
Abstract
Introduction
Tobacco use is one of the leading causes of preventable deaths, responsible for more than 7 million deaths per year worldwide, among which 890,000 deaths are attributable to second-hand smoking. 1 Research has demonstrated that tobacco smoking increases the risk of heart disease, respiratory diseases, and cancer. 1 Between 1990 and 2019, North Africa, the Middle East, and sub-Saharan Africa had the most significant relative increase in the number of smokers among both males and females. 2
Adolescents have been the target of the tobacco industry over the years, with almost 90% of present smokers starting smoking before the age of 18, 3 with at least one in every ten adolescents between the ages of 13 and 15 using tobacco products worldwide. 1 Report findings from the WHO Global Health Observatory showed that the prevalence of adolescent students that currently smoke cigarettes around the world is 19.33%, with higher tobacco use among male adolescents. 4
Adolescents go through a challenging transitional period between childhood and adulthood, involving biological, psychological, and social changes that play an essential role in their development5,6 and enabling sensation-seeking and risk-taking behaviors. 7 These behaviors are shaped heavily by their surrounding environment and peer influence that either approve or discourage actions. 8 Although adolescents are affected by peer behaviors and influence, parents and family members’ actions can also indirectly promote risky behaviors, acting as role models to the developing adolescent.9,10 Thus, adolescence is a vulnerable and risky period, and the behaviors initiated at this stage are more likely to be passed into adulthood.7,8
Iraq has been going through a challenging period of war conflicts and economic crises for the past three decades, traumatically affecting the Iraqi community, especially its younger youth population.11,12 The post-war conflict’s psychosocial and mental health trauma contributed to increased vulnerability to drug and substance use among the population. 12 It is evident that there is a marked increase in rate of Iraqi adolescent tobacco smoking in the past decade. A previous analysis of Iraq GYTS data in 2012 that estimated the prevalence as 21.8%, 13 while a recent study done in Erbil, Iraq in 2019 estimated the prevalence of cigarette smoking among adolescents to be 27.6%. 14 This is in spite of the 2012 anti-smoking laws that prohibits smoking in public places and selling tobacco to those who are less than 18 years old. Research using the Global School-based Student Health Survey reported an overall prevalence of smoking cigarettes of 19.4% among teenagers (13-17 years) in the Eastern Mediterranean Region; 28.2% and 10.7% among boys and girls, respectively. 15 Specifically among Iraqi teenagers, the overall prevalence of smoking was 18.6%; 25.2% and 9.9% among boys and girls, respectively. 15 Not many studies looked at adolescents’ current E-cigarette use, especially in the middle east region. The rise in tobacco smoking rates among adolescents could be caused by low socioeconomic status post-war conflicts, accompanied with psychological factors and nicotine addiction.12,16
Strong social networks, family influence and respect to teachers are long term features of the culture in Iraq and the Middle East Region. Understating how such relationships influence the behavior of adolescent re-smoking is imperative. Against this background, we aim to assess the potential relationship between family and teachers’ smoking behaviors on that of Iraqi adolescents attending schools. We hypothesize that adolescents whose parents or teachers smoke will have higher rates of tobacco use.
Methods
Study design, sampling, and survey
Data analyses were conducted on the data from the Iraq Global Youth Tobacco Survey (GYTS) data for the year 2019. GYTS is a cross-sectional and nationally representative survey of students attending schools, conducted by the World Health Organization (WHO), and US Centers for Disease Control and Prevention (CDC). The survey, originally developed in English, was translated to Arabic and back translated to ensure it accuracy. It uses a global standardized methodology, employing a two-stage sample design. The inclusion criteria for school selection in the GYTS included both public and private schools in all geographic areas of Iraq. The inclusion criteria for class selection in the GYTS comprised of classes that generally encompass boys and girls 13-15 years of age. 17 Schools are selected with a probability that is proportional to enrollment size in the first stage. Classes are then randomly selected in the second stage, granting all students eligibility to participate in the survey. More information concerning the GYTS questionnaire and methodology can be accessed under the WHO website. 18
In Iraq, the cross-sectional survey was administered by the Ministry of Health and WHO to a total of 2560 adolescents. With such a sample size the study is able to estimate any prevalence to within a margin of error of at most ±2% using 95% confidence interval. The overall response rate was 89%. Necessary ethical approvals were obtained by the national authorities such as Ministries of Public Health and Education. Parental consent was obtained and students were informed that participation was voluntary and that by filling the questionnaire they were giving their assent.
The GYTS is a self-administered questionnaire that includes 43 core questions related demographics, socio-economic status, tobacco use, cessation, second-hand smoke, access and availability of tobacco products, media and advertisements, knowledge, and attitudes. 19 In addition, countries can opt to ask about other forms of tobacco use, such as shisha use, smokeless tobacco, or E-cigarettes. The survey is anonymous and self-administered using paper-based bubble sheets that are scannable.
Measures
For this study, there were two outcome variables: current use of any tobacco product and current use of E-cigarettes. Current use of any tobacco product was defined using the GYTS questions such as “During the past 30 days, on how many days did you smoke cigarettes”, as well as the other tobacco products including shisha, pipe, cigars, hand-rolled tobacco, and smokeless tobacco. Participants who responded with >=1 day of smoking were considered current tobacco users, while responses with 0 days were considered not current tobacco smokers. Current use of E-cigarettes was defined using the following question “During the past 30 days, on how many days did you use electronic cigarettes?” Similarly, responses with >=1 day were considered current E-cigarette smokers, while responses with 0 days were considered not current E-cigarette smokers.
The four exposure variables assessed in this study included exposure to smoking at home, exposure to smoking at school, participant’s attitudes toward tobacco use, and knowledge of tobacco use. Questions regarding exposure smoking at home included the following four questions: 1) “How often do you see your father (stepfather or mother’s partner) smoking in your home?”, 2) “How often do you see your mother (stepmother or father’s partner) smoking in your home?”, 3) “How often do you see your brother/sister smoking in your home?”, and 4) How often do you see other people smoking in your home?”. Answers “about every day” and “sometimes” were coded as “yes” to questions 1 through 4, “never” was coded as “no”, and “don’t have/don’t see this person” were kept the same. Questions regarding exposure to smoking at school included the following three questions: 1) “During the past 30 days, did you see anyone smoke inside the school building or in the school yard (inside school walls)?”, 2) “During school hours, how often do you see teachers smoking in the school building?”, and 3) “During school hours, how often do you see teachers smoking outdoors on school premises?”. Answers to question 1 were reported as “yes” and “no”. Questions 2 and 3 were combined into one exposure named “Any teachers smoking on school premises” with responses of “about every day” and “sometimes” coded as “yes”, “never” coded as “no”, and “don't know” kept the same. Adolescents’ attitudes towards tobacco smoking were assessed using the following seven questions: 1) “Are you in favor of banning smoking inside enclosed public places (such as schools, shops, restaurants, markets, cars)?”, 2) “Are you in favor of banning smoking at outdoor public places (such as playgrounds, streets, gardens, parks)?”, 3) “Do you think tobacco advertising should be banned?”, 4) “Do you think the sale of tobacco products to minors should be banned?”, 5) “Do you believe that tobacco companies try to get young people under age 18 to use tobacco products?”, 6) “Do you think smoking tobacco helps people feel more comfortable or less comfortable at celebrations, parties, or in other social gatherings?”, and 7) “Do you think smoking shisha helps people feel more comfortable or less comfortable at celebrations, parties, or in other social gatherings?”. For questions 1 through 5, participants who responded with “yes”, “definitely yes”, and “probably yes” were given a score of 1, while participants who responded with “no”, “definitely no”, and “probably no” were given a score of 0. For questions 6 and 7, participants who responded with “less comfortable” were given a score of 1, while participants who responded with “more comfortable” and “no difference” were given a score of 0. Scores of all seven questions were summed to yield an attitude score between 0 and 7. A higher score indicated more conservative/negative attitudes towards tobacco use. Adolescents’ knowledge about tobacco smoking was assessed using the following three questions: 1) “Do you think the smoke from other people's tobacco smoking is harmful to you?”, 2) “Once someone has started smoking tobacco, do you think it would be difficult for them to quit?”, and 3) “Do you think the smoke from other people's shisha smoking is harmful to you?”. Participants who responded with “yes”, “definitely yes”, and “probably yes” were given a score of 1, while participants who responded with “no”, “definitely no”, and “probably no” were given a score of 0. Scores of all three questions were summed to yield a knowledge score between 0 and 3. A higher score indicated more knowledge about tobacco use.
Demographic variables included age, sex, grade level, and weekly money to spend. Ages of study participants ranged from 11 to 17 years old; due to having very few patients in some categories, those in ages 11 to 13 were grouped and reported as “≤13 years old.” Weekly spending money was based on the question “During an average week, how much money do you have that you can spend on yourself, however you want?” and ranged from <3000 to >14,000 Iraq Dinar (IQD), equivalent to approximately <2.63 to >12.30 U.S. Dollars (USD) respectively using the conversion rate of 1 USD = 1138 IQD during the time of data collection. 20 Due to small frequency in higher categories, those spending more than 10,000 IQD, equivalent to 8.79 USD, were grouped and reported as “more than 10,000 IQD.”
Statistical analysis
Frequency distributions were used to summarize demographic variables such as age group and gender while means and standard deviations (SD) were used for numeric variables. The main outcomes were summarized using frequency distributions along with 95% confidence intervals using the Wald Method. Crude associations between demographic and exposure variables and the two main outcomes were estimated using univariate logistic regression. Covariates with P-values ≤0.2 in univariate regression analysis were included in the multivariable models. Odds ratios (OR) and adjusted odds ratios (AOR) with their 95% confidence intervals (CI) and P-values are presented. Significance was set at the 5% level. Data analyses were conducted using IBM-SPSS (version 26, Armonk, New York, USA).
Ethical approval
This study uses publicly available anonymized GYTS data, thus it was not required to obtain a separate ethical approval from the authors’ institution.
Results
The Frequencies of Demographic Measures and Exposure to Smoking at Home and School Among 2560 Iraqi Adolescents Attending Schools.

Table 1 also reports the frequencies of adolescents’ exposure to second-hand smoking at home and school and the prevalence of current use of any type of tobacco and E-cigarettes. Around 40% of the students reported seeing their fathers smoke, while 13.9% reported seeing their mothers smoke. About a quarter of students stated their siblings smoke (23.9%), and more than half of reported other individuals smoke at home (56.1%). The percentage of students who witnessed people smoking within school premises was 45.7%, and more than half of students observed teachers smoking in schools (57.6%).
Prevalence Estimates of Current Use of Any Type of Tobacco and E-Cigarettes Among 2560 Surveyed Iraqi Adolescents Attending Schools.

CI: Confidence Interval.
Attitudes and Knowledge Towards Tobacco Use Among 2560 Iraqi Adolescents Attending Schools.
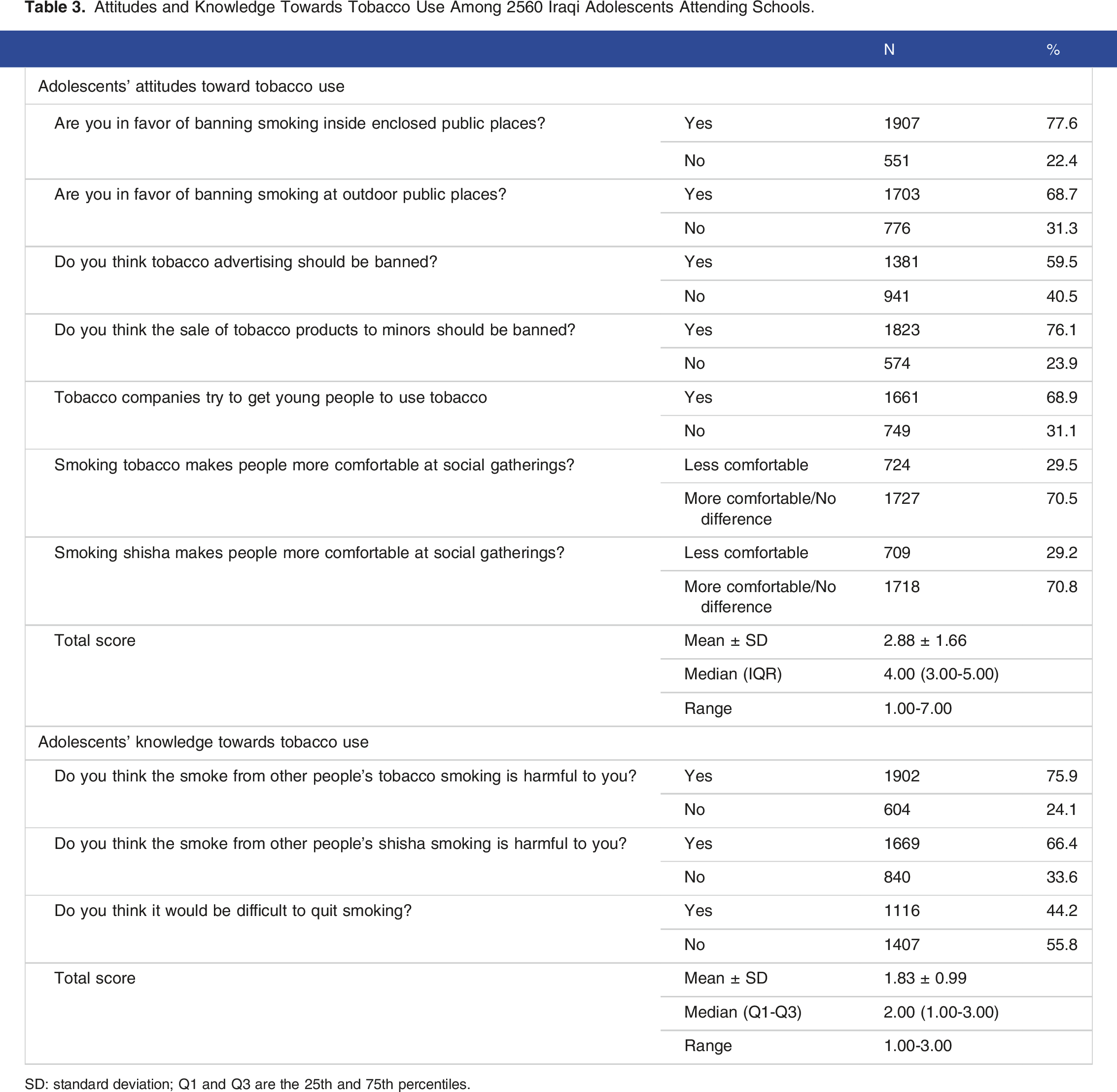
SD: standard deviation; Q1 and Q3 are the 25th and 75th percentiles.
Univariate and Multivariate Logistic Regression Analyses Assessing the Association Between Exposure to Smoking and Any Current Tobacco Use, Adjusting for Demographic Factors, Attitude and Knowledge Sum Scores Towards Tobacco Smoking.

SD: standard deviation; OR: odds ratio; AOR: adjusted odds ratio; CI: confidence interval.
Exposure to family members’ smoking habits was highly associated with increased susceptibility to tobacco smoking. Compared to adolescents with non-smoking fathers and mothers, adolescents with fathers and mothers who smoke had significantly higher odds of using tobacco products with an AOR of 1.39 (95% CI: 1.05-1.85) and 1.84 (95% CI: 1.30-2.60) respectively. Additionally, adolescents with siblings who smoke tobacco had significantly higher odds of tobacco smoking, 3.50 (95% CI: 2.62-4.67) times that of adolescents with non-smoking siblings. Students who observed people and teachers smoking within school premises were significantly associated with increased tobacco use compared to students who did not, with an AOR of 1.99 (95% CI: 1.57-2.53) for other people smoking in school and an AOR of 1.48 (95% CI: 1.10-1.98) for observing teachers smoking. Students with lower attitude (AOR = 0.81; 95% CI: 0.76-0.87) and knowledge (AOR = 0.81; 95% CI; 0.72-0.91) sum scores were significantly correlated with the current use of any tobacco product.
Univariate and Multivariate Logistic Regression Analyses Assessing the Association Between Exposure to Smoking and Current E-Cigarettes Use, Adjusting for Demographic Factors, Attitude and Knowledge Sum Scores Towards E-Cigarettes Smoking.

SD: standard deviation; OR: odds ratio; AOR: adjusted odds ratio; CI: confidence interval.
Discussion
The study demonstrated that the prevalence of any form of tobacco smoking among adolescents in Iraq was 30.3%, while E-cigarette smoking was 9.7%. Cigarettes were the main form of tobacco used, followed by cigars and shisha. The strongest predictors of tobacco and E-cigarette smoking among adolescents were male gender, siblings smoking, and people smoking at school. Adolescents with attitudes against smoking were at less risk of smoking tobacco or E-cigarettes, while more knowledgeable adolescents were at more risk of smoking tobacco smokers only.
Male adolescents were at almost double the risk of being tobacco or E-cigarette smokers compared to females. Previous study in Erbil city in Iraq indicated that the strongest predictors of cigarette smoking was male gender. 14 Gender differences in smoking prevalence for tobacco and E-cigarettes can be attributed to societal and cultural values in Iraq. The Iraqi Kurdistan culture consider smoking as taboo for both genders but would turn a blind eye and tolerate male smoking compared to female smoking behaviors.21-23 This is due to deeply embedded patriarchal beliefs that places less judgement on men and their views and practices, while women are criticized and condemned for the same practices. This pattern is also seen in Arab countries, such as Syria, where the most common reason women reported not being smokers was traditions and social norms. 24
Adolescents of low socioeconomic status were less likely to smoke tobacco or E-cigarettes, suggesting that adolescents with higher weekly spending money could be smokers. A study based in Iraq had similar findings and proposed that access to spending money could help adolescents obtain cigarettes. 23 Along with access to money, lack or poor enforcement of banning tobacco sale to minors makes it easy for adolescents to obtain tobacco products. 21
Siblings have an even stronger influence on adolescent tobacco and E-cigarette smoking habits compared to parents; adolescents with smoking siblings were found to be about three times more likely to smoke tobacco or E-cigarettes. A 2021 study in Saudi Arabia demonstrated that adolescents who have smoking siblings had seven times more risk to smoke tobacco, and six more the risk of tobacco smoking intension. 25 The strong association between adolescents smoking frequency and siblings influence could be attributed to the shared environment and social connectedness that siblings share. 26 Thus, adolescents who live in and share the same environment as their siblings are more likely to acquire similar habits, and in turn picking up similar smoking habits as their siblings.
Exposure to parental and teacher smoking proved to increase risk of adolescent tobacco and E-cigarette smoking. Two studies, conducted in Lebanon 27 and Morocco, 28 reported increased risk of adolescent tobacco smoking with exposure to parental tobacco smoking. The research conducted using the GSHS survey in the Eastern Mediterranean Region reported a significant association between parental smoking (father, mother, or both) with cigarette smoking among teenagers with an AOR of 1.3 (95% CI 1.21-1.41). 15 Teachers smoking in schools was also associated with higher risk of tobacco smoking among adolescents, as daily exposure to teachers’ smoking on school premises had higher impact on student smoking behaviors than having a parent who smokes.27-30 With the rate of teachers smoking in schools being higher than that of parents, it is imperative that policy-makers implement smoke-free schools in Iraq, reducing exposure and influence to smoking since the current 2012 anti-smoking law allows for schools to have a designated smoking area away from the sight of nonsmokers. Growing adolescents are influenced by people that they view as authoritative figures, such as parents and teachers, and attempt to imitate their behaviors.8,31 This observation can be explained by the Social Learning Theory, indicating that social behavior is acquired from observing and imitating the behaviors of role models. 31 Negative attitudes notably decreased the likelihood of tobacco and E-cigarette smoking, yet knowledge plays a larger role in influencing tobacco use among adolescents. An Iraq-based study reported that adolescents with strongly negative attitudes towards E-cigarettes would consume them nonetheless. 21 This is attributed to the lack of information and awareness of E-cigarette use in the community, as adolescents believed E-cigarettes impose less harm than traditional cigarettes. 21 The lack of knowledge was positively associated with adolescents being more susceptible to E-cigarette usage. Despite that, due to the limited number of knowledge questions regarding E-cigarettes included in the study, it is difficult to draw concrete conclusions regarding the effect of knowledge on adolescents’ E-cigarette smoking habits.
The GYTS survey had a large, representative sample of adolescents attending schools in Iraq, and included diverse questions regarding different types of tobacco and E-cigarette use. This is the first study to our knowledge that investigated the parents’ and teachers’ smoking habits and their association with adolescents’ tobacco and E-cigarette use. Previous studies looked at the relationship but not the statistical association and impact on adolescents.
One of the study limitations was that adolescents’ tobacco and E-cigarette use was self-reported and that students might have under reported their smoking habits, specifically female students due to cultural taboo and societal disapproval of females smoking tobacco. The GYTS school survey is only limited to adolescents attending schools, overlooking students who are not enrolled in school due to poor socio-economic status post-war conflicts. 32 Children and adolescents are dropping out of schools and engaging in child labor to support their families, putting education at a lower priority. 32 The effects of these circumstances on adolescents’ smoking habits need to be further investigated. Another limitation was the use of data dating back to 2019 while attending the rapidly changing societal context, particularly concerning the strategies of tobacco companies and the prevalence of tobacco prevention and control measures.
Additionally, the study is a secondary analysis of preexisting data from the WHO GYTS, therefore could not assess the effect of stressors and mental health factors of adolescents on tobacco and E-cigarette use. Another limitation is that the survey included a small number of attitude and knowledge questions limited to tobacco smoking only and few on shisha smoking, but not including other types of tobacco or E-cigarettes. The study could not assess if family, friends, or teachers aid adolescents in obtaining tobacco products; it would have given more insight of family and friends involvement in enabling adolescents to consume tobacco. Moreover, the cross-sectional nature of the study design doesn’t allow for inferring causality.
Conclusion
In conclusion, one in three Iraqi adolescents attending school reported using tobacco, while one in ten reported smoking E-cigarette smoking. Exposure to family and teachers smoking demonstrated significant associations with adolescent smoking. As such, policy makers should enforce stricter policies to ensure safer school environments that do not expose adolescents to smoking habits of teachers or other students. Furthermore, this study indicated a rise in tobacco smoking rates among adolescents from 21% in 2012 to 30% in 2019, which could be influenced by post-war conflicts, accompanied with psychological factors and nicotine addiction. Investigating post-war mental health effect on adolescents is worth looking at as well as investigating its effects on tobacco smoking and other health-related behaviors. There is no existing policy or law regulating public indoor E-cigarette use in Iraq. More studies, taking into consideration all above limitations, on E-cigarette use in Iraq and its prevalence can assist and directs policymakers to implement interventions that can help tackle the issue and reduce public indoor E-cigarette smoking in the future, especially in educational institutions and schools.
Footnotes
Acknowledgements
The authors thank the division of Medical Education at Weill Cornell Medicine in Qatar for funding the publication of this article.
Author contributions
Concept and study design: ZRM; Data acquisition: ZRM; Data analysis: FAB, SRD; Data interpretation: FAB, SRD, ZRM; Drafting of the manuscript: FAB, SRD; Final Review: FAB, SRD, ZRM.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper uses data from the Global Youth Tobacco Survey (GYTS). GYTS is supported by the World Health Organization and the US Centers for Disease Control and Prevention.
Ethical Statement
Data availability statement
The dataset and code book associated with the core GYTS questionnaire modules are made available to the public on the WHO and CDC websites. Data from core-expanded questions and country-specific questions are not made public. No school or student identifiers are included in the public use dataset (![]() ).
).