
Abstract
Background:
The prevalence of smoking has increased in recent years in Saudi Arabia. Our objectives were to determine the factors affecting smoking among physicians and to assess physicians’ quitting behavior.
Methods:
A cross-sectional study was carried out at 3 district hospitals in Riyadh, Saudi Arabia. It involved physicians with different levels of experience and different specialties. They were asked to complete a self-administered questionnaire adapted from validated tools. The questionnaire addressed sociodemographic data, lifestyle, and work-related factors as well as smoking cessation and relapse. SPSS statistical software was used for the statistical analysis.
Results:
The study included 290 physicians, of whom 91% were Saudi and 59.7% were male. About 55.2% were younger than age of 30. Overall, 34.8% were smokers. The following factors had a significant association with smoking: a smoking family member/friend, resident occupational status, medical specialty, and frequent on-call duties increased the likelihood of smoking. One-third of the physicians (31.6%) who tried to quit smoking reported seeking information on social media, television, and/or the internet. The most common causes of relapse were social stress and withdrawal symptoms, while the least common was work-related stress.
Conclusions:
Smoking was highly prevalent among physicians. The likelihood of smoking was higher in, residents, medical specialists and those with a high number of on-call duties. Moreover, this study described cessation practices in this group, which might be considered when designing and improving counseling programs for physicians who smoke.
Introduction
Physicians have major responsibilities for tobacco control, and their attitudes and practices regarding smoking can affect their own health, if they are smokers, and that of their patients. 1 During the past 2 decades, overall global tobacco use has decreased from 1.397 billion in 2000 to 1.337 billion in 2018, according to the WHO global report on trends in the prevalence of tobacco use 2000 to 2025. 2 However, despite this reduction in prevalence, it has been reported that approximately 8 million deaths annually occur due to smoking-related illnesses. 3
There are no recent data on smoking behavior among healthcare professionals or physicians in particular. Most of the studies performed in the period from 2000 to 2010 reported that smoking is prevalent among healthcare staff. 4 The highest reported prevalence of smoking among physicians were 37% in Central/Eastern Europe, 29% in Africa, 25% in Central and South America, and 17.5% in Asia. Meanwhile, the lowest rates are reported in developed countries such as the USA, UK, and Australia. 5 In Saudi Arabia, a review article published in 2009 reported that 16% to 34% of physicians and pharmacists were current smokers. 6
Different sociodemographic and lifestyle factors might influence smoking behavior. One study of medical students showed that the most common influencing factors were peer pressure, parents’ smoking, and the media. 7 Moreover, age plays a role, as smokers tend to initiate smoking at a younger age and then continue to smoke until adulthood. 8 Individuals’ work and workplace might have an impact on smoking. 9 For example, shift work was shown to be associated with a higher smoking prevalence than non-shift work. 10 Among physicians, it has been found that anesthesiology and surgical residents were more likely to smoke than those at other occupational levels or in other specialties. 11
Smoking cessation counseling is an important service provided by physicians. However, some studies have reported that the smoking status of physicians can affect their role in offering such services; that is, nonsmokers tend to engage in a significantly higher frequency of patient counseling than current smokers do.12,13 Moreover, few published studies have discussed this complex issue and examined whether common cessation methods that might work with the general population can be generalized to physicians.14,15
Several local studies have confirmed that smoking is a firmly established epidemic. However, few have investigated the prevalence of smoking among healthcare professionals, particularly physicians.16,17 Few studies have explored the factors affecting smoking behavior or the causes of cessation and relapse. Taking all these issues into consideration, we aimed to explore smoking behavior among physicians in Riyadh, Saudi Arabia, and to assess factors associated with smoking, cessation attempts and relapse.
Methods
This was a cross-sectional study that was carried out at 3 district hospitals in Riyadh, over a 6-month period in 2017 to 2018. The sample included physicians living in Riyadh and comprised a range of specialists as well as medical interns. Data were collected using a self-administered questionnaire that was adapted from the Global Health Professions Student Survey (GHPSS). 18 The variables included sociodemographic data, lifestyle, work-related factors, smoking cessation, and relapse.
Using convenience sampling, we calculated the sample size using a statistical software program based on the following parameters: a population size (N) of approximately 70 000 physicians in Riyadh; a hypothesized prevalence of smoking in the population (p) of 50% ± 5; and a 90% confidence interval with 80% power.
We pretested our instrument on 20 individuals to determine the face validity and the time required to complete the questionnaire. We mainly used online questionnaires, which made missing responses unlikely by making answers fields mandatory. SPSS statistical software (release 24, SPSS, Inc., Chicago, USA) was used for data analysis. Data are presented as the means and standard deviations (SDs) for continuous data and as frequencies and proportions for categorical data. The chi-squared test was used to assess associations between categorical variables, while ANOVA was used to compare the means of continuous variables. Binary logistic regression was conducted to verify the variables that were associated with smoking status (smoker, nonsmoker). A P ⩽ .05 was considered statistically significant.
The study protocol was approved by the Institutional Review Board (IRB) at Princess Nourah Bint Abdelrahman University, Riyadh, Saudi Arabia (IRB-PNU: 11061601). Written informed consent was obtained from the participants.
Results
A total of 293 participants returned completed surveys. However, 3 participants were excluded because they were not physicians. About 91% of the subjects were Saudi citizens, 59.7% were males, and 55.2% were younger than age of 30; the participants’ ages ranged from 24 to over 45 years. Their occupations were as follows: 39.6% residents, 22.7% interns, 22.4% consultants, and 15.2% registrars (Table 1).
Sociodemographic characteristics of the study sample (n = 290).
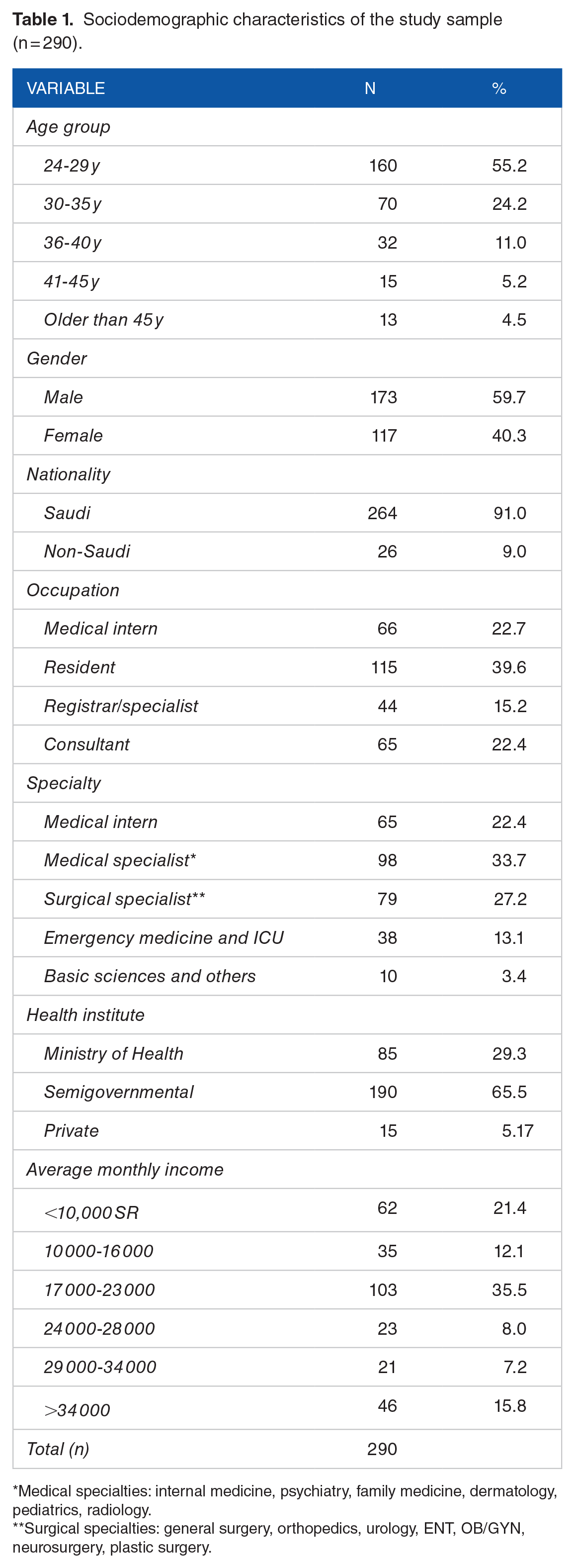
Medical specialties: internal medicine, psychiatry, family medicine, dermatology, pediatrics, radiology.
Surgical specialties: general surgery, orthopedics, urology, ENT, OB/GYN, neurosurgery, plastic surgery.
A 34.8% of the participants were smokers; of these, 22.75% smoked tobacco and 20% smoked waterpipes (shisha) (Table 2). The smoking prevalence was 70.4% for males and 29.6% for females. Smoking was most prevalent among residents (50%), followed by medical interns (22.4%) and registrars (15.3%), as shown in Figure 1. Moreover, smoking was more prevalent among medical specialists than among other specialists (Figure 2). Further exploration on smoking behavior among this sample revealed that (45.5%) started smoking at age between 21 and 25-year-old and (41.5%) smoked for at least 1 to 5 years. Moreover, (44.5%) attribute smoking behavior to experience something new followed by stress (37.6%). Regarding impact of work on smoking behavior, it has been found that (41.6%) think that work increases their smoking, while (37.6%) think it has no effect. Furthermore, long working hours and workload were the leading factors for smoking (34.6% and 15.8%) respectively.
Prevalence of smoking (n = 290).

Ex-smoker: smoking cessation for more than a year.

Prevalence of smoking according to physician’s occupation.

Prevalence of smoking according to physician’s specialty.
Considering smoking as dependent binominal variable (smoker, non-smoker) and the following variables are independent (marital status, nationality, income, occupation, number of on calls, working hours, institute, presence of smoker among family/friends, exercise, coffee consumption, and sleeping duration), we have conducted binary logistic regression to determine which of these factors associated with smoking as shown in Table 3. After adjusting for age and gender, this model showed that smoking associated with presence of smoking member in the family and friends, resident occupation, and number of on-calls. Moreover, the chi-squared test indicated that there was a statistically significant difference between the participants with medical and surgical specialties (χ2 = 11.5, P = .021). Therefore, there was a statistically significant association between smoking and the participants’ specialties.
Multivariate logistic regression model of factors associated with smoking (adjusted for age and gender).
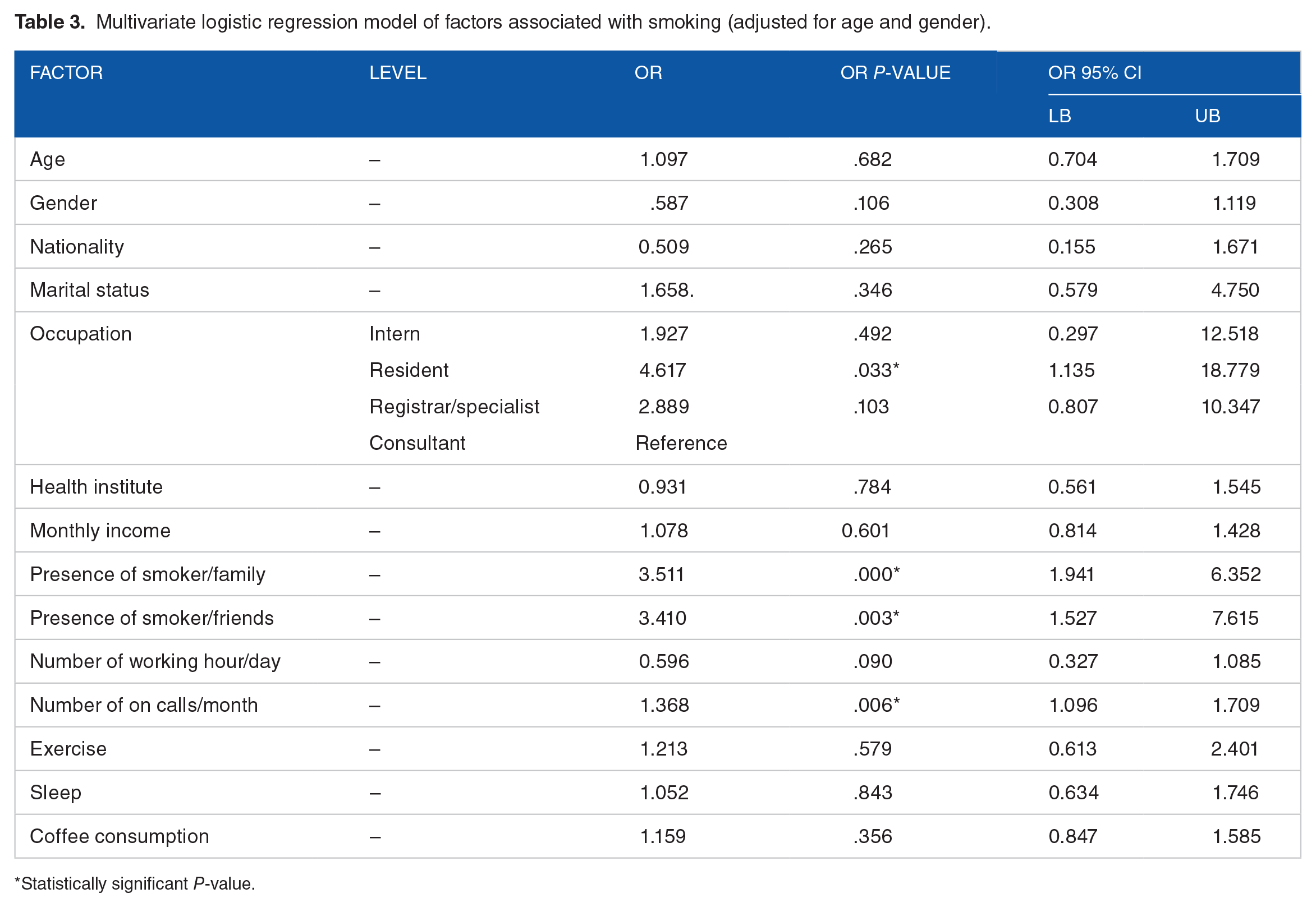
Statistically significant P-value.
Regarding smoking cessation, 34.7% of the participants had an intention to quit smoking. Moreover, 66.3% of the current smokers had attempted to quit smoking in the past. A total of 40.8% of the smokers had quit smoking for less than 1 month, 24.5% had stopped smoking for 1 to 5 years, and only 1% of the smokers had stopped smoking for 3 years or longer in the past.
The most important factors that influenced smoking cessation were health risks, passive smoking hazards, and health provider counseling (21.4%, 19.4%, and 12.2%, respectively). Other factors that contributed less were religious reasons, parent/spouse disapproval, advice from family/friends, and the effect of smoking on appearance (dark lips, gums, etc.; 7.1%, 6.1%, 4.1%, and 4.1%, respectively).
Regarding methods for smoking cessation, 31.6% sought information from the internet, television, and social media; the next most commonly endorsed method was obtaining healthcare advice (8.2%), followed by self-help pamphlets (5.1%). Finally, regarding the reasons for smoking relapse, 24.5% of the participants cited social stressors, and 21.4% cited withdrawal symptoms. Work-related stress was reported as a cause of relapse in only 9.2% of smokers.
Discussion
Based on the recent WHO report on global trends in tobacco use, the smoking prevalence in Saudi Arabia was estimated to be 19.4% in 2020. 2 This study reported a high prevalence of smoking among physicians compared to reports from other countries, such as Japan. 19 Moreover, a study of Estonian physicians showed a lower prevalence of smoking among physicians than among the general population. 20 In our study, the prevalence of smoking a waterpipe was 20%, while in a recent local study, the prevalence was 45% among physicians. 21 Interestingly, both studies showed that the prevalence of smoking a waterpipe (shisha) was higher among physicians than among the general population. 22
Smoking was more common in the younger age group, and one study reported a similar finding in which people usually started smoking in early adulthood and continued afterward. 23 Previous studies indicated that smoking was more prevalent among males during their college years. 7 The smokers thought that smoking helped them face stress, 24 while others reported that imitating peers and boredom encouraged them to smoke. 25
We explored the possible sociodemographic factors associated with smoking, such as having family members/friends who smoke, that were consistent with previous studies.11,26 The highest smoking rate was among residents, a finding that might be explained by the fact that residents, followed by interns and consultants, comprised the highest proportion of participants. A comparable outcome was also reported in another study carried out in Saudi Arabia. 27 Moreover, the present study showed an association between smoking and the physicians’ specialty, in contrast to a previous study, which showed a higher prevalence of smoking among surgical specialists. 21 We speculate that a future study with a larger sample size and equal representation of different ranks and specialties will identify any potential association between smoking and work-related variables.
Healthcare professionals usually face challenging and demanding situations as well as considerably stressful shifts/on-call duties. Thus, some workers tend to smoke to overcome work-related stress. 23 This might explain why on-call shifts were associated with smoking among physicians. However, other work-related factors, such as workplace setting and number of working hours, showed no significant association with smoking.
Previous smoking cessation for one month was reported by approximately 40% of the smokers, and previous smoking cessation for 1 to 5 months was reported by 24% of the smokers. The most common reasons for quitting were health concerns and the effect of passive smoking on their families. Multiple studies have indicated that physicians’ desire to quit was associated with concerns about smoking hazards.28,29 Furthermore, another study reported that physicians’ readiness to quit smoking was higher than that of the general population. 30 However, stress is considered a major barrier for smoking cessation, 31 which is compatible with our findings.
Although this study reported some significant associations of smoking with some sociodemographic and occupational factors, However, its limitation includes cross-sectional design as well as relatively small sample size among different categories of occupation and specialties. Thus, we recommend producing prospective studies on a large sample size.
Conclusion
Physicians can serve as role models in their community by adopting a healthy lifestyle. Despite legislation that controls tobacco use and physicians’ awareness of the health risks of smoking, this study reported a high prevalence of smoking among physicians. Epidemiological studies are required for an in-depth exploration of the attitudes and behavior of physicians who smoke and to assess the impact of their work and workplaces. Additionally, smoking usually starts in early adulthood. Thus, cessation programs should target medical students and younger physicians. In addition, specific strategies should be adapted to encourage smoking cessation among physicians, as the majority of physicians are self-dependent and seek such information from media sources.
Footnotes
Acknowledgements
We gratefully acknowledge the participation of physicians from KAAUH, KFMC, and KKUH. We also appreciate the research service center at PNU for providing valuable input in data analysis. Finally, we are grateful for the input of Dr. Eman Alshahrani, a family medicine resident at King Khaled University Hospital, KSU, for her participation in the data collection.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AA: Data interpretation and manuscript preparation. AN: Study design, data collection, and entry. EB: Study design, data collection, and entry. SN: Study design, data collection, and entry. AF: Study design, data collection, and entry. BB: Study design, data collection, and entry.
Ethical Approval/Patient Consent
The study protocol was approved by the Institutional Review Board (IRB) at Princess Nourah Bint Abdelrahman University, Riyadh, Saudi Arabia (IRB-PNU: 11061601). Written informed consent was obtained from participants. All data used in the study are available for interested researchers upon request from the corresponding author after approval from the Institutional Review Board at PNU (contact