
Abstract
The 12-item Smoking Self-Efficacy Questionnaire (SEQ-12) is a valid and reliable instrument to assess confidence in one’s ability to refrain from smoking in a variety of different situations. This study evaluated the psychometric properties of the Spanish version of the 12-item Smoking Self-Efficacy Questionnaire (SEQ-12) among a sample of Spanish-speaking Latino smokers engaged in a smoking cessation research study. A forward-backward translation procedure guided the translation of the SEQ-12 into Spanish. The Spanish version of the SEQ-12 showed promising internal consistency reliability and construct validity among Latino smokers, with potential applications in both research and clinical settings.
Introduction
Tobacco use remains the leading preventable cause of disease and death among Latinos, 1 the largest minority group in the United States (U.S.). 2 Of the approximately 60 million Latinos who reside in the U.S., 9.8% are current cigarette smokers. 3 As highlighted in both the National Cancer Institute Tobacco Control Monograph: “A Sociological Approach to Addressing Tobacco-related Health Disparities” and the “Treating Tobacco Use and Dependence Clinical Practice Guideline,” culturally and linguistically appropriate interventions are needed to advance tobacco cessation treatment among Latinos.4,5 Key to this effort is a pressing need to have language-appropriate and validated instruments to support this work – especially as only 25% of U.S. Latinos primarily speak English. 6
Self-efficacy is defined as a personal judgment of “how well one can execute courses of action required to deal with prospective situations.” 7 Self-efficacy is key in the study of behavior change, and has thus been incorporated as a construct in many behavioral theories, such as the Social Cognitive Theory, 8 the Health Belief Model, 9 and the Theory of Planned Behavior. 10 The ability to accurately measure self-efficacy across different populations and behaviors is important for the advancement of health behavior research. Smoking abstinence self-efficacy, or confidence in one’s ability to abstain from smoking, has received much attention in the smoking cessation literature.11,12 Although the scales used to measure self-efficacy, the timing of the measurement (eg, before, during, or after treatment), the abstinence endpoints, and the effect sizes have varied across studies, results from a meta-analysis conducted by Gwaltney et al 11 show that self-efficacy is a consistent predictor of smoking cessation.
The 12-item Smoking Self-Efficacy Questionnaire (SEQ-12) is a valid and reliable instrument to assess confidence in one’s ability to refrain from smoking in a variety of different situations involving both internal (eg, feeling stress) and external stimuli (eg, presence of stimuli associated with cigarettes and other people smoking). 13 First developed in Switzerland, the SEQ-12 has demonstrated test-retest reliability, as well as content reliability and validity when used among a variety of populations and in different languages (eg, the Malay version among Bruneian students, 14 the Thai version among alcohol-dependent smokers, 15 the Chinese version among cardiac patients who smoke, 16 and the English and French version among smokers with a psychiatric comorbidity). 17 To the best of our knowledge, there is no Spanish version of the SEQ-12 and the psychometric properties of the SEQ-12 have not been established among Spanish speakers, precluding the confident use of the instrument in this population. The purpose of this study was to translate the SEQ-12 into Spanish and assess its factor structure and internal consistency among a sample of Latino smokers residing in the U.S.
Methods
Research design
The present study was part of a single-arm pilot study with 50 Latino smokers who received a culturally- and linguistically-adapted smoking cessation text messaging intervention and nicotine replacement therapy (NRT). Details and results of the pilot study have been reported elsewhere. 18 In sum, a culturally- and linguistically-adapted smoking cessation text messaging intervention for Latinos was well-accepted by participants, generated high satisfaction and frequent text messaging interactivity, produced high therapeutic alliance, and resulted in noteworthy cessation rates (30%) at the end of treatment (week 12). 18 Moreover, the authors concluded that the intervention offers a promising strategy to increase the use and adherence of NRT among Latinos. 18 Study procedures were approved and monitored by The University of Kansas Medical Center’s Institutional Review Board.
Participants
Latino smokers were recruited by Promotores de Salud (Spanish for Community Health Workers) using community-based recruitment strategies. Individuals were eligible if they (1) self-identified as Hispanic or Latino, (2) were >21 years of age, (3) smoked a minimum of 3 days in the past week, (4) had a cellphone with unlimited text messaging capability, and (5) were willing to complete a baseline and 12-week follow-up assessment. Individuals were excluded if they (1) were currently enrolled in a smoking cessation program or using smoking cessation medication, (2) had another household member participating in this study, (3) consumed other forms of tobacco (including e-cigarettes), (4) were currently pregnant, breast-feeding, or planning to do so in the next year, or (5) were planning to move from their residential city in the following 6 months. Written informed consent was obtained from each participant. Details and results of the recruitment, eligibility, and consent have been reported elsewhere. 18
Measures
All assessments described in this study were completed in the language of preference of the participant, either English or Spanish, at baseline. The in-person baseline survey collected sociodemographic variables including gender, age, education level, country of birth, language spoken at home, marital status, and type of health insurance. Smoking-related variables collected included number of cigarettes per day (CPD) and responses to the SEQ-12. The SEQ-12 consists of 12 items. 13 Each item is rated on a 5-point Likert scale (1 = not at all sure, 2 = not very sure, 3 = more or less sure, 4 = fairly sure, and 5 = absolutely sure). 13 SEQ-12 scores range from 12 to 60 with higher scores indicating greater self-efficacy. 13
Translation
A forward-backward translation method was used to translate the SEQ-12 into Spanish. 19 In this procedure, a forward translation was produced from the original language (English) to Spanish. Translation was done by 2 research assistants who were fluent in both English and Spanish, and back-translated into English language by a third research assistant, who was also fluent in English and Spanish. Any differences that arose between among the 3 research assistants were discussed until consensus was achieved.
Analysis
For the purpose of this study, only Latino smokers who completed the baseline assessment in Spanish were included in the analysis. Simple frequencies were calculated for categorical variables and means and standard deviations for continuous variables. The Kaiser-Meyer-Olkin measure of sampling adequacy and Bartlett’s Test of Sphericity were analyzed to evaluate whether the data fulfilled the assumptions for carrying out a factor analysis.20,21 An exploratory factor analysis of all items of the SEQ-12 was performed using a principal component method with varimax rotation to identify the underlying factors of the questionnaire. The exploratory factor analysis was chosen because, to the best of our knowledge, this is the first evaluation of the psychometric properties of the Spanish version of the SEQ-12 among Latino smokers. This analysis was largely exploratory, rather than confirmatory, designed to identify items for measuring the construct, rather than the latent structure of the instrument. 22 Moreover, an exploratory factor analysis allows to take into account all of the variance in items, not simply the shared variance, and to identify factors. 22 Factor loadings of 0.30 or higher were considered to be adequate. 22 Cronbach’s alpha was used to assess the internal consistency reliability of the questionnaire. 23 An alpha of .70 or above was set as indicative of adequate reliability.24,25 Item-total correlations were assessed. Item-total correlation values lower than .3 were indicative of items with inadequate correlation with the scale overall. 26
Results
Of the 50 Latino smokers who enrolled into the smoking cessation single-arm pilot study, 47 completed the baseline assessment in Spanish. Table 1 summarizes the baseline characteristics of these Spanish-speaking participants. Participants’ mean age was 43.1 years old (SD 9.4), 66.0% of the participants were male, 42.6% had less than high school graduate education, and most participants (78.7%) had no health insurance. The majority of participants (85.1%) were born in Mexico. Most participants (72.3%) were light smokers (1-10 CPD). Table 2 shows the translation for each item and the distribution of the participants’ scores on the Spanish version of the SEQ-12.
Baseline characteristics of participants (n = 47).

Distribution of scores of the participants on the Spanish version of the SEQ-12 (n = 47).
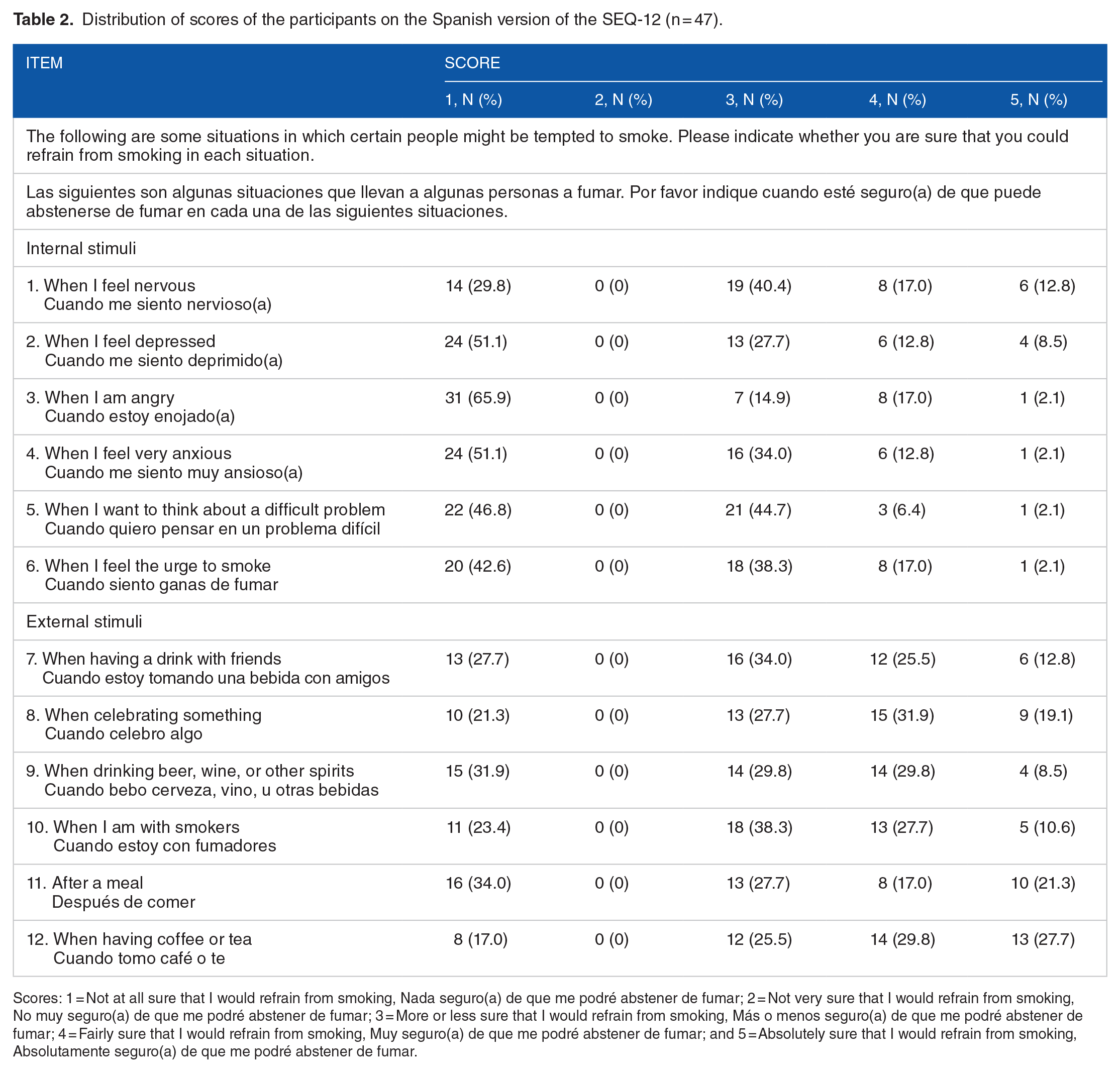
Scores: 1 = Not at all sure that I would refrain from smoking, Nada seguro(a) de que me podré abstener de fumar; 2 = Not very sure that I would refrain from smoking, No muy seguro(a) de que me podré abstener de fumar; 3 = More or less sure that I would refrain from smoking, Más o menos seguro(a) de que me podré abstener de fumar; 4 = Fairly sure that I would refrain from smoking, Muy seguro(a) de que me podré abstener de fumar; and 5 = Absolutely sure that I would refrain from smoking, Absolutamente seguro(a) de que me podré abstener de fumar.
Construct validity
The Kaiser-Meyer-Olkin measure of sampling adequacy was 0.83, confirming factorability of the correlation matrix of the Spanish version of the SEQ-12. The Bartlett’s Test of Sphericity indicated that variables were correlated (χ2 = 270.15, d.f. = 66, P < .001). Using a rule for extracting factors (eigenvalue greater than 1), 4 factors were extracted explaining 45.6%, 11.5%, 8.7%, and 8.3% of variance, respectively, in all 12 variables. The total variance explained by these 4 factors was 74.3%. Item loadings greater than 0.30 on each factor are displayed in Table 3. Items 1, 2, 4, 8, 10, and 11 were loaded on Factor 1, items 3, 5, and 6 were loaded on Factor 2, items 7 and 9 were loaded on Factor 3, and item 12 was loaded on Factor 4.
Exploratory analysis of the Spanish version of the SEQ-12 using principal component extraction with varimax rotation.

Factor loadings below 0.30 are omitted for clear presentation. Factor loadings in bold indicate that the item was considered part of the factor.
Internal consistency reliability
The Cronbach’s alpha coefficient was .76 for the total scale, .87 for the internal stimuli subscale and .67 for the external stimuli subscale. The inter-item correlation matrix is detailed in Table 4.
Item-total correlation and Cronbach’s alpha coefficient for the Spanish version of the SEQ-12.
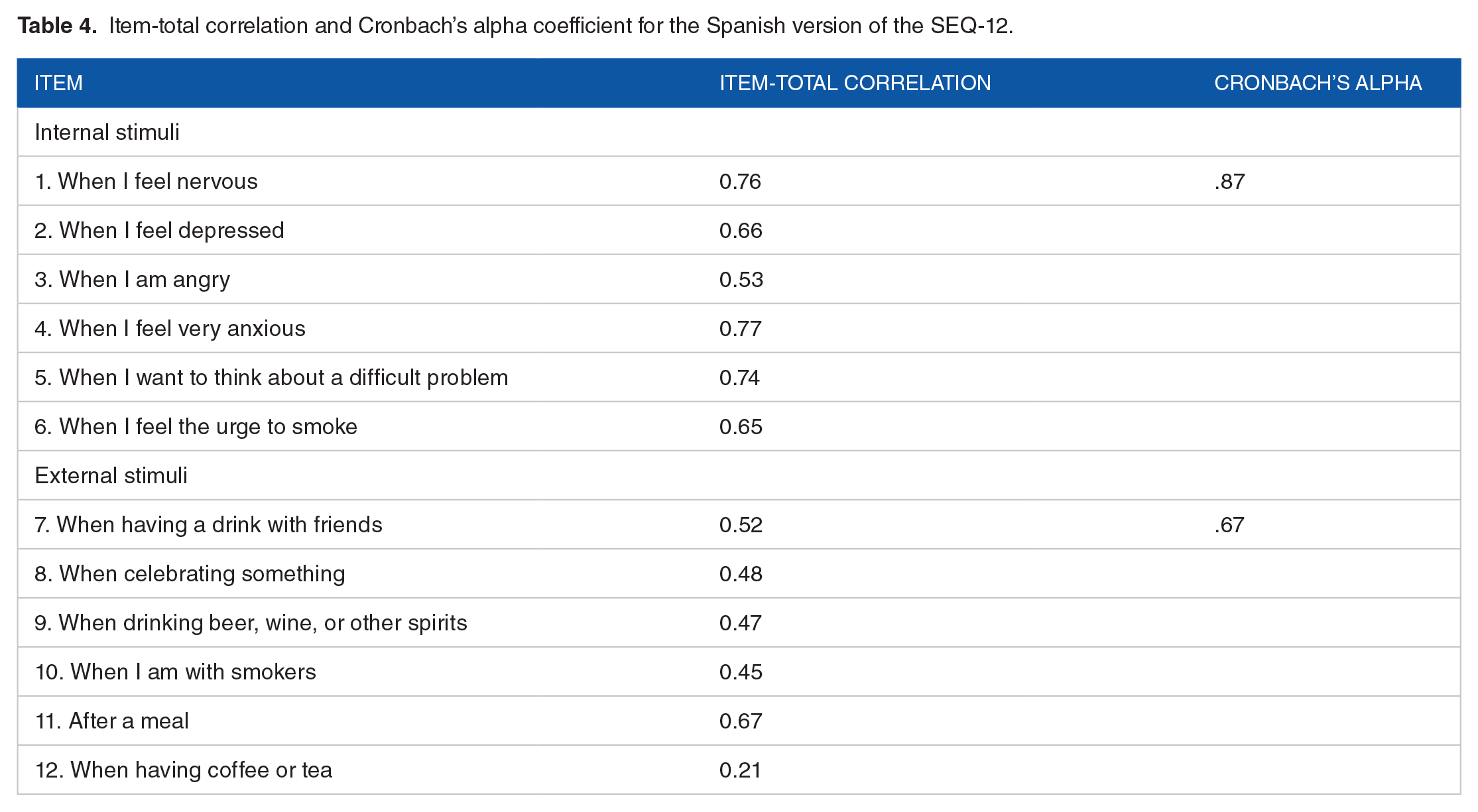
As the item-total correlation value of item 12 (when having coffee or tea) indicated that the item was poorly correlated with scale overall, Cronbach’s alpha coefficients were recalculated after removal of this item. New Cronbach’s alpha coefficients were .78 and .70 for the total scale and the external stimuli subscale, respectively.
Discussion
This study evaluated the psychometric properties of the Spanish version of the Smoking Self-Efficacy Questionnaire among a sample of Spanish-speaking Latino smokers engaged in a smoking cessation research study. A forward-backward translation procedure guided the translation of the SEQ-12 into Spanish. Preliminary psychometric analysis of the new Spanish version provided support for use of the instrument among Latino smokers, using standard indicators of internal consistency and construct validity. This questionnaire could be readily applied to smoking-related studies, especially for interventions aiming to increase participants’ self-efficacy and those examining whether self-efficacy is associated with abstinence among Latino smokers. 27
The Kaiser-Meyer-Olkin value indicated that there was an adequate sample size for the validation of the Spanish version of the SEQ-12. Moreover, the Bartlett’s Test of Sphericity indicated that the questionnaire demonstrated good construct validity. Four factors explained 74.3% of the variance. Factor 1, Psychosocial Factors (items 1, 2, 4, 8, 10, and 11) included both internal and external stimuli (when I feel nervous, when I feel depressed, when I feel very anxious, when celebrating something, when I am with smokers, and after a meal). Factor 2, Negative Mood (items 2, 5, and 6) was related to negative mood (when I am angry, when I want to think about a difficult problem, and when I feel the urge to smoke). Factor 3, Alcohol Consumption (items 7 and 9) was related to alcohol consumption (when having a drink with friends and when drinking beer, wine, or other spirits). Factor 4, Coffee or Tea Consumption, was related to having coffee or tea (item 12). This is an indication that, in the Spanish version of the SEQ-12, self-efficacy was measured in 4 dimensions. This was confirmed by the high factor loadings. All the items had a factor loading after varimax rotation of >0.5.
Similar to this study, Etter et al, 13 performed an exploratory factor analysis of the original SEQ-12 using a principal component method with varimax rotation to identify the underlying factors. Etter et al 13 found that the original SEQ-12 has 2 factors: Internal and external stimuli. Talip et al 14 conducted an exploratory factor analysis of the Malay version of the SEQ-12 using a principal component method with varimax rotation. Consistent with the results from Etter et al, 13 Talip et al 14 found that the Malay version of the SEQ-12 has 2 factors: Internal and external stimuli. In this study, the principal component method with varimax rotation reveled 4 factors in the Spanish version of the SEQ-12: Psychosocial Factors, Negative Mood, Alcohol Consumption, and Coffee or Tea Consumption. One of the factors of the Spanish version of the SEQ-12, Psychosocial Factors, overlaps items of the 2 factors found by Etter et al and Talip et al. This result suggests that, although a meaningful structure of the SEQ-12 can be identified among Latino smokers, factors are likely to vary among populations. Such variations are possibly due to differences in cultural values. More research with larger samples is needed to replicate and consolidate the proposed factors of the Spanish version of the SEQ-12.
This study also revealed that the Spanish version of the SEQ-12 has an acceptable internal consistency for all 12 items (α = .76) and both the internal (α = .87) and external (α = .67) stimuli subscales. These Cronbach’s alphas are lower compared to the original questionnaire (internal stimuli: α = .95; and external stimuli: α = .94). 13 However, these results are comparable to those obtained in the Chinese-translated version of SEQ-12 (internal stimuli: α = .88; and external stimuli: α = .77). 16
Item 12 in the questionnaire (when drinking coffee or tea) had a low item-total correlation value (.21). This phenomenon may be explained by the fact that drinking coffee and tea is not very common among Latinos. According to data from the National Health and Nutrition Examination Survey, both tea consumption and daily coffee drinking are less prevalent among Latinos compared to their white counterparts (tea consumption: 10.3% vs 20.4%, respectively; 28 daily coffee drinking: 42.7% vs 53.9%, respectively). 29 This phenomenon may also be explained by the fact that the majority of participants were light smokers (⩽10 CPD). The relationship of smoking to a morning cup of coffee may not be as strong among light smokers who may wait until later in the day to have their first cigarette. Another possible explanation to this low item-total correlation value may be participant response fatigue, especially since items were not randomized and this item was the last one in the questionnaire. Participant response fatigue occurs when individuals respond to survey questions but do not provide truthful or consistent responses in order to reduce the burden of answering questions. 30 When recalculating the Cronbach’s alpha coefficients after dropping this item from analysis, results indicated that the questionnaire demonstrated somewhat improved reliability.
Limitations
This study has some limitations that should be considered when interpreting the findings. Most participants were of Mexican origin, reflecting Latinos in the U.S. 31 Moreover, although the analysis confirmed the adequacy of the sample size, it was a small convenience sample of smokers interested in smoking cessation. Confirmatory analyses of the psychometric properties of the Spanish version of the SEQ-12 among Latino smokers across all stages of readiness to quit smoking and from different countries of origin are needed. Future studies should investigate whether the Spanish version of the SEQ-12 predicts and/or mediates smoking abstinence. Finally, the psychometric properties of the Spanish version of the SEQ-12 should be further evaluated among non-daily smokers, especially since Latinos are among the racial/ethnic minority groups with the highest rates of non-daily smoking. 32 In addition, evidence suggests that individuals who smoke more cigarettes have low self-efficacy scores and are less confident in their ability to stop smoking than those who smoke less.33,34
Conclusion
The Spanish version of the SEQ-12 shows promising internal consistency reliability and construct validity among Latino smokers, with potential applications in both research and clinical settings. The use of reliable, validated, Spanish-language assessments tools is vital to supporting crucial research, in light of the need for culturally and linguistically appropriate interventions to advance tobacco cessation treatment among Latinos. Future research should examine other aspects of instrument validity (eg, predictive validity) and involve larger and more heterogeneous samples, to rule out the effect of sample homogeneity on the results.
Footnotes
Acknowledgements
The study was based at JUNTOS Center for Advancing Latino Health, an academic and community partnership at the University of Kansas Medical Center. We are grateful to the individuals who participated in this study. Special acknowledgment to members of our Community Advisory Board as well as the JUNTOS research team (listed in alphabetical order by last name): Drew Cox; Kendra Cruz, MPH; Lucia Martínez; Norma Molina; Jaime Perales-Puchalt, PhD; Mariana Ramírez, LMSW; Mitzi Ramirez; Catalina Reyes; and Karen Yepez-Maza.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Minority Health and Health Disparities (NIMHD) under grant R41MD010318. The content is the sole responsibility of the authors and does not necessarily represent the official views of the NIMHD.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.