of higher cigarette taxes, which not only make smoking less affordable but also generate government revenue that can be reinvested in healthcare. Additionally, targeted public health campaigns aimed at high-risk groups can raise awareness of smoking’s dangers and its contribution to non-communicable diseases. Combining these measures with accessible smoking cessation programs can lower smoking rates, reduce healthcare costs, and improve workforce productivity, ultimately easing the financial strain on healthcare systems and improving public health, particularly in lower-middle-income countries like Iran.
Footnotes
Acknowledgments
The authors would like to express their gratitude to all the individuals who helped conduct this study and to all patients for contributing to it.
Ethics Approval
Ethical considerations: The study has been approved by the Ethics Committee of Mashhad University of Medical Sciences, with the code IR.MUMS.FHMPM.REC.1400.084. All participants provided written informed consent forms for the various aspects of data collection. The study was also implemented following the principles and regulations of confidentiality and privacy. All research methods were carried out following relevant guidelines and rules.
Authors’ Contributions
AMT, AA, and MV contributed to the designing and running the model. AMT and AA gathered the required data for the model, including literature review, cost, and efficacy data. AA and MV contributed to the study’s statistical and epidemiological parts and double-checked all analyses. AMT, ZK, MM, and AA wrote the manuscript. JM, FSH, and MV reviewed the manuscript and double-checked all the analyses. All authors participated in reviewing the manuscript and its revision, and they were involved in research, interpretation, and finalizing the manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study’s findings are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Transparency Statement
The lead author, Dr Mehdi Varmaghani, affirms that this manuscript is an honest, accurate, and transparent account of the study being reported, that no important aspects of the study have been omitted, and that any discrepancies from the study as planned (and if relevant, registered) havebeen explained. All authors have read and approved the final version of the manuscript. Dr Mehdi Varmaghani, the corresponding author, had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.