
Abstract
Background
Supporting smoking cessation at pharmacies can be challenging owing to difficulties in recruiting smokers to participate in cessation programs, insufficient communication skills among pharmacists, and lack of knowledge and self-efficacy in successfully quitting smoking in Japan.
Objective
This study evaluates the effectiveness of a smoking cessation training program on community pharmacists’ knowledge, attitude, and self-efficacy in supporting smoking cessation.
Methods
The study, conducted in Japanese pharmacies with 100 community pharmacists, employed a quasi-experimental design. Two online training programs were implemented. Participants completed a web-based survey assessing their knowledge, attitude, and self-efficacy in supporting smoking cessation before, immediately after, and 1 year after the training program. A two-way analysis of variance with a mixed model was used to examine score changes at each time point.
Results
Total knowledge scores significantly increased between baseline and immediately after training and baseline and 1 year after training. The total attitude scores between baseline and immediately after training differed significantly. However, no differences were noted between baseline and 1 year after training. Total self-efficacy scores significantly increased at baseline, immediately after training, and between baseline and 1 year after training. Despite no significant interactions between the programs, there was a partial interaction effect on knowledge, with only the customized program having items whose knowledge levels improved after 1 year.
Conclusion and Relevance
The training program improved community pharmacists’ knowledge, attitude, and self-efficacy regarding smoking cessation support. The customized program must be reinforced to improve support performance and maintain attitude.
Introduction
Smoking is a risk factor for cancer, cardiovascular diseases (including stroke), respiratory diseases (such as chronic obstructive pulmonary disease), type 2 diabetes, and dementia. In Japan, according to data released by the Ministry of Health, Labour and Welfare in FY2016, active smoking is estimated to cause 120,000-130,000 deaths yearly. These account for approximately 10% of all deaths annually, with most deaths attributed to cancer (77,000), followed by cardiovascular (33,000) and respiratory diseases (18,000). 1
Historically, smoking cessation support in Japan has been delivered primarily through smoking cessation outpatient clinics staffed by doctors and public health nurses who provided specific health guidance. 2 However, ensuring adequate smoking cessation support systems is becoming increasingly challenging. The Ministry of Health, Labour and Welfare in Japan launched the “family pharmacy system” in 2016, which requires community pharmacies to be more deeply involved in the health management of patients as “health support pharmacies.” In this system, support for smoking cessation is explicitly stated as the pharmacists’ role. 3 Considering these circumstances, if pharmacists were to take a more active role in providing smoking cessation support in pharmacies, they could significantly contribute to the “improvement of public health”—a key responsibility for pharmacists. Although several intervention studies have examined and reported the effect of pharmacists in supporting smoking cessation,4-6 their evaluation remains to be determined. 7 Moreover, despite efforts to promote smoking cessation support in pharmacies in Japan, its uptake remains limited.8-10 Additionally, there is a lack of intervention research in the field.11-13
Supporting smoking cessation at pharmacies can be challenging owing to various factors, including difficulties in recruiting smokers to participate in cessation programs, insufficient communication skills among pharmacists, and a lack of pharmacists’ self-efficacy to support smoking cessation successfully. 14 Nevertheless, training programs designed to enhance pharmacists’ knowledge, attitude, and self-efficacy related to smoking cessation support can improve their ability to interact with smokers effectively. 15
Several previous studies have investigated the effect of training on smoking cessation support, with a systematic review published in 2022 encompassing 12 studies that evaluated the effects of diverse educational interventions aimed at enhancing community pharmacists’ abilities to provide smoking cessation services. 15 One study, which involved a 1-day workshop that featured 3 hours of lectures and 3 hours of role-playing exercises, revealed that all participating pharmacists exhibited improved knowledge, role attitude, and self-efficacy regarding smoking cessation counseling practices. 16 Another investigation incorporated two types of training, with the intervention group receiving six hours of instruction based on the stage-of-change model and motivational interviewing, resulting in an improved smoking cessation rate compared with a control group that received 3 hours of training. 17 Moreover, the follow-up education training program, which comprised home studies and live training, and incorporated the 5 As (Ask, Advise, Assess, Assist, and Arrange) approach, has been shown to improve post-course knowledge and self-efficacy in smoking cessation counseling. 18
Several studies have shown that providing training to pharmacists in smoking cessation clinics leads to improved patient attitude (evaluated using the number of patients approached by pharmacists for consultations) and the distribution of more handouts. 19 Furthermore, smoking cessation support programs that emphasize the strategic use of handouts and refinement of their consultation style using appropriate body language and key phrases have resulted in better outcomes for smokers seeking cessation support. 20
Previous studies confirm the effect of educational interventions on three key aspects: improvement in pharmacists’ self-efficacy, knowledge, and attitude toward providing smoking cessation services. However, training programs for community pharmacists to support smoking cessation in Japan focus on imparting knowledge. Moreover, there are no systematic or practical training programs, and the verification of educational effectiveness is insufficient.
Objective
Given the aforementioned situation, this study aims to develop two types of “pragmatic smoking cessation support training programs” for community pharmacists and determine their effectiveness. Specifically, this study aims to demonstrate the positive effects of these training programs on the improvement and sustainability of community pharmacists’ knowledge, attitude, and self-efficacy regarding smoking cessation support
Method
Design and Setting
This is a quasi-experimental study conducted in January 2022, encompassing pharmacies located in the Western region of Japan.
Participants
Out of the chain pharmacies that consented to participate in the study, 100 pharmacists working in 84 pharmacies, which had been notified as health support pharmacies, were included. The managing pharmacist at each pharmacy recruited staff pharmacists to participate in the training program, and at least one pharmacist at each pharmacy agreed to participate. The time required to confirm participants was one and a half months. Pharmacists were randomly assigned in a 1:1 ratio to attend different training programs (50 pharmacists in each program). This study utilized the sample-size calculation formula outlined by Viechtbauer et al, 21 with parameters set at a 95% confidence level and a margin of error of ± 4%. A sample of 59 pharmacists was required for this study.
Written consent was not required for this research study, as each participant’s voluntary response to the questionnaire was considered consent.
22
However, the following text was inserted at the beginning of the online response screen. • Participation in the survey is voluntary and you may refuse to answer. • By responding to the survey, you agree to cooperate with the survey. • You will not receive any special treatment because you responded to the survey. • Those who do not respond to the survey will be excluded from the study.
Intervention
Two categories of 1-day training programs, the standard and customized versions, were meticulously devised and implemented via the digital platform Zoom. Before participating in the training sessions, individuals completed an electronic learning module referred to as a J-stop, which was imparted by the Japan Smoking Cessation Promotion Physicians and the Dental Federation, to acquire fundamental knowledge how to provide brief motivational counseling and general information about smoking cessation. 23
J-stop consists of 3 sessions (video lecture, text learning, and case series). The learning time is about 3 to 4 hours. Video lectures include information about approaches for achieving smoking cessation in clinical practice. The text learning includes 4 parts (harmful influence of smoking, effects of smoking cessation, nicotine dependence, and pharmacotherapy for smoking cessation). The case series includes three cases: case 1 is a male in the precontemplation stage of change for smoking cessation; case 2 is a male in the contemplation stage of change for smoking cessation; and case 3 is a female in the contemplation stage of change for smoking cessation. The 20 sample questions and answers include frequent contemplation, and preparation of change for smoking cessation stages.
After completing the e-learning program, the participants were randomly assigned to one of the training programs. If the individuals could not attend live online training, they were allowed to access an on-demand video recording of the training.
In their daily work, Japanese community pharmacists “instruct” patients, focusing exclusively on prescription drugs, and are not accustomed to offering “support” that empowers patients while attending to their feelings. Therefore, they lack the knowledge, attitude, and self-efficacy to support smoking cessation. Thus, while constructing the training program, we aimed to follow a simple approach that can be implemented in daily practice for 5-15 min using the 5 As 24 (Ask, Advise, Assess, Assist, Arrange) and 5 Rs 24 (Relevance, Risk, Rewards, Repetition, Roadblock) methods, which have been proven successful in helping people quit smoking worldwide. The training program was constructed following the Delphi method with physicians practicing smoking cessation counseling, health promotion specialists with experience conducting smoking cessation classes in the community, and academic and educational personnel from pharmacies and university faculty members conducting the practical experience. Subsequently, a workshop was held by physicians in charge of smoking cessation, community pharmacists, university faculty (pharmacists), and researchers to develop the program and compile it into a manual.
Training programs (standard version and customized version).

Content differs from the standard version in areas marked with ✓.
On January 31, 2022, a customized version of the training program that included recruitment training similar to the standard version was conducted. The customized version covered various topics, such as continuous follow-up procedures in accordance with the original smoking cessation guidebook, usage of handouts and smoking cessation aids, setting up pharmacy bulletin boards and attitude-raising corners, and case-specific counseling using the 5As, 5Rs, 24 and behavior change stage models in the form of discussions. Compared with the standard version, the customized version introduces the smoking cessation support program (FINE), which the authors have implemented and confirmed to be effective, 11 and provides a more specific flow of smoking cessation follow-up. This helps to understand the readiness of smoking patients and improve customized support for smoking cessation (Table 1).
Effectiveness assessment
In this study, “attitude” refers to the extent to which pharmacists recognize the need, understand the significance, and are motivated to offer smoking cessation support in the pharmacy. Additionally, “self-efficacy” refers to the pharmacist’s level of confidence in encouraging and empowering smoking patients to quit smoking and supporting them in achieving smoking cessation.
Before attending training, we conducted a baseline web survey that covered the following: pharmacists’ attributes (years of service, experience with smoking cessation support, and experience with successful smoking cessation support); knowledge of smoking cessation support comprising 13 items; attitude toward smoking cessation support comprising 10 items; self-efficacy in smoking cessation support comprising 12 items. Furthermore, following the training, we conducted an additional web survey on knowledge, attitude, and self-efficacy in smoking cessation support and compared the changes before (baseline), immediately after, and 1 year after the training program. Regarding knowledge, respondents could choose between correct, wrong, and do not know. For each question related to “attitude toward smoking cessation support,” the consciousness scale ranged from 0 (completely disagree) to 10 (completely agree). The respondents were asked to rate their self-efficacy levels for smoking cessation support on a scale of 0 (not confident at all) to 10 (very confident) for each question. These questions were newly designed by the authors to test this study’s effectiveness. Tables 3–6 present all the questions.
Analytical methods
Based on the responses from the pharmacists in the baseline survey, we computed Cronbach’s alpha coefficient to verify the consistency and reliability of the questions evaluating knowledge, attitude, and self-efficacy. Data from pharmacists who responded to all surveys at the time points prior to attending training (baseline), immediately after the study, and 1 year after training were used in the analysis. We aggregated the scores for knowledge (13 points for one correct answer to 13 items), attitude (total: 100 points), and self-efficacy (total: 120 points) into a single total score for each of these timings. A two-way analysis of variance with a mixed model was conducted using IBM SPSS Statistics for Windows version 28.0 to investigate the changes in pharmacists’ knowledge, attitude, and self-efficacy in smoking cessation support before (baseline), immediately after, and 1 year after the training program. By testing for the presence of an interaction effect, we checked for differences in the trend of score change over time among the programs. If there was no interaction, Bonferroni multiple comparisons were used to compare scores across timings. If an interaction was found between programs, a one-way analysis of variance was performed for each program. A level of 5% was considered statistically significant.
Main outcome measures
The main outcome measures were as follows: changes in pharmacists’ knowledge, attitude, and self-efficacy in smoking cessation support before (baseline), immediately after, and 1 year after the training program, respectively.
Ethical compliance
This study was conducted with the approval of the Ethics Committee of Osaka Medical and Pharmaceutical University (Approval number: 0054).
Results
Pharmacist attributes at baseline
Pharmacist attributes at baseline.

A t-test was used to compare years of service, and a chi-squared test was used for the other items.
Reliability of questions
Cronbach’s alpha coefficient, a measure of reliability, was 0.690 for knowledge, 0.946 for attitude, and 0.852 for self-efficacy at baseline. Although there is no absolute standard for Cronbach’s alpha coefficient, it is generally considered that the internal consistency would not be a problem if it was approximately 0.7 or higher.
Changes in knowledge, attitude, and self-efficacy before (baseline), immediately after, and 1 year after the training program
The number of pharmacists for whom response data were available at all times (baseline, immediately after training, and 1 year later) was 36 in the standard version group and 43 in the customized version group. The retention rate was 79%, as 14 pharmacists occurred in the standard version and 7 in the customized version who were not available for follow-up due to leave of absence or resignation during the study period.
Change in knowledge
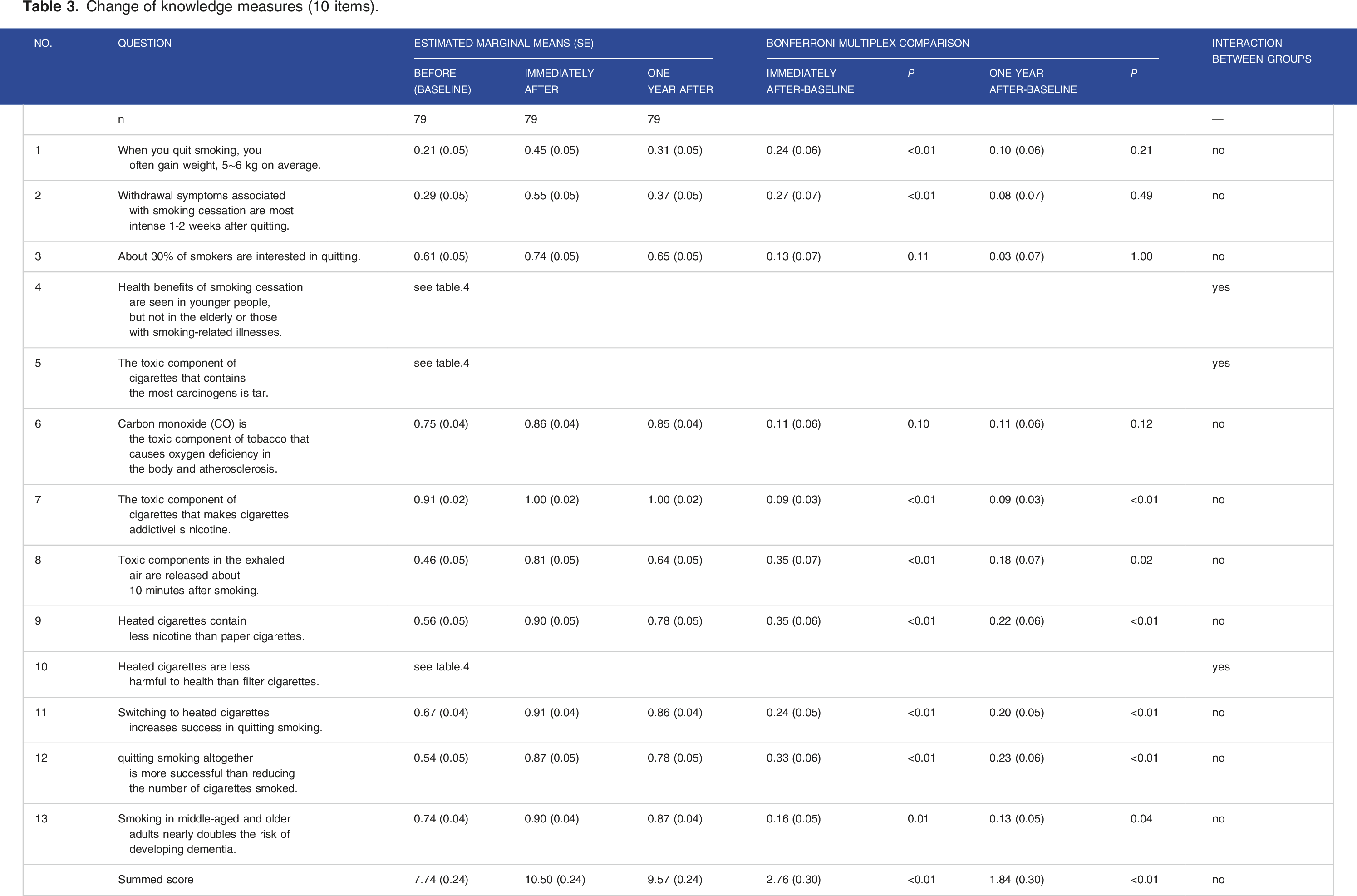
Change of knowledge measures (10 items).
Change of knowledge measures (3 items).

Items that showed varying degrees of knowledge were compared. For questions 7 (nicotine toxicity), 8 (time of release of harmful components from breath), 9 (heated tobacco and nicotine), 11 (change to heated tobacco and ease of quitting smoking), 12 (ease of quitting smoking through smoking moderation), and 13 (smoking and dementia risk), differences from baseline (hereafter referred to as “differences”) at both timings were noted. Additionally, differences were found immediately after training for questions 1 (weight gain owing to smoking cessation) and 2 (timing of onset of withdrawal symptoms).
Regarding the three items for which there was an interaction between programs, only the customized version showed a difference at both time points for Question 4 (age and smoking cessation effect). Regarding Question 5 (tar as a toxic component), the difference was observed 1 year after the customized version. Regarding Question 10 (harmfulness of heated cigarettes), there was a difference at both time points for the standard version and immediately after the customized version.
Change in attitude
Change of attitude measures (10 items).

In the item-by-item analysis, differences were observed immediately after the training rather than after 1 year for the following questions: 3 (importance of support for smoking cessation by pharmacists); 4 (importance of pharmacists receiving training in support of smoking cessation); 9 (importance of using posters and other materials to raise smoking patients’ awareness of smoking cessation in pharmacies); and 10 (importance of setting up smoking cessation support corners in pharmacies). Furthermore, a negative difference was found for Question 7 after 1 year (effectiveness of providing smoking cessation support according to the readiness of smokers).
Change in self-efficacy
Change of self-efficacy measures (12 items).

In the item-by-item analysis, all items except question 12 (support for smoking cessation for smokers in the preparation stage) showed differences immediately after training. Furthermore, differences were observed 1 year after training for the following questions: 1 (recruitment); 2 (explaining and dealing with withdrawal symptoms); 3 (support for varenicline users); 4 (support for nicotine patch users); 5 (support for nicotine gum users); 6 (referral to smoking cessation clinics); and 7 (support for the elderly to quit smoking).
Discussion
This study examines the effectiveness of two smoking-cessation support training programs developed for community pharmacists. In the analysis by summed score in the knowledge, attitude, and self-efficacy, there was no interaction between the two training programs, suggesting that they were effective. This study is quasi-experimental and will contribute to the development of a smoking cessation support program to further improve pharmacists’ knowledge, attitude, and self-efficacy. Specifically, the home study (e-learning) component included learning about the harmful effects of tobacco (including heated tobacco), the trans-theoretical model, and the 5As smoking cessation counseling process, which commonly included recruitment, smoking cessation education activities in community pharmacies, and problem solving through case studies. However, while the standard version is relatively didactic in the content review of the home study and preparedness and attitude toward smoking cessation support, the customized version includes specific individualized measures, such as ongoing follow-up according to the original smoking cessation guidebook and case-specific 5As and 5Rs counseling. Therefore, our initial hypothesis stated that the effects on knowledge, attitude, and self-efficacy would differ (ie, an interaction would be observed) between programs; nonetheless, no interaction was found, except for a few knowledge items. This is attributed to the fact that the customized version did not allow for sufficient practice of instructional techniques that have been shown to improve self-efficacy, such as group discussions, role-play, and feedback, especially in recruitment and case studies, because the training was entirely online.
For summed knowledge scores, there was a significant improvement compared with the baseline at both times. Regarding the items for which there was an interaction, improvement was observed in one of the three items for the standard version and three items for the customized version. We believe that this may be the result of a home study contributing to the development of skills, the foundation of knowledge necessary for higher-order thinking, and the subsequent training program contributing to greater awareness of the resources necessary to apply knowledge to practice. 25
Regarding the summed score of attitude, there was an improvement immediately after training. However, there was no significant difference between baseline and 1 year after training. Although four of the ten items showed improvement immediately after training, and one item showed improvement 1 year after training, pharmacists’ attitude were relatively low. A previous study reported that a 1-day workshop focusing on role-playing improved the attitude of all participating pharmacists toward smoking cessation counseling. 16 Another study also has demonstrated the long-term benefit of the stage of change training over a 3-year period, for both community pharmacists and their staff, on attitudes. 25
Therefore, the lack of sufficient role-playing in the current training programs may have been the main reason for the low degree of attitude improvement.
Regarding the summed self-efficacy score, there was a significant improvement compared with the baseline at both time points. Eleven of the 12 items showed significant improvement over baseline immediately after training, and seven items showed significant improvement 1 year after training. This is consistent with previous research showing that live training incorporating home study and the 5As approach improved self-efficacy after the course. 18 This finding also suggests that even online, pharmacists’ self-efficacy can be enhanced by integrating instructional training strategies such as group discussions and feedback.
While working in this field, pharmacists seek opportunities to hone their skills and improve patient care. Therefore, those who construct and implement training programs should aim to improve pharmacists’ knowledge, attitude, and self-efficacy simultaneously. In a previous study, more than 75% of pharmacists could provide smoking cessation counseling, and 65% could perform 5As brief interventions after participating in a smoking cessation support workshop that incorporated role-playing. Nevertheless, the latter reported that they lacked the skills to assist with smoking cessation plans and follow-up arrangements. 26 Thus, further improvement of the customized version developed in this study is likely to influence pharmacists’ skill development and their ability to translate these skills into practice. Future work is necessary to verify whether pharmacists who participate in training programs actually offer smoking cessation support in the field.
Limitations of this Study and Future Issues
We recognize several limitations in this study. First, we developed our own scales for knowledge, attitude, and self-efficacy in order to evaluate the effectiveness of this training program according to its content. Cronbach’s alpha coefficient, a measure of reliability, was 0.690 for knowledge, 0.946 for attitude, and 0.852 for self-efficacy at baseline. There is no absolute standard for Cronbach’s alpha coefficient, but it is generally considered that internal consistency is not a problem when it is above approximately 0.7. In the present study’s results, the Cronbach’s alpha coefficient for knowledge was below 0.7, indicating that there is room for improvement and that a more validated questionnaire needs to be developed. In the future, a factor analysis should be conducted using the established scale to carefully check for factors that measure different aspects of knowledge. Second, owing to the limited sample size, caution should be exercised when generalizing the results. Third, as both programs were conducted online to prevent the spread of infection with COVID-19, group discussions, role plays, and accompanying performance evaluations could not be conducted adequately. We believe that this may explain why the customized versions, which emphasize individualized responses, and standard version were not differentiated. In the training we had conducted before, we had role-playing every time, but we could not do it this time. Therefore, in the future, it is necessary to try role-playing at least once, with oneself in the role of a supporter. Forth, the study did not investigate attributes such as gender, age or work experience of the pharmacists who responded. The main reason is that several surveys conducted by the authors did not suggest an association between pharmacist attributes and knowledge, attitudes and confidence in support for smoking cessation, and that there is no previous research suggesting an association between pharmacist attributes and knowledge, attitudes and confidence in support for smoking cessation. Nonetheless, despite some limitations, this is the first study in Japan to examine the effectiveness of smoking cessation support training over a long period. We believe that we have gained valuable insights.
Conclusion
The smoking cessation training program had a positive impact on community pharmacists’ knowledge, attitudes, and self-efficacy in supporting smoking cessation. The customized program showed effectiveness in improving knowledge levels after 1 year, suggesting the need for reinforcement to enhance support performance and maintain positive attitudes. In the future, integration of training strategies can enhance participants' smoking cessation support skills conducting the training program in a face-to-face format to include interactive components that were not possible in the online format.
Supplemental Material
Supplemental Material - Effect of a Smoking Cessation Education Program on the Knowledge, Attitude, and Self-Efficacy of Community Pharmacists in Japan: A Quasi-Experimental Study
Supplemental Material for Effect of a Smoking Cessation Education Program on the Knowledge, Attitude, and Self-Efficacy of Community Pharmacists in Japan: A Quasi-Experimental Study by M. Onda, M. Horiguchi, M. Domichi and N. Sakane in Tobacco Use Insights
Footnotes
Acknowledgements
Authors Contributors
Onda, M, Contributed to conception and design, Contributed to analysis, Drafted the manuscript, critically revised the manuscript, Gave final approval, Agrees to be accountable for all aspects of work ensuring integrity and accuracy. Horiguchi, M, Contributed to conception and design, critically revised the manuscript, Gave final approval, Agrees to be accountable for all aspects of work ensuring integrity and accuracy. Domichi, M, Contributed to conception and design, critically revised the manuscript, Gave final approval, Agrees to be accountable for all aspects of work ensuring integrity and accuracy. Sakane, N, Contributed to conception and design, Contributed to analysis, critically revised the manuscript, Gave final approval, Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.