
Abstract
Objective
To estimate the economic costs of selected tobacco-related illnesses (TRI) in Kenya in 2022.
Research Design and Methods
This study was conducted in 2 phases. Phase 1, conducted between 2021 and 2022, entailed conducting a cross-sectional study conducted in 4 national public referral hospitals in Kenya. Patients with cardiovascular disease, cancer, chronic obstructive pulmonary disease, or tuberculosis were interviewed to compute the indirect and direct medical costs related to the illness. Activity-Based Costing approach was used to capture costs for services along the continuum of care pathway. In the second phase, the Tobacco Attributable Factor was used to estimate the direct, indirect, and ultimately economic cost due to tobacco smoking.
Results
The estimated health care cost attributed to tobacco use in Kenya is US$396,107,364. Among TRIs included in the study, myocardial infarction had the highest health care cost at US$158,687,627, followed by peripheral arterial disease and stroke with health care cost of US$64,723,181 and US$44,746,700 respectively. The main cost driver across all the illnesses is the cost for medication accounting for over 90% of the total health care cost. The productivity losses from the diseases ranged between US$148 to US$360 and accounted for 27% to 48% of the economic costs. The total cost attributable to tobacco use to Kenya’s economy for the selected TRIs was between US$544.74 million and US$756.22 million.
Conclusions/interpretation
Tobacco related illnesses impose a significant economic burden as reported for direct and indirect costs. These findings underscore the need for strengthened implementation of the provision of the Framework Convention on Tobacco Control and the Tobacco Control Act (2007) to facilitate a reduction in tobacco consumption in the population.
Keywords
Introduction
Tobacco use contributes to the risk factor of developing many Non-Communicable Diseases. The high prevalence of tobacco use among adults aged 15 years and above in Kenya poses a notable public health issue, with 11.6% reported as tobacco users. Notably, there is a gender disparity, as the rate of tobacco use is much higher among men, with 19.1% using tobacco products compared to only 4.5% of women. Furthermore, 7.8% of adults smoke tobacco, while 4.5% use smokeless tobacco. 1 Among youth aged 13 to 15, 9.9% use tobacco products, with boys exhibiting a higher prevalence at 12.8% compared to 6.7% among girls. Additionally, 4.9% of youth in this age group smoke cigarettes, with boys again showing a higher rate at 7.4% vs 2.6% for girls. Similarly, 3.9% of youth use smokeless tobacco, with a slightly higher prevalence among boys at 4.3% compared to 3.3% for girls. 2
Smoking and other forms of tobacco use impose economic costs on societies through healthcare and productivity losses. Eighty percent of these deaths occur in low- and middle-income countries (LMICs). 3 In addition to the impact on health, the effects of tobacco transcend other sectors such as agriculture and the environment. In the absence of tobacco control measures developing countries will face higher tobacco-related healthcare spending in the future, 4 which will further exacerbate the already overburdened healthcare systems in these countries. Several studies have attempted to quantify the economic loss of tobacco consumption globally and in some sub-Saharan African countries. On a global scale, smoking has been shown to account for 1.8% of the worldwide gross domestic product. 5 Regrettably, 40% of these economic losses occur in low- and middle-income countries (LMICs), with a substantial proportion of these expenses borne by individuals of lower socioeconomic status. Additionally, smoking is responsible for 15% of all direct healthcare costs in high-income countries. 6 Taiwan however has reported lower proportions where smoking and SHS accounted for 4.3% of the direct healthcare expenditure. 7 The aggregate total economic costs of smoking represent a significant loss for the whole economy, reaching 2.1%–3.4% of gross domestic product (GDP) in Australia, 1.3%– 2.2% of GDP in Canada, and 1.4%–1.6% of GDP in the United States. 8 There is scanty data regarding tobacco economic costs in Africa. In South Africa, the financial impact of smoking was found to be 0.97% of the GDP The healthcare expenses associated with smoking-related diseases accounted for 4.1% of the overall health expenditure in South Africa. 9 A study in Uganda found that tobacco use totaled to 0.5% of the GDP. The estimated health cost of tobacco use accounted for 4.1% of the total health expenditure, as a percentage of the GDP. 10
A study in the USA reported that the economic losses from cigarette smoking, totaling $864.5 billion, greatly exceeded the income generated from cigarette sales, which amounted to $94.2 billion, at a ratio of nearly ten to 1 in terms of the net economic impact of tobacco consumption. 11 Proponents of the economic benefits of tobacco have always argued that tobacco generates substantial revenue to countries through taxation, sale of products and provision of employment. The significance of tobacco production, manufacture and retailing to country’s economy is usually amplified by the tobacco industry to justify their demands against tobacco control interventions. 12 However, many of these arguments fail to account for huge costs resulting from morbidity and mortality from tobacco-related diseases.
Economic effects of smokeless tobacco are equally devastating with smokeless-related cancer estimated to cost 0.45% of GDP in Sri Lanka and the cost of Bidis use estimated to be 0.48% of GDP in India. 13 Regarding economic costs associated with illness due to secondhand smoking (SHS), 14 a study done in 6 Asian countries found that cost due to SHS accounted for 20.4% of all the cost associated with tobacco consumption. This translated to approximately 0.21% of the combined GDP in these countries. 15 In Greece, SHS accounted for 8.9% of the total tobacco economic costs translating to 0.356% of the GDP. 16 This is similar to what was found in Taiwan where the proportion attributed to SHS was 8% of the total economic costs. In China, SHS was responsible for 0.3% of the total health care costs with approximately $559 million for outpatient visits and $612.4 million for inpatients in 2011. 17 In Greece the highest proportion of morbidity costs were from musculoskeletal diseases for smoking and diabetes for SHS. 16 These studies have shown that tobacco use presents many externalities in society. Smokeless tobacco use can also have indirect economic impacts through externalities, such as environmental costs and an increased burden on social welfare systems. The production, distribution, and disposal of smokeless tobacco products may have environmental consequences that require additional resources for mitigation or remediation. Heart disease emerged as the costliest disease associated with SHS in China. 17 The type of diseases with the highest direct economic cost due to smoking varies according to geographic location and disease burden. Diabetes and respiratory diseases were found to be the major contributor of morbidity costs associated with tobacco-related illnesses in Asia. 15 The economic impact of tobacco consumption in India represents roughly 1.04% of the country’s gross domestic product (GDP), with the excise tax revenue generated from tobacco sales in the previous year accounting for a mere 12.2% of these economic costs. Specifically, the direct medical expenses attributable to tobacco use make up 5.3% of the overall healthcare expenditure. The substantial financial burden placed on India’s healthcare system by tobacco-related illnesses has the potential to overwhelm public health resources and place strain on the economy, highlighting the urgent need for significant expansion of tobacco control initiatives in the country. 18 In Indonesia, the 2019 economic cost of smoking ranged from Rp 184.36 trillion to Rp 410.76 trillion (1.16%-2.59% of the gross domestic product). 19 Each year, smoking in Argentina results in 45,000 fatalities and 221,000 health incidents, leading to a financial burden of USD2782 million in direct healthcare expenditures, USD1470 million in costs related to decreased labor productivity, and USD1069 million in expenses associated with informal caregiving. This amounts to 1.2% of the country’s gross domestic product. 20
While evidence shows tobacco has economic effects to countries, the economic effects of tobacco vary across countries driven by unique characteristics facing the country such as prevalence of tobacco use, disease epidemiology and economic structure. In developing countries, the economic burdens of tobacco use are reduced compared to developed nations because of lower healthcare and labor costs, as well as lower levels of employment. These costs are higher in high-income countries due to the large size of the population and workforce affected, lost productivity and premature mortality, and the associated healthcare cost. 5
It is essential to assess the country-specific implications of tobacco consumption in developing nations to support and direct policy actions on tobacco regulation and oversight. Estimating the economic impacts of tobacco use in Kenya is crucial for guiding policy decisions based on evidence. This highlights the actual expenses linked to tobacco use and offers a factual foundation for defining the necessary policy measures to address the adverse effects of tobacco use, encompassing both health and economic costs. It also sheds light on the repercussions that nonsmokers may face due to secondhand smoke, with an estimated 600,000 deaths annually attributed to this cause. 21 Moreover, the population of these countries carries the financial load resulting from tobacco-related illnesses on the public healthcare system, irrespective of their smoking habits. By quantifying the economic impact of tobacco use, a more comprehensive examination of the repercussions of tobacco consumption on the economy becomes possible. These measures are also for advancing global development objectives outlined in the Sustainable Development Goals (SDGs). The findings of this study will catalyze urgent and effective policy actions, driving meaningful progress toward public health and sustainable development on a global scale.
This study is the first comprehensive economic analysis that documents the costs of selected Tobacco Related Illnesses (TRI) in Kenya and the percentage of these expenses that can be attributed to tobacco consumption. Using the Activity-Based Costing (ABC) approach, this study offers insights into costs arising from tobacco use in Kenya. The study provides detailed estimates of both healthcare costs and productivity losses from tobacco use in Kenya. In addition, the analysis fills the information gap on economic effects of tobacco in LMICs, especially in Sub-Saharan Africa since majority of existing studies are from high-income countries.
Methods
Estimating the size of the population with TRIs
Diseases characteristics.

This study used a two-stage mixed sampling strategy combining purposive and random sampling methods. First, 4 referral hospitals were purposively selected as they represent the main hospitals providing services to the illnesses being costed. The second stage included random selection of the patients containing the selected TRI. Patient records from both outpatient and inpatient departments were initially screened to identify individuals with tobacco-related illnesses. Daily reviews of inpatient and outpatient registers were conducted across all relevant wards and clinics in the selected healthcare facilities during the study period to identify any new patients with tobacco-related illnesses. The study included all patients aged 18 years and above in specialty clinics, surgery and medicine wards, and those who met the inclusion criteria. Patients who did not provide consent or had severe incapacitation were deemed ineligible to participate in the study. The inpatient and out-patient registers were reviewed daily in all the relevant wards and clinics during the study period. For outpatient, the study targeted all the adult outpatient specialty clinics, surgery and medicine wards and all patients who met the criteria.
Study design
This study was a cross-sectional analysis of the cost of illness in Kenya, conducted at the 4 main tertiary hospitals: Kenyatta National Hospital (KNH), Moi Teaching and Referral Hospital (MTRH), Kenyatta National Hospital-Othaya Referral Hospital (KNH-ORH), and Kenyatta University Teaching, Referral, and Research Hospital (KUTRRH), between 2021 and 2022. These facilities were selected because they attend to patients with the 4 study conditions (Cancer, CVD, COPD and tuberculosis) within their inpatient and out-patient departments. Patients with CVD, cancer, COPD, or TB were interviewed using a preformed questionnaire which included the patient’s demographic details, the type of tobacco use, indirect and direct medical costs related to the illness. The direct costs included costs of medicines, consumables, diagnostics, and personnel, travel and subsistence, materials and supplies, rent, utilities, maintenance expenses, other recurrent, furniture & equipment, operational equipment, insurance and other services. The indirect costs were costs associated with lost productivity due to these TRIs.
Study procedures
Two research assistants gathered data at the hospitals involved in the study. They underwent training on the standardized data collection tool, study protocol, and procedures. Following the training, a pilot test of the study procedures was carried out. Prior to commencing data collection, the research team introduced the study to the hospital management teams and departments. A visit was made to the health facility study sites to evaluate the feasibility of conducting the research. The team requested cooperation from the hospital authorities to facilitate the implementation. Quality checks were performed daily to identify inconsistencies, incomplete information, and conflicting responses.
The following data collection tools were used; (a) Key informant interview guide for CVDs, COPDs, selected cancers and pulmonary TB (b) Process maps for adaption (c) Client exit survey (d) Facility cost data collection tool
The collection was done online via phones or tablets and using ODK platform.
Data analysis
The study utilized Statistical Package for Social Sciences (SPSS version 23.0) and Statistical Application Software (SAS version 9.0) for analysis. The data analysis process involved creating service pathway maps, estimating inputs for each service per patient, quantifying resource capacity and cost, calculating unit costs per visit, and determining client economic costs. Client exit survey responses were used to compute economic costs, including out-of-pocket expenses, transportation costs, and opportunity costs. The total cost of patient care was calculated by multiplying resource costs by usage time and adding equipment and supplies costs. Direct health costs were integrated with mortality and morbidity costs to assess economic burden. Indirect costs were included, along with the economic impact of tobacco use using the Tobacco Attributable Factor (TAF). The study evaluated the overall impact of tobacco on the economy by considering government tax revenue and contributions, aiming to determine the net societal cost of tobacco use.
Cost of illness estimation
The economic cost of tobacco was estimated based on the cross-section data capturing cost of care, and productivity losses as estimated based on the data collected through client exit interview/survey.
Healthcare cost
The following types of costs were derived for this study. • Staff Cost: This included expenses associated with the healthcare professional involved in treating the TRI such as salaries, wages, benefits, and any other costs related to staffing, such as training and recruitment. • Consumables Cost: This included the cost of consumable items used in the treatment of the TRI. We included items such as medical supplies, disposable equipment, laboratory tests, and other materials directly consumed during the provision of healthcare services. • Medicines Cost: This represented the expenses associated with the medications prescribed for the treatment of TRI. We included the cost of pharmaceutical products, drugs, and any related supplies necessary for medication administration. • Overhead Costs: These were indirect expenses that were not directly tied to TRI but were necessary for the overall functioning of the healthcare system. These costs included administrative expenses, utilities, facility maintenance, and other general operational costs. • Capital Costs: These included the expenses associated with acquiring and maintaining capital assets used in the treatment of TRI eg, the cost of medical equipment, infrastructure, facilities, and any long-term investments required to support the provision of healthcare services.
Activity-Based Costing approach was used to capture costs for services relating to CVD, COPD, selected cancers, and pulmonary TB at the facility level. Activity-based costing approach is a patient-centered approach that allow measurement of all the resources including health care workers, equipment, medications, and consumables used to provide the patients with their required health services. 22
The activity-based costing approach consists of the following steps: Selecting medical conditions under each of the 4 broad areas of CVDs, COPD, selected cancers and pulmonary TB; defining the care delivery value chain: - charting out all the activities in the entire cycle in the provision of health care services; creating process maps for each activity in the delivery of health services – recording every administrative and clinical process involved in the care of the chosen medical condition; obtaining the time spent and resource used in serving a patient at each point through the entire service chain to arrive at time estimates for each process; estimating the expense of supplying patient care resources, which includes direct and indirect care costs, as well as overhead and support center costs; estimating the capacity of each resource and calculating the capacity cost rate and the total cost of patient care per disease.
Productivity losses
The health care cost was combined with the mortality and morbidity cost to estimate the economics cost for the TRIs diseases. Mortality loss was estimated based on the lost productivity attributable to reduced productivity due to years lost as a result of premature death. While the morbidity loss was based on estimated lost output due to absenteeism from work – here the person did not go to work; lost output due to presenteeism – here the person went to work alright but because of sickness they cannot function efficiently, inability to produce optimally on account morbidity of the from the TRIs.
Productivity losses arising from morbidity and premature death were estimated based on the Disability adjusted life years (DALYs) from TRIs. The DALYs were estimated by
The DALYs = YLL + YLD
YLD = DW*Prevalence or number of cases
YLL = Remaining years of life at the time of death based on life expectancy * number of deaths observed
Total economic cost of tobacco consumption
To estimate the total economic cost the direct cost (cost related to health cost) and indirect cost (cost related to lost productivity) were added to get the economic cost of each of the disease. The Tobacco Attributable Factor (TAF) was used to estimate the direct, indirect, and ultimately economic cost attributable to tobacco use. The Tobacco Attributable Fraction (TAF) represents the percentage of health risks, healthcare service utilization, healthcare expenses, deaths, or other health consequences that can be linked to tobacco use. In Kenya, the TAF for each specific disease was determined by calculating the morbidity and mortality associated with tobacco use within the 4 designated disease categories.
In the SAMMEC method, the number of deaths attributable to each cause of mortality was computed using the following formula:
Mortality attributable to tobacco smoking or smoking attributable mortality (SAM) is the product of observed mortality (OM) and Tobacco attributable fraction (TAF) and PAF is bases on formulae by Levin [10]
The use of the TAF enabled estimation of the net and economic cost of tobacco use by netting off the effect of other variables that affect tobacco related diseases. The TAF for each TRIs was multiplied with the total economics cost of tobacco to get the economic cost attributable to tobacco use.
Economic Benefits from tobacco
The total contribution to the economy by the tobacco industry is captured as aggregate tobacco revenue in the country across the production and consumption system. This is also reflected as country Gross Domestic Product contribution from the tobacco industry. Thus, the revenue accruing to the leaf farmers, cigarette retailers and wholesalers, manufacturers, taxes, and all other groups within the production and supply chain. The total GDP attributable to the whole tobacco industry was sourced from the Economic survey, 2022. 23 This approach was applied to quantify the gross and net economic benefits of tobacco use in the markets. The proportion of selected TRIs to the burden of Tobacco use was multiplied with the total economic benefits of tobacco use to get the economic benefits attributable to tobacco use. Kenya GDP is $105 Billion with tobacco industry contributing 7% of GDP equivalent to $7.1 Million, 24 the selected TRIs account for 34.35% of GDP attributable to tobacco industry equivalent to $2.5 Million.
Cost and benefits from tobacco
The study adopted a simple cost and benefit framework, making use of estimated total gain vs the benefits of tobacco use to generate the cost benefit ratio. The ROI was established by comparing the benefits vs the costs. We quantified the ROI by estimating monetized DALYs based on a constant value per statistical life year (VSLY) derived from a VSL estimate. There is uncertainty in VSL, and it does not represent the inherent value of life but condenses actual and stated trade-offs people make in choosing between money and small changes in mortal risk. The VSLY is provided by the residue of life expectancy and age of death. We used the Value of Statistical Life-Year for Kenya which is Ksh. 358,567. Both costs and benefits were discounted at a yearly rate of 3%, in line with economic principles and guidelines. 25
Ethical considerations
The study received ethical approval from the Kenyatta National Hospital-University of Nairobi Research and Ethics Committee (KNH/ERC/R/168) and the Moi University/Moi Teaching and Referral Hospital Institutional Research and Ethics Committee (IREC Number FAN 0003954).
Results
Disease characteristics
Oral-pharyngeal cancer was the most common disease among the TRIs, accounting for 36% of cases, followed by nasopharyngeal cancer at 12% and lung cancer at 10%. Peripheral arterial diseases had the lowest representation. Just over a quarter of patients had additional comorbidities, and one-third of patients required hospitalization. Most patients (52%) had been diagnosed with the TRIs in the last 5 years. See Table 1 below.
Healthcare expenditures attributed to TRIs
Total annual healthcare cost by TRIs, (in US Dollars).
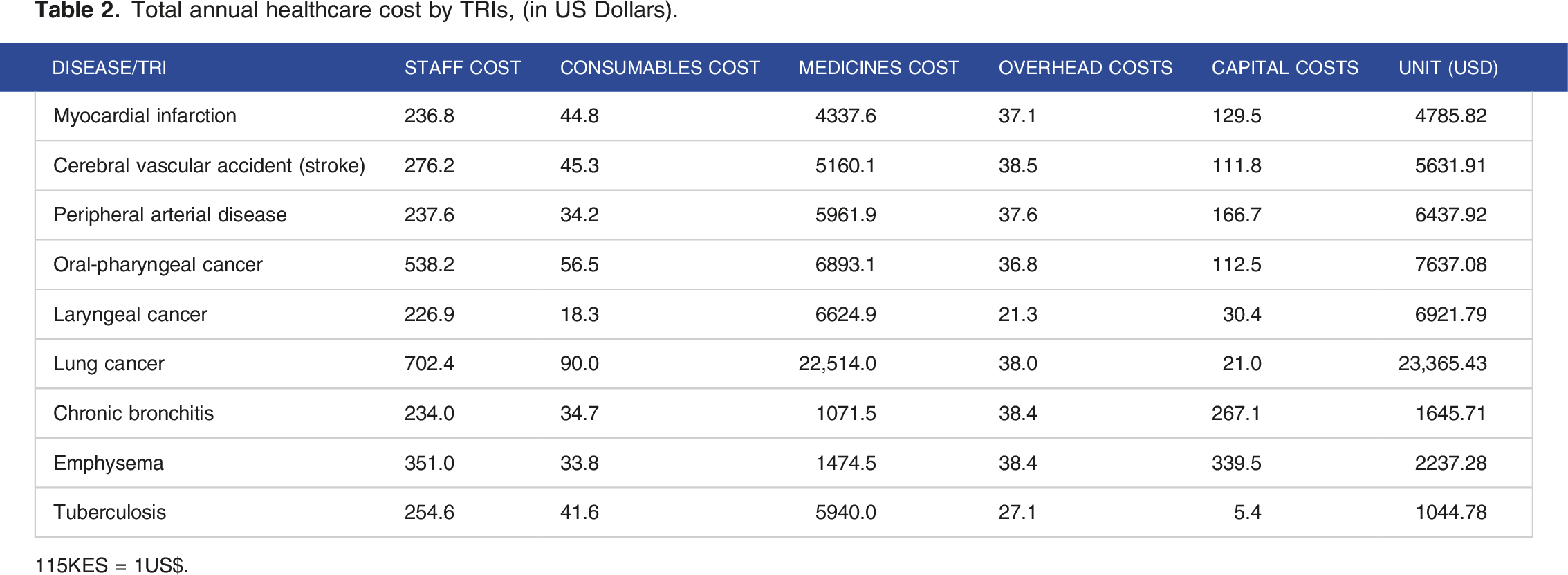
115KES = 1US$.

Distribution of Total Healthcare cost by Cost categories.
Future economic burden of Tobacco Related illnesses
Total disability adjusted life years gained.

Annual monetized burden (DALYs) of TRIs (in USD).

Health care cost attributable to tobacco use by TRI (in USD).

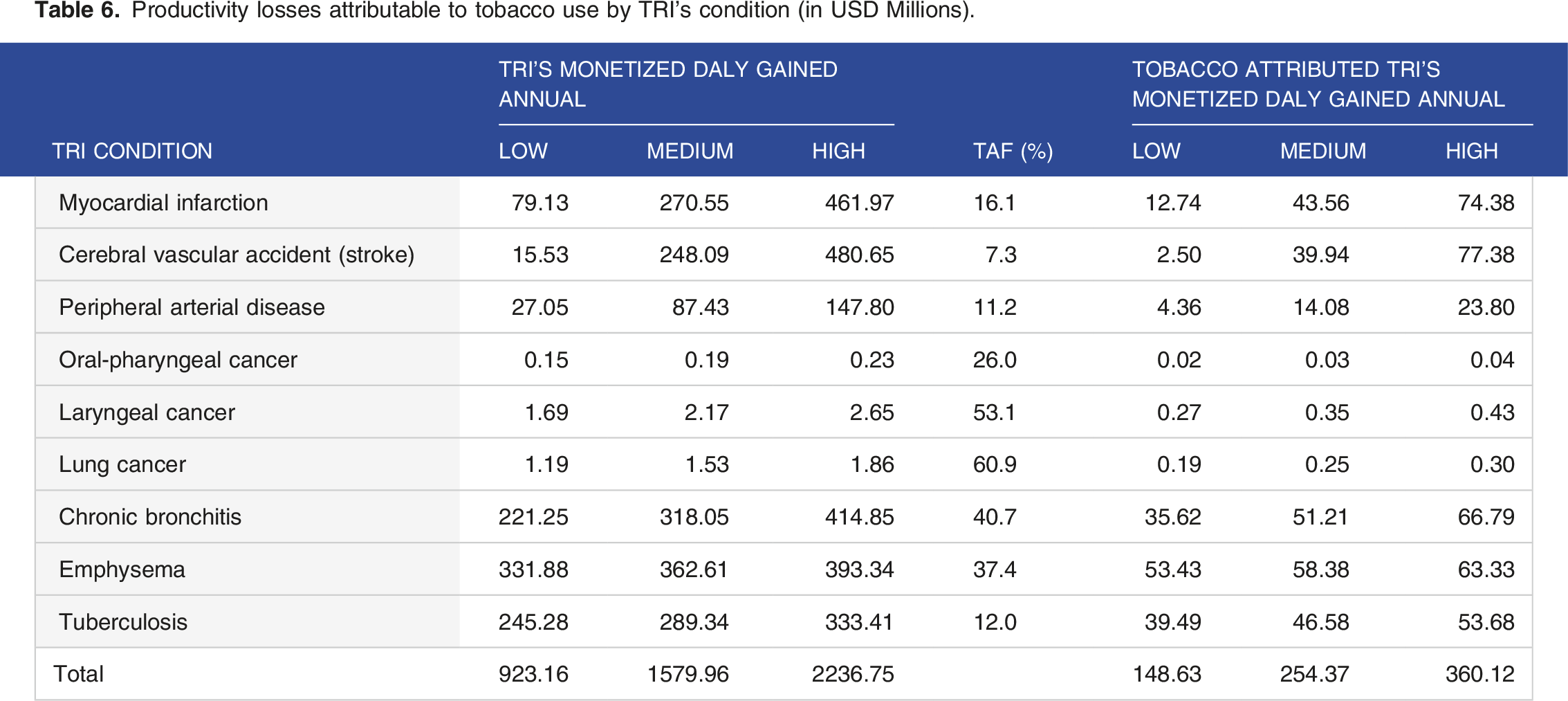
Productivity losses attributable to tobacco use by TRI’s condition (in USD Millions).
Total Economic Cost of Tobacco Use in Kenya (in USD Millions).

Cost benefit analysis
In 2022, the tobacco industry’s revenue was $7.35 Million. This represented 7.0 % of Kenya’s GDP of $105 Billion in the same year. At the same time, selected TRIs attributable economic cost of tobacco use (Table 6) account for 34.35% of tobacco industry’s revenue (Share of GDP form the tobacco industry).
In a simple cost and benefit framework, we found that the financial impact of tobacco use in Kenya ranges from US$544.74 million and US$756.22 million, while the tobacco industry’s contribution to GDP (benefit from tobacco industry) was $252.93 Million.
Net impact of tobacco use in the markets based on costs attributable to selected TRIs, 2022. (In USD Millions).

Discussion
The costs presented are for the period between 2021 and 2022. Our analysis found that treating and managing TRIs included in the study in Kenya presents enormous cost to the health system. The total cost of treating TRIs is estimated at $2.8 Billion. Of these costs, we estimate that $396.1 Million is linked to tobacco use, accounting for 14% of the total expenses associated with treating and handling the TRIs. The economic burden of tobacco use falls within the range of $544.74 million and $756.22 Million The economic implications of tobacco consumption in Kenya is slightly less than what has been found in South Africa (US$2.88 billion) but more than what was found in Uganda (USD126.48 million). 9 The variances can be clarified by the differences in smoking rates and the prevalence of Tobacco-Related Illnesses (TRIs) among the countries.
For every dollar received in the tobacco industry, the economy loses $2.2 to $3. Similar findings have been found in previous studies. 10 This essentially demonstrates that revenue accrued by the entire tobacco economy is less than the cost to the economy. This net loss is a likely underestimation as it does not consider other losses experienced in the tobacco production chain such as illnesses associated with tobacco farming and factory injuries. This notable net loss is a strong indication of the need for the government to fully implement the Tobacco control law of 2007 28 and the recommendations of the WHO FCTC 29 paying close attention to law enforcement and fiscal measures such as raising the excise tax on tobacco products. Moreover, as stipulated by the tobacco regulations of 2014, the country now receives 2% solatium compensation contribution from tobacco products that are either manufactured or imported to the country and these funds should be used to strengthen tobacco cessation programs and other prevention programs. 30
There were variations seen in terms of health cost attributed to tobacco use for each disease with myocardial infarction having the highest healthcare cost at US$158,687,627 and the least health care cost found in Oropharyngeal cancer at US$119,139. Studies done elsewhere attribute the highest health care cost to different diseases, for example lung cancer in Argentina and musculo-skeletal diseases in Greece, which reflects the differences in the burden of the diseases and the maturity levels of the health system between countries. The care all, the total healthcare expenses linked to tobacco use in our study was found to be US$396,107,364. Our findings are consistent with what was found in various Latin American countries. 31 In India a higher health cost of US$6.05 billion was reported and the difference could be explained by the higher prevalence of tobacco use in India. 14
Further analysis indicated that most of the healthcare costs were related to the costs of medicines ranging from 65% to 95% of the total healthcare costs of treating and managing TRIs. A higher proportion of capital costs was seen in health care costs for chronic respiratory diseases: chronic bronchitis and emphysema. The high health care costs found in our study underpins the importance of prevention programs to reduce the use of tobacco in the population. This will have an overall effect reducing the costs to both the patient and healthcare system in the long term. Key to note is that in Kenya, out of pocket expenditures (OOPs) contributes to 20% of the financing schemes for NCDs. Cessation and prevention programs will reduce OOPs. 32
The results attest to substantial productivity losses ranging between US$148.63 million and US$360.12 million, showing that ultimately society bears a significant brunt of tobacco use that translates to economic losses. When compared to direct health care cost, productivity costs accounted for between 27% and 48% of the overall financial burdens associated with tobacco use in Kenya. This is consistent with what was found in Tanzania 33 but is in contrast to India 14 where the 78% of the total economic costs attributed to tobacco use were accounted for by indirect costs. 34 The divergent results can be explained by the difference in methodology used and the fact that generally health care cost in Kenya remain significantly high. 35 Nevertheless, these productivity losses can be averted by strengthening the current tobacco control initiatives in Kenya.
Limitations of the study
This cost estimate is conservative and likely underestimates the true burden of tobacco use for the following reasons: • The estimate does not account for intangible costs like pain and suffering, care provided by informal caregivers, and administrative costs of insurers. • The analysis focuses only on healthcare expenditures where usage patterns differ between individuals with Tobacco-Related Illnesses (TRIs) and those without TRIs, potentially excluding areas where people with TRIs may utilize services at higher rates. • Variations in the average cost of health services based on TRI status are not factored in. If individuals with TRIs tend to use more expensive health services, the cost estimate may be too low. • The study addresses differences in healthcare utilization related to TRIs, such as the number of hospital inpatient days, but does not consider variations in the types of healthcare professionals seen (eg, specialists vs primary care physicians). • Individuals with undiagnosed TRIs are categorized with the non-TRI population in the study. If those with undiagnosed TRIs use more healthcare services per capita than those without TRIs, the healthcare costs attributed to TRIs may be underestimated.
Subsequent research could explore the expenses related to Tobacco-Related Illnesses (TRIs) in the areas overlooked in the current analysis. The national cost estimate of TRIs was determined using prevalence-based cost-of-illness methods, incorporating data from client medical record reviews and client exit surveys. Various data sources were examined for certain cost components (eg, supply costs), and the findings were cross-referenced to ensure the reliability of the results.
Conclusions
Tobacco use exerts a notable economic influence on Kenya, ranging from between US$$544.74 million and US$756.22 million. This economic analysis further highlights that for every dollar received by the tobacco industry in the form of revenue, the economy loses US$2.2 to US$3. These findings underscore the need for strengthened implementation of the provision of the WHO FCTC and the Tobacco Control Act to facilitate a reduction in tobacco use in the population. In particular, measures such as increasing excise tax on tobacco products, strengthening cessation programs, enhancing the capacity of law enforcement agencies to combat illicit trade in tobacco and education of the public on the harms of tobacco use need to be prioritized.
Reducing tobacco use is crucial for global public health goals, as outlined in the Sustainable Development Goals (SDGs), particularly SDG 3 focusing on healthy lives and well-being. Tobacco use is a major cause of non-communicable diseases, leading to high morbidity and mortality rates worldwide. Lowering tobacco consumption can reduce NCD burden, cut healthcare costs, and enhance population health, in line with SDG 3 objectives. Moreover, this effort supports SDG 1 by potentially alleviating poverty and SDG 12 by promoting sustainable practices. Addressing tobacco use is vital for nurturing a healthier, more sustainable future aligned with the broader SDGs agenda.
Implementing effective tobacco control measures in Kenya necessitates a collaborative effort between governmental and non-governmental entities. The government should lead in developing and enforcing comprehensive tobacco control policies in line with the WHO Framework Convention on Tobacco Control, including measures like increased tobacco taxes and graphic health warnings. NGOs can support by advocating for policies, conducting research, and raising awareness. Governmental enforcement units should monitor compliance, with NGOs aiding in awareness campaigns and oversight. Joint public awareness initiatives should educate on tobacco risks and cessation services. The government should provide accessible cessation services, while NGOs offer counseling and support groups. Monitoring and evaluation of measures is crucial, with the government collecting data and NGOs assisting in research. Through collaboration, both sectors can effectively implement tobacco control measures in Kenya, leading to better public health outcomes and reduced tobacco-related diseases.
Policy implications
Implementation of tobacco control measures in Kenya requires a multi-faceted approach involving both governmental and non-governmental entities. The Kenyan government can take proactive steps such as passing comprehensive tobacco control legislation, enforcing existing laws, and increasing taxes on tobacco products to reduce affordability and accessibility. Governmental bodies can also collaborate with non-governmental organizations (NGOs) to raise awareness about the health risks of tobacco use through educational campaigns and community outreach programs. NGOs can play a crucial role in advocating for policy change, providing cessation support services, and monitoring the tobacco industry’s activities to ensure compliance with regulations.
Several barriers may impede the effective implementation of tobacco control measures in Kenya, including industry interference, lack of political will, and limited resources for enforcement. To overcome these challenges, it is essential to strengthen collaboration between relevant stakeholders, increase public awareness through media campaigns, and engage with policymakers to prioritize tobacco control on the national agenda. Additionally, capacity building efforts to enhance enforcement mechanisms and training for healthcare professionals on tobacco cessation interventions can help mitigate these barriers. Developing partnerships with international organizations and leveraging their expertise and resources can also support the successful implementation of tobacco control policies in Kenya.
The impact of implementing comprehensive tobacco control measures in Kenya could lead to a significant reduction in tobacco-related morbidity and mortality, improved public health outcomes, and a decrease in healthcare costs associated with treating tobacco-related illnesses. By aligning with global best practices and evidence-based strategies, Kenya can strengthen its tobacco control policies and regulations to create a healthier environment for its citizens. Furthermore, the findings of such initiatives can inform the development of new policies, such as smoke-free laws in public spaces, stricter advertising restrictions, and enhanced support for tobacco cessation programs.
Footnotes
Acknowledgements
We thank Development Gateway for facilitating the study. We wish to acknowledge the contribution of Dr Caroline Mithi, Rachel Kittony and Winnie Awour who provided technical inputs for analysis of this paper.
Author’s contribution
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.