
Abstract
Background:
Because implementation of the Framework Convention on Tobacco Control (FCTC), a World Health Organization (WHO) treaty to reduce tobacco use, is an important goal of the 2015 United Nations Sustainable Development Goals (SDGs) and Thailand has sought to fully comply with all its articles, a multiperspective assessment was developed to ensure that any gaps in compliance with FCTC provisions were identified and addressed.
Method:
One assessment mechanism of this multicomponent assessment was the development by experts and use by stakeholders of a 3-tiered rating of all major provisions of the main articles of the FCTC. The results of the performance ratings on FCTC articles by a diverse group of stakeholders were used to spotlight areas of local and regional implementation and compliance with FCTC provisions.
Results:
Implementation ratings by stakeholders generally followed the chronology of WHO priorities as reflected in the development by WHO of guidelines for the various FCTC articles with highest ratings for articles 6, 8, 11, 12, 14, 15, and 16. However, only 5 articles (Articles 6, 11, 12, 15, and 16) reached level 2 (effectiveness) of the 3-level rating; articles 6, 8, 11, 13, and 14 are discussed because they are the WHO priority articles of the MPOWER tobacco control policy. Importantly, stakeholders cited problems with lack of completeness of present Thai law and processes for enforcement, as well as lack of public understanding regarding tobacco control strategies and provisions.
Conclusions:
Overall, the breadth and inclusiveness of the stakeholder approach devised for improving implementation by the Tobacco Control Research and Knowledge Management Center provided greater understanding about shortcomings of present policy and resource management which informed the Tobacco Products Control Act passed in 2017 and plans for advancing stronger Thai regulation by local and national government.
Introduction
Implementation provides the experience that informs assessment. Without assessment, it is difficult to make sense of what is happening in any field or enterprise. 1 Measures for the assessment of tobacco control programs have improved from the past due to more and better indicators of outcomes. 2 Putting assessment into a World Health Organization (WHO) treaty of general measures dependent on the cooperation of member states is not certain to be specific enough to address all national circumstances. Therefore, many mechanisms have been used to help countries to assess the levels of implementation that have been obtained in meeting the provisions of the articles of the Framework Convention on Tobacco Control (FCTC) which was adopted in 2003 and went into effect in 2005.
The FCTC is a treaty of the WHO, which seeks to protect present and future generations from the devastating health, social, environmental, and economic consequences of tobacco consumption and exposure to tobacco smoke. The FCTC has 38 articles with certain demand and harm reduction articles which have been given primary attention in this assessment of implementation gaps in Thailand. Some 180 countries are parties to this international treaty. The 5 primary articles in this study are described in detail as follows:
Article 6 of the FCTC is on price and tax measures to reduce the demand for tobacco. This means a government tax policy incorporating the FCTC goal of maintaining the taxes on tobacco high enough to deter smoking, especially for populations susceptible to initiation of tobacco use such as youth.
Article 8 of the FCTC is protection from exposure to tobacco smoke which is known to be harmful to health. This means government adoption of laws and regulations prohibiting smoking in “indoor workplaces, public transport, indoor public places, and other public places.”
Article 11 of the FCTC is on the packaging and labeling of tobacco products. This means government should ensure that the public is informed of the dangers/harms of tobacco use and is not deceived by false or misleading packaging and labeling of tobacco products. This means the presence of health warnings on tobacco products and the absence of false descriptors or terms on such products.
Article 13 of the FCTC specifies a ban on the advertising, promotion, and sponsorship by tobacco companies of their products. This means the government limits all means of advertising and promotion, including corporate social responsibility measures designed to boost demand for tobacco products.
Article 14 of the FCTC includes demand reduction measures concerning tobacco dependence and cessation. This means governments should include some measures to assist people quit smoking. This may include one or more measures such as quit line services by phone or electronic means, cessation counseling, and/or drug treatment or other means known to be effective.
Articles 6, 8, 11, 13, and 14 are considered demand reduction measures within the 6 MPOWER policies which mean as follows: M for monitor tobacco use and prevention policies; P for protect people from tobacco smoke; O for offer help to quit tobacco; W for warn about the dangers of tobacco; E for enforce bans on tobacco advertising, promotion, and sponsorship; and R for raise taxes on tobacco. World Health Organization has developed indicators for each of the MPOWER policies and periodically assesses how FCTC signatories are meeting these indicators. 3
The FCTC implementation is a goal under the Sustainable Development Goals (SDGs). The SDGs are a set of goals adopted on September 25, 2015, at the United Nations Sustainable Development Summit in New York. Those countries agreeing to the goals embraced 17 specific goals to end poverty, protect the planet, and ensure prosperity for all. Goal number 3 focuses on health and includes using the FCTC to end the tobacco epidemic as an important part of efforts to prevent noncommunicable diseases such as cancer, heart disease, diabetes, and hypertension. 4 Increased FCTC implementation is associated with a general decline in the prevalence of tobacco use and improved health outcomes. 5
Thailand has been a leader in tobacco control in Asia since the 1990s with a declining smoking prevalence. It is now below 20% as assessed by WHO, but smoking by men is still high, whereas smoking by women is very low, <3%. However, tobacco use still contributes to the noncommunicable disease burden responsible for more than 60% of deaths in Thailand. 6 Thailand has ratified the FCTC and has achieved the highest level of attainment of several articles of the FCTC. 3 When compared with other countries in Southeast Asia on levels of implementation and the likely sustainability of tobacco control activities, Thailand has ranked very high.7,8 However, as a middle-income country, Thailand still faces limitations of fiscal and human resources for tobacco control and must devise methods to set and assess implementation goals important to fulfilling its FCTC responsibilities and domestic aims for effective and efficient tobacco control activities. In considering these responsibilities, the Tobacco Control Research and Knowledge Management Center (TRC), a research unit based at Mahidol University, Bangkok, has chosen to use stakeholder input to identify the gaps and needs for gains in tobacco control implementation of specific FCTC articles.9–11
Methodology
The TRC decided to use 3 assessment elements which included assessing research evidence, target audience attitudes and perceptions, and implementation stakeholders’ views of enforcement. In short, assessment included reviewing international research, focus group input of the target population, and a 3-tiered rating of implementation progress by stakeholders. This article focuses on the development and use of the 3-tiered scale with scoring between 0 and 3 to establish level of adequacy of implementation of 5 major articles of the WHO FCTC. The indicator categories, scaled 0 to 3, specified adequacy of implementation with 0 indicating no implementation, 1 indicating some but ineffective implementation, 2 indicating effective but inefficient implementation, and 3 indicating both effective and efficient implementation. Ratings were given by 55 tobacco control stakeholders involved in policy and implementation for 15 Articles of the FCTC, with 5 main MPOWER articles, the central focus of the assessment. These indicator levels were developed by experts in each FCTC area prior to the rating of FCTC Articles by stakeholders from various organizations directly involved with FCTC Article implementation. Experts were directed to develop specific, observable, and measurable indicators for assessing implementation success. The meeting where the 3-level indicators were explained and ratings made of each article included 40 government and 15 nongovernment stakeholders who were experienced officials with familiarity with the implementation of laws and regulations and their enforcement in Thailand. Persons included in the meeting were from the Bureau of Tobacco Consumption Control, Department of Disease Control-Ministry of Public Health, Thai Health Promotion Foundation, Action on Smoking and Health (Thailand), Food and Drug Administration Thailand, Health Department—Bangkok Metropolitan Administration, Ministry of Natural Resources and Environment, the Department of Health—Ministry of Public Health, and several other nongovernmental organizations. Following the meeting, scores were given based on participants’ views of the situation in Thailand in 2016 for each article item and then the scores were averaged for a final score for each article. Mean scores were provided as an indication of the central tendency of the ratings across the 3 levels chosen by the topic exports for each article rating scale. Confidence intervals are not given because of the qualitative nature of the scales.
In the scoring which followed the stakeholder meeting, a score of 1 meant “present but not effective,” whereas a score of 2 meant “effective but not efficient.” Finally, a score of 3 signified “highly effective and efficient” implementation. For example, for Article 8 on protection from tobacco smoke, a graduated percent of compliance was used for “effective implementation,” and for Article 11 on warning of tobacco dangers, the size and clarity of the warnings on cigarette packs were used as indications of implementation effectiveness.
Results
Figure 1 shows the mean ratings of implementation of articles of the WHO FCTC in Thailand in 2016 based on a 3-tier rating system of article items from present but not effective (1) to effective but not efficient (2) and highly effective and efficient (3).

Mean ratings of implementation of Articles of the WHO FCTC in Thailand in 2016 based on a 3-tier rating system of article items from present but not effective (1) to effective but not efficient (2) and highly effective and efficient (3).
In considering the results of using stakeholder rankings of Articles and their different provisions, it is important to be clear that this method may or may not show results consistent with an outside rating of implementation. Sometimes a ranking by implementation experts in Thailand may be very different than a ranking by an external, objective standard. For example, the MPOWER assessment for Thailand gives Thailand a high level of attainment (6 of 10) on Article 13, Tobacco Advertising, Promotion, and Sponsorship (TAPS). In contrast, the implementation ranking using the stakeholder method gave it a very low rating, not even reaching a minimal 1 ranking out of 3. This is a very pointed indication that although there may be a legal framework for stopping TAPS violations, there is a major gap in that framework and its implementation. In the case of Article 13 in Thailand, it is the lack of provisions on corporate social responsibility, online promotions, and other areas that make implementation inadequate and results in a very low implementation rating. 12
It is important to note that there are corresponding rankings for implementation on articles of the FCTC by those making them in Thailand and for implementation completion levels by other member states. This is undoubtedly true because of the order that articles were considered for guideline development by the FCTC Conference of the Parties (COP). The core demand reduction provisions of the FCTC are known to be Articles 6 to 14. For example, between 2007 and 2010, Articles 8 (2007), 11, 13 (2008) and 12, and 14 (2010) were considered and guidelines produced so that member states had specific information on how provisions might be implemented. Thus, it is not surprising that these articles have high implementation ratings both in Thailand and by other FCTC member countries.
It is clear that the priority given core demand reduction provisions would logically mean that Thailand and all other FCTC members would give attention to these articles resulting in higher implementation levels/completion. The strength of the stakeholder method is in the fact that specific provisions of the article are assessed in a graduated 3-tier rating system so as to highlight the context of implementation. This is illustrated in provisions of Articles 8 and 11, both articles with fairly high implementation ratings, but where certain provisions are rated as poorly implemented.
Article 8 on protection from exposure to tobacco smoke is an area where Thailand is rated as attaining the highest level of achievement, 100% smoke-free public places according to WHO’s report on the status of the tobacco epidemic, 2017. However, in the Thai stakeholder ratings of the detailed provisions of the article, detailed knowledge of implementation emerges which shows that present law does not adequately cover international airports and private motor vehicles and that compliance is low in some public places such as pubs and bars. This is important information for future implementation action.
Article 11 on packaging and labeling of tobacco products is another area where Thailand is rated as attaining the highest level of achievement due to its large (85%) picture health warnings and its prohibition of misleading descriptors on tobacco products. However, the stakeholder ratings in the area of information on tobacco product constituents and emissions are very low, indicating that not enough information is being provided to the public through packaging and labeling. This brings attention to the need for more evidence on constituents and emissions through testing and for this evidence to be provided to the public. Research and public policy to include more information is thus highlighted through stakeholder ratings of implementation.
The rating for Article 14 on cessation had a mean of 1.58 which was below the ratings for Article 6 (2.0), Article 8 (1.67), and Article 11 (2.0). This means that the effectiveness in providing cessation counseling and services is not complete. This is likely due to the fact that cessation programs in Thailand followed release of the WHO FCTC Article guidelines on cessation in 2010. A high level of cessation achievement in Thailand did not result until 2012 as reported by WHO. 4 Only recent WHO cessation guidelines with attention to cessation practice have resulted in some implementation gaps, a common problem when priority areas compete for resources. 13
Important lessons from the stakeholder meeting to assess implementation of FCTC Articles included that the higher ratings of implementation are consistent with WHO’s MPOWER policy assessment for Thailand with Articles 6 (Raise taxes), 8 (Protect from tobacco smoke), and 11 (Warning of tobacco harms) rated as effective (2.0 of 3.0) or somewhat effective (1.67 for Article 8). Cessation activities (Offer quitting help) were less so (1.58), with stakeholder input showing the need for better follow-up with those identified as smokers and greater availability of accessible community services as well as the Thai National Quitline.
Discussion
Overall, importance placed on certain articles as core demand reduction articles and the early role out of guidelines for these same core articles has resulted in some of the general implementation success of these items both in Thailand and for all member states. However, the specificity of looking at every provision within each article as illustrated with Articles 8 and 11 above provides an opportunity to find weak areas and to reflect and discuss how these areas might be addressed at present and when new legislation might be adopted or different provisions for monitoring and enforcement devised.
Implementation success involves many factors, but one important one is a feeling of ownership of the process of attaining the goal. It is easy to let implementation slide with a system where top-down directives predominate and local and even regional authorities have little opportunity to take responsibility and are only intermediate links in a chain of action from above. The new Tobacco Products Control Act which has just gone into effect in July 2017 provides the opportunity for decentralization of implementation on many core demand reduction measures, and the specific results of the stakeholder assessment method provide relevant input to bring local and regional actions forward for FCTC Article implementation through the new Bangkok and Provincial Tobacco Products Control Committee powers and responsibilities. 14
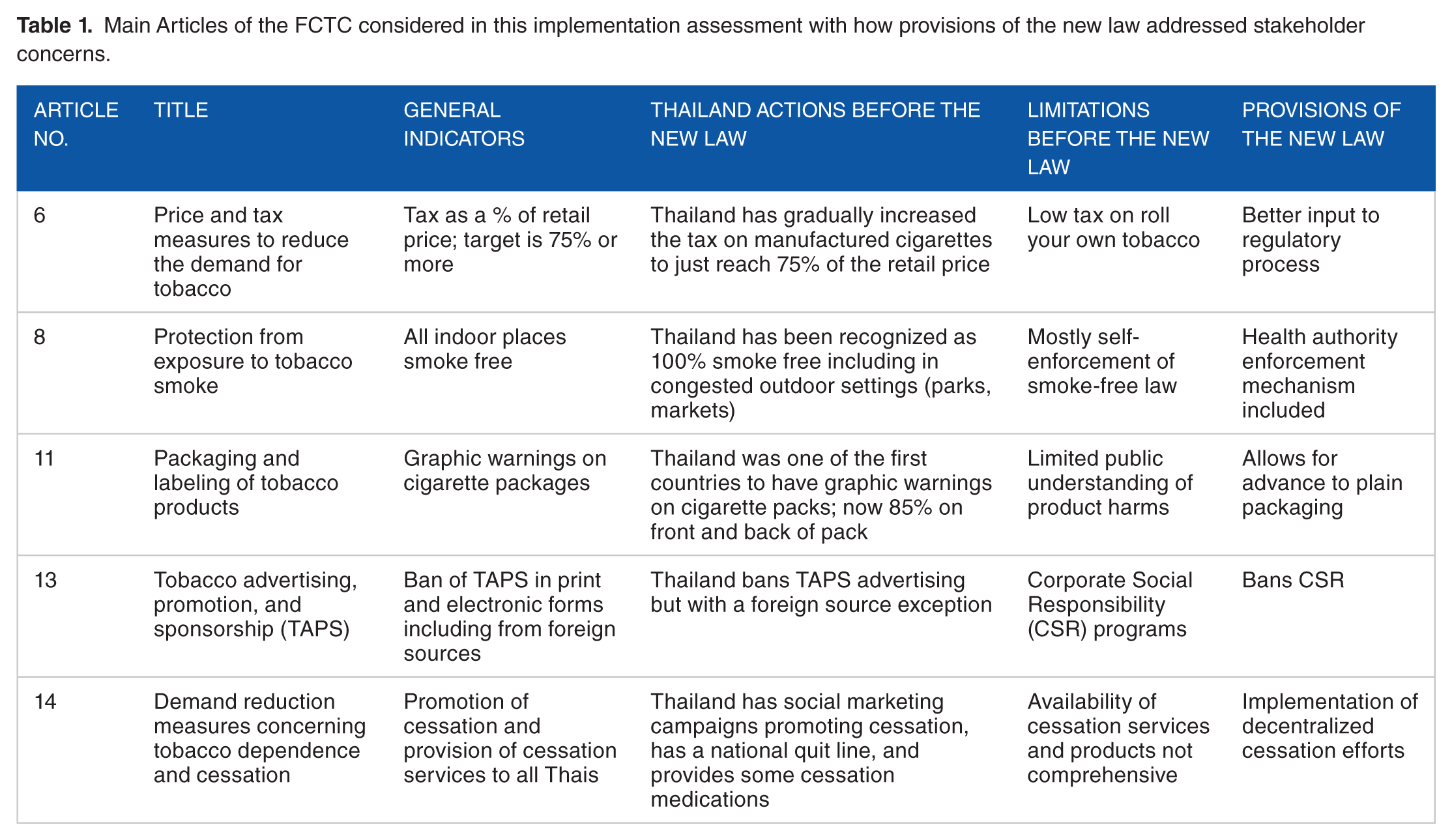
How did the stakeholder ratings help with policy implementation? Table 1 shows how the stakeholder ratings brought attention to aspects of the new Tobacco Products Act 2017.
Main Articles of the FCTC considered in this implementation assessment with how provisions of the new law addressed stakeholder concerns.
Conclusions
Overall, the breadth and inclusiveness of the stakeholder approach devised for improving implementation by the TRC is a timely addition to the ongoing process of assessing effective and efficient tobacco control activities. It promises to be particularly important as the new Tobacco Products Control Act of 2017 goes into effect, providing insight into the additional resources and infrastructure needed for improved tobacco control implementation.
What this article adds
The efforts of TRC show that multiple methods of assessment aimed at showing insight from local researchers, audiences, and implementers can result in greater understanding for implementation planning and improvement.
The Thai assessment method which captures concrete experiences of implementers clarifies accomplishments and gaps in meeting core goals of FCTC articles and can foster commitment to further progress.
Footnotes
Acknowledgements
The authors would like to thank all participants and those who were involved in the assessment process throughout.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding of this research was provided by the Tobacco Control Research and Knowledge Management Center, Bangkok, Thailand. The research was also partially supported by the China Medical Board.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SP, DS, NC and NK designed the study. Data collection by DS. Data analysis by NC and SLH. Contribution of materials and equipment by SP. All authors contributed in writing.